Efficacy and safety of acupuncture-moxibustion for cerebral palsy-induced speech impairment:a systematic review and meta-analysis
2023-06-19WANGJiahui王佳慧ZHOUTaocheng周陶成BAOChao鲍超LIJianbing李建兵SUIYuhang隋宇航
WANG Jiahui (王佳慧), ZHOU Taocheng (周陶成), BAO Chao (鲍超), LI Jianbing (李建兵), SUI Yuhang (隋宇航)
1 The Children’s Hospital of Anhui Province, Hefei 230022, China
2 Jiangsu Province Hospital of Traditional Chinese Medicine, Nanjing 210000, China
3 The First Clinical Medical College of Nanjing University of Traditional Chinese Medicine, Nanjing 210000, China
Abstract
Keywords: Acupuncture-moxibustion Therapy; Scalp Stimulation Areas; Cerebral Palsy; Speech Disorders; Randomized Controlled Trial; Meta-analysis; Systematic Review
Cerebral palsy (CP) is a term used to describe a group of perm ane nt mobility and posture abno rma lities causedbynon-progressivedisruptionsinthe developing fetus or infant brain that result in activity limitation.CP is frequently accompanied by sensory,perceptual, cognition, communication, and behavior impairments, as well as seizures and musculoskeletal problems[1].Approximately 75% of children with CP have some degrees of communication difficulty, which is mostly caused by brain damage that interferes with the language input and output system[2].A mild brain injury will result in a reduction in speech, and a serious brain injury will result in complete speech loss or aphasia[3].Dysarthria, delayed speech and language development, and hemiplegic aphasia are the most common clinical symptoms.These barriers prevent the kid from engaging in everyday social interaction activities, reducing their ability to self-care, which has a direct impact on their cognitive development, learning ability, and social skills.For speech impairment in children with CP, there is currently no specific medicine or prescription.Dysarthria treatment, delayed speech and language development treatment, neuromuscular electrical stimulation, group language training classes,acupressure massage therapy, music therapy, use of communication equipment, oral motor exercise, and guided education are some of the non-pharmacological treatment options.Although these treatments may improve speech and language skills in the near term,they do not have long-term benefit.As a result, patients are more likely to seek out other options.
Acupuncture-moxibustion therapy is regarded as a promising complementary and alternative therapy for the treatment of speech impediment.Acupuncturemoxibustion therapy has been included in the Chinese guidelines for CP rehabilitation as one of the therapeutic options that can interfere with language difficulties in children with CP.Acupuncturemoxibustion, on the other hand, is not addressed in the worldwide guidelines.A literature search revealed a plethora of published clinical randomized controlled trials (RCTs) of acupuncture-moxibustion therapy with language impairment in order to determine whether acupuncture-moxibustion is truly a safe and effective approach.The utilization of the most up-to-date evidence is at the heart of evidence-based medicine.RCT-based systematic review (SR) or meta-analysis (MA)is now widely acknowledged as the highest level of evidence[4].The published SR and MA mostly focused on the efficacy of acupuncture and moxibustion in improving motor function and sialorrhea in children with CP, according to document retrieval.Language difficulties have a scarcity of study.Therefore, we planned to undertake SR and MA to investigate the efficacy and safety of acupuncture-moxibustion in the treatment of cerebral palsy-related language problems.
1 Methods
1.1 Eligibility criteria
The included studies had to meet the following criteria.Patients with CP who met the diagnostic criteria for speech impairment were included, and the patients’age, gender, source of cases, and course were not limited; studies were designed according to RCT guidelines; according to the original document content,the trial group received acupuncture-moxibustion treatment, as well as rehabilitation techniques.Speech therapy, sports training, cognitive perception dysfunction training, sensory integration training,physical therapy, neurodevelopment promotion approaches, or other rehabilitation methods were used in the control group; the effective rate was the efficacy index.
The following were the criteria for exclusion.Studies in which the experimental group received pharmacoacupuncture, laser acupuncture, or other unusual forms of acupuncture; studies in which the experimental group received a combination of interventions with other traditional Chinese medicine therapies such as Chinese herbal medicine, acupoint injection, or herbal extracts; studies in which the required data were not available.
1.2 Data sources and search strategy
The Cochrane Database of Systematic Reviews,PubMed, Excerpta Medica Database (EMBASE), Web of Science (WOS), Chinese National Knowledge Infrastructure (CNKI), Chongqing VIP Database (CQVIP),and Wanfang Academic Journal Full-text Database(Wanfang) were searched to find relevant trials published between January 7, 2000 and January 12,2021.“Cerebral palsy”, “acupuncture”, “acupuncture therapy”, “acupuncture-moxibustion therapy”,“electroacupuncture”, “scalp acupuncture”, “ear acupuncture”, “randomized controlled trial”, “random assignment”, “clinical trial”, and “placebo”were some of the search terms utilized.These terms, as well as their synonyms, were used as free text terms for searching Korean and Chinese databases.“Cerebral palsy”,“acupuncture”, “electroacupuncture”, “ear acupuncture”and “random”, as well as “randomized controlled trial”were used as search keywords, with no language restrictions.The search strategy for PubMed is shown in Table 1.Independently, two reviewers (WANG Jiahui and ZHOU Taocheng) checked the titles and abstracts of the retrieved citations, assessed the complete texts,and determined the eligibility.Disagreements were settled by consensus or a third reviewer’s arbitration(BAO Chao).Two reviewers (WANG Jiahui and ZHOU Taocheng) independently extracted the following data:general characteristics (authors and the year of publication); baseline data (sample size, age, and gender); intervention measures, evaluation indicators,and acupuncture points.The registration number is CRD42021232482, and more information can be found on the International Prospective Register of Systematic Reviews.
1.3 Quality assessment and data analysis
The two reviewers (WANG Jiahui and ZHOU Taocheng)independently assessed the methodological quality of the retrieved trials using the Cochrane collaboration risk of bias tool.The risk of bias was assessed using the following criteria: random sequence generation (i.e.,selection bias), allocation concealment (i.e., selection bias), blinding of participants and personnel (i.e.,performance bias), blinding of outcomes assessment(i.e., detection bias), incomplete outcomes data (i.e.,attrition bias), selective reporting (i.e., reporting bias),and other biases, according to the Cochrane handbook.Each category’s bias risk was rated as high, low, or uncertain, and the differences were settled by consensus or discussion with a third party.
(a)句中,they代指其前的cats,即cats→they,此处的衔接手段为前照应;(b)句中,This代指后面的整句话,即this→I will telephone Anna and explain,此为后照应。
Data were analyzed using Review Manager Software 5.3.0 (Cochrane Collaboration, Oxford, UK).With a 95%confidence interval (CI), the results were expressed as a relative risk (RR) or mean difference (MD).The heterogeneity was assessed using the Chi-square test[5],with a detection level of 0.1.TheI2value was then used to estimate the degree of heterogeneity: a fixed effects model was used for combined analysis.I2≤40%indicated that there was no significant statistical heterogeneity.I2>40% but <75% revealed statistical heterogeneity, and the source of the heterogeneity must be investigated further.A random effects model was utilized for combined analysis if there was no clear clinical heterogeneity.I2≥75% indicated high heterogeneity, and descriptive analysis was used instead of advocate merging.
2 Results
2.1 Results of literature search and selection
The original search yielded 904 possible studies, 295 of which were eliminated due to duplicate citations.Another 323 publications were eliminated after titles and abstracts were screened.After reading the complete text of the remaining studies, we eliminated another 269 records.Finally, we included 17 RCTs[6-22]that matched the qualifying criteria in our review(Figure 1).
2.2 Characteristics of the included trials
Seventeen RTCs were included in the review.All 17 papers were published in China and written in Chinese,and the total number of patients was 1 238 (623 in the treatment group and 615 in the control group).The trials were published between 2006 and 2020, with sample sizes ranging from 30 to 111 and ages ranging from 1 to 10 years.Table 2 lists the features of the studies that were included.
2.3 Risk of bias and methodological quality
On the risk of bias, 17 articles were summarized.See Figure 2 and Figure 3.Despite the fact that all studies were properly randomized, there were only 4 technically appropriate (random number table)[11,15-16,19].Only one study[15]mentioned allocation concealment,patient and employee blinding, and outcome assessment blinding.In these 17 articles, the risk of bias from selective reporting was unknown.

Figure 1 Flow chart of the literature selection process
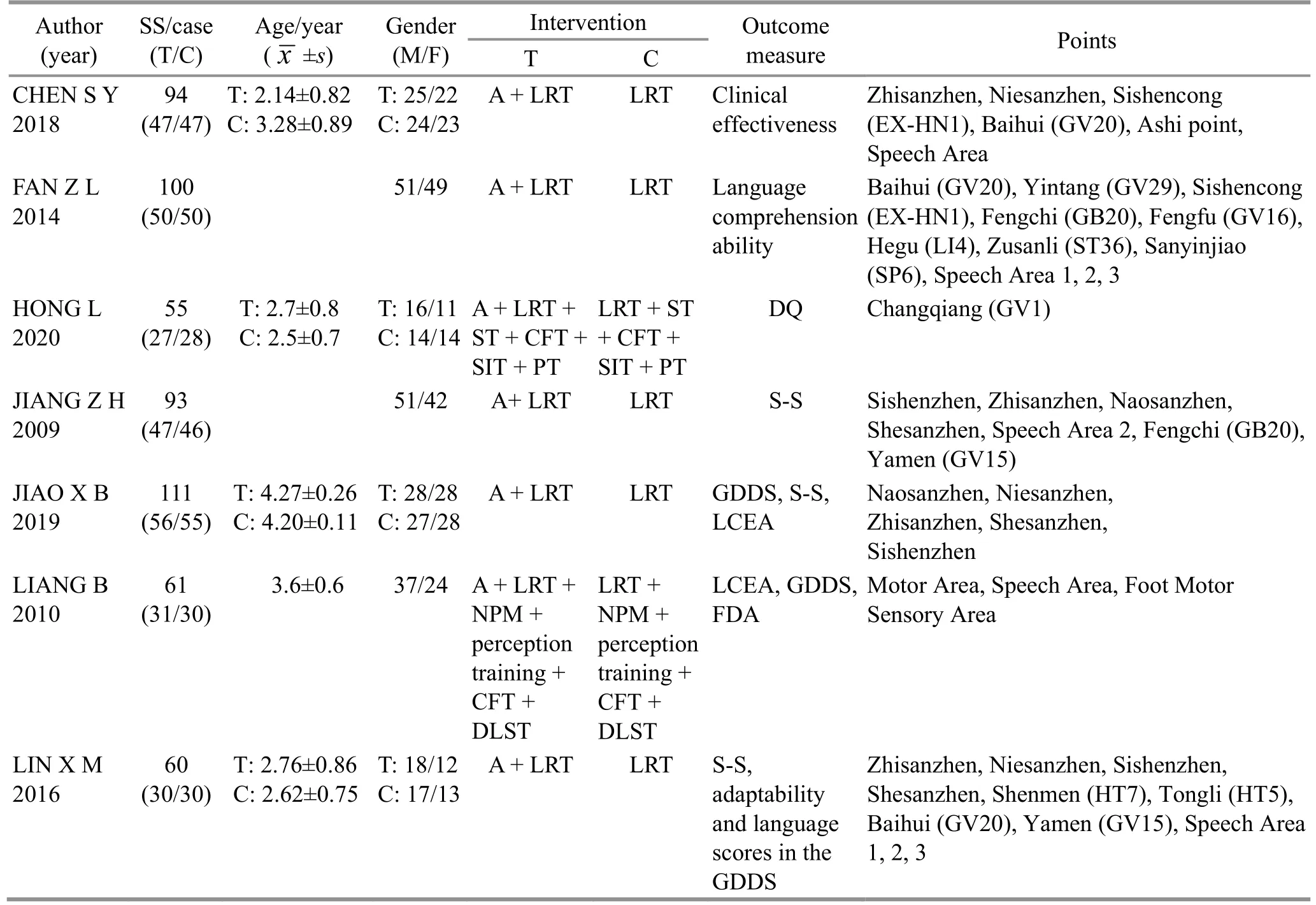
Table 2 Characteristics of the included studies
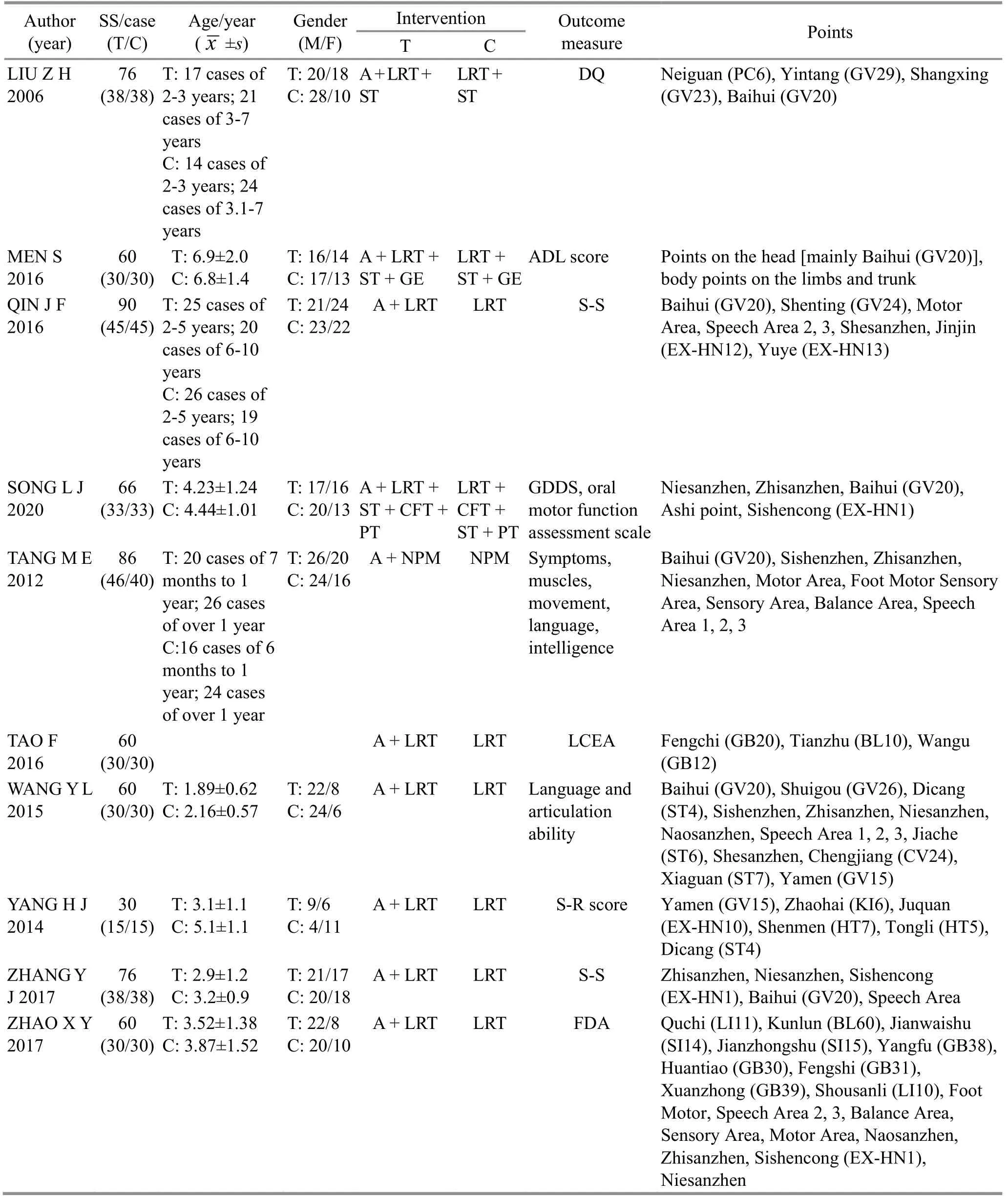
Table 2 Characteristics of the included studies (continued)
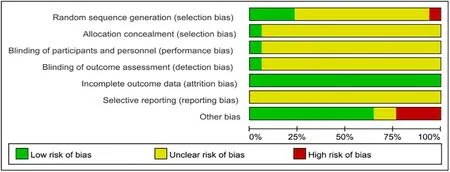
Figure 2 Ratio of risk of bias in the included studies
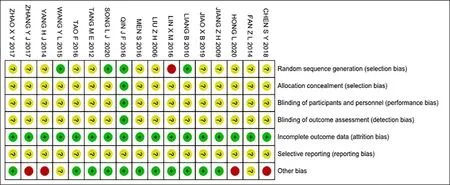
Figure 3 Assessment of risk of bias in the included studies
2.4 Primary outcome measure: total effective rate
The effectiveness in these 17 trials was documented,involving 623 people in the treatment group and 615 in the control group.This meta-analysis included these 17 RCTs to investigate the efficacy of acupuncture in the treatment of speech impairment in CP patients.The overall effective rate was calculated as follows: Total effective rate = (Total number of patients - Number of patients who did not respond) ÷ Total number of patients.After treatment, “no reaction”means there was no significant progress in any component of language development.For meta-analysis, the random-effects model was utilized.This meta-analysis demonstrated that patients who received acupuncturemoxibustion combined with rehabilitation training benefited much more than those who received rehabilitation alone, as shown in Figure 4 [RR=1.23,95%CI (1.16, 1.30),P<0.00001,I2=0%].However, the left and right of the funnel plot is asymmetry, suggesting a certain publication bias (Figure 5).
2.5 Second outcome measures
2.5.1 Gesell score of developmental quotients (DQ)
DQ was evaluated in 6 trials.The analysis of random effects model showed that patients who received acupuncture-moxibustion combined with speech rehabilitation training improved their DQ scores much more than those who received simply rehabilitation training [inverse variance=9.63, 95%CI (4.60, 14.66),P<0.00001], (Figure 6).There was considerable heterogeneity in the result (P=0.0002,I2=95%).Figure 7 shows that the left and right sides are essentially symmetrical, indicating no noticeable publishing bias.The heterogeneity was reduced from 95% to 0% by eliminating a trial[11].After deletion, acupuncturemoxibustion combined with rehabilitation training improved their DQ scores much more than those who received rehabilitation training alone [inverse variance=11.46, 95%CI (10.24, 12.68),P=0.82], (Figure 8).According to sensitivity analysis, the source of heterogeneity could be attributed to the fact that the study only used scalp acupuncture as an intervention and that the intervention time was much retarded after the commencement.Figure 9 shows that there was no noticeable publishing bias.When one study was given too much weight, sensitivity analysis was performed by adjusting the effect size.The outcome remained unchanged, showing a degree of consistency.However,the heterogeneity cannot be eliminated by changing the effect size (Figure 10).
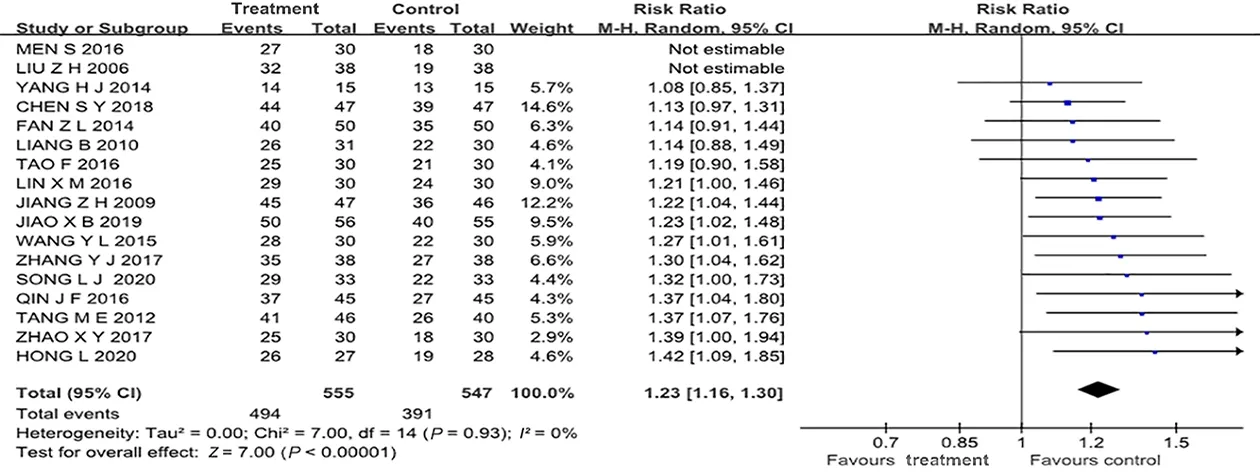
Figure 4 Forest plot for the effective rate
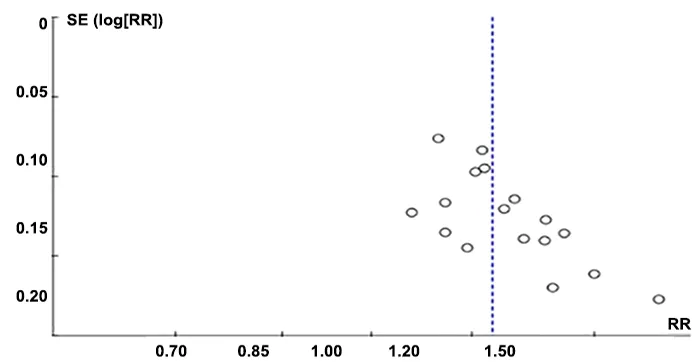
Figure 5 Funnel plot of the effective rate
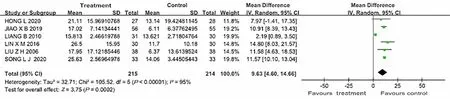
Figure 6 Forest plot for Gesell score of DQ in 6 studies
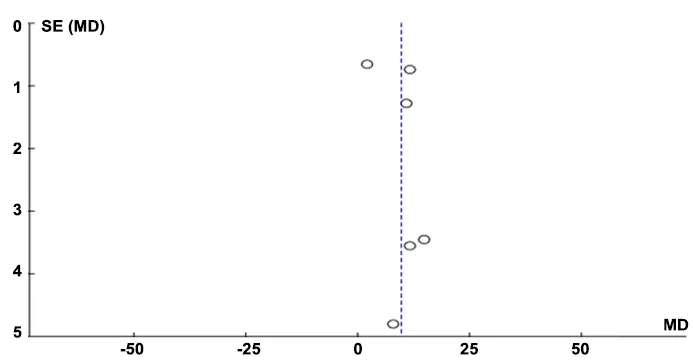
Figure 7 Funnel plot of Gesell score of DQ in 6 studies
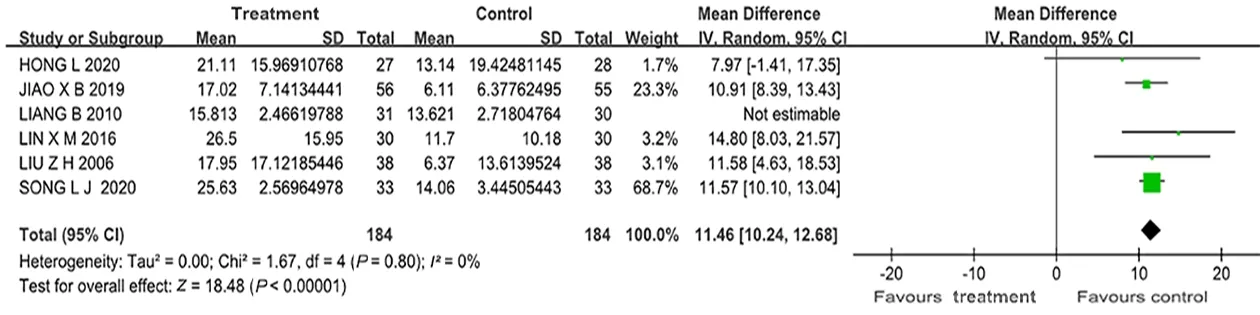
Figure 8 Forest plot for Gesell score of DQ in 5 RCTs

Figure 9 Funnel plot of Gesell score of DQ in 5 RCTs

Figure 10 Forest plot for Gesell score of DQ in 5 RCTs (sensitivity analysis by changing effect size)
2.5.2 Adverse events
3 Discussion
3.1 Analysis of efficacy
Overall, this systematic review found that when acupuncture-moxibustion was combined with rehabilitation training, the effect on speech impairment in children with CP improved significantly more than when rehabilitation training was given alone.At the same time, the level of intelligence of children with CP improved significantly.Furthermore, we discovered significant improvements in gross motor abilities, fine motor skills, flexibility, personal social interaction, and self-care capacity[8,10,12,16-17].This clearly shows that acupuncture-moxibustion has no therapeutic limitations in the treatment of CP because it can affect a broader spectrum of symptoms.On the other hand, the results[12,19]revealed that the efficacy and prognosis of acupuncture-moxibustion for speech impairment induced by CP were closely connected to the existence and severity of mental retardation.The majority of children with athetosis or ataxia type of CP have normal IQ but dysarthria as a symptom.Acupuncturemoxibustion has a high rate of success for these patients.Children with spastic CP often have varying degrees of intellectual disability, as well as reduced learning and comprehension skills and cognitive abilities.As a result, the clinical efficacy of acupuncturemoxibustion in these individuals is unsatisfactory.Acupuncture efficacy is also influenced by factors such as the time of intervention and age[12,15,19].Early acupuncture-moxibustion intervention is expected to lead to improved therapeutic success, according to studies; nevertheless, these papers differed in their views on age but age is believed to be the window of opportunity.Furthermore, the mechanism of acupuncture-moxibustion is still a mystery.Acupuncture-moxibustion can prevent the chain reaction of lipid peroxidation following cerebral hypoxia-ischemia by inhibiting the harmful effects of excitatory amino acids, regulating calcium homeostasis,and preventing calcium overload in nerve cells,according to animal studies[23-24].The anti-apoptotic effect is caused by the activation of apoptosis genes and the encouragement of anti-apoptotic gene expression.Furthermore, after acupuncture-moxibustion treatment,the levels of noradrenaline, dopamine, and 5-hydroxytryptamine in the brain tissue of juvenile rats with CP increased dramatically.A putative mechanism of acupuncture-moxibustion in treating CP in young rats could be raising the content of monoamine neurotransmitters in critical brain tissue[23].Acupuncture-moxibustion can also enlarge and widen the vertebral-basilar artery, as well as establish cerebral collateral circulation, resulting in an increase in cerebral blood flow, the restoration of ischemia-hypoxia, and the healing of brain tissue[25].
3.2 Strengths and limitations
The non-verbal functions, such as motor function,aberrant posture, intelligence, and salivation, are almost entirely ignored in the systematic analysis of acupuncture-moxibustion treatment for CP.This study compensates for the lack of acupuncture-moxibustion in the treatment of CP speech impairments and provides evidence-based support for the use of acupuncture-moxibustion in this field.There are some drawbacks in this study.Some studies may be missed,resulting in sample bias, because we exclusively looked for papers in English and Chinese databases.Furthermore, the sample size of this study is limited,and there is variability in the control group due to the lack of recognized placebo control, which may impair the accuracy of the evaluation.Due to a lack of blinding between the subjects and researchers, the methodology of the selected studies was often incorrect, which means that the results will inspire more optimistic expectations, potentially amplifying the effects of acupuncture.Because the included trials only observed the short-term and mid-term benefits of acupuncture-moxibustion combined with language rehabilitation training, future research should focus on the long-term effects of acupuncture-moxibustion therapies on speech impairments in CP.Other high-quality randomized trials and MA are needed for future reference to evaluate whether acupuncturemoxibustion combined with rehabilitation training is more effective than language rehabilitation training alone.
4 Conclusion
In summary, our findings suggest that acupuncturemoxibustion is a safe and effective treatment for speech disability caused by CP.The most commonly used points for speech disorders are Baihui (GV20), Speech Area,Zhisanzhen, Niesanzhen, and Sishenzhen.To overcome the limitations of small number of RCTs, lack of long-term impact, publication bias, and low methodological quality, more research is needed.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was partly sponsored by the Construction Project of Inheritance Studio for National Famous Chinese Medicine Specialists (全国名老中医专家传承工作室建设项目, No.2016-42); Development Program (Social Development) Project of Jiangsu Provincial Department of Science and Technology (江苏省科技厅社会发展面上项目, No.BE2017769); Natural Science Foundation of Nanjing University of Traditional Chinese Medicine (南京中医药大学自然科学基金, No.XZR2021002);Postgraduate Research & Practice Innovation Program of Jiangsu Province (江苏省研究生培养创新工程研究生科研与实践创新计划, No.SJCX21_0771).
Data Availability
The data used to support the findings of this study are available from the corresponding author upon request.
Received: 2 July 2021/Accepted: 30 September 2022
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Electroacupuncture stimulation attenuates corpus striatum white matter injury in rats with cerebral ischemia by inhibition of Nogo-A/NgR pathway
- Study on the antipyretic mechanism of large pushing Tianheshui for young rabbits with endotoxin-induced fever
- Effects of different moxibustion time on knee cartilage morphology and the expression of TNF-α and IL-10 in rats with knee osteoarthritis
- Effects of horse-riding squat exercise plus Governor Vessel-regulating Tuina therapy on static balance function in patients with stroke
- Observation on the efficacy of traditional Qigong exercise combined with Tuina manipulations in treating lower cervical disc herniation
- Clinical study of treating somatoform pain disorder with the combination of electroacupuncture and duloxetine