A systematic review of reading tests
2023-02-11PanagiotaNtontiChristinaMitsiEleftheriosChatzimichaelEiriniKanellaPanagiotopoulouMinasBakirtzisAristeidisKonstantinidisGeorgiosLabiris
Panagiota Ntonti, Christina Mitsi, Eleftherios Chatzimichael, Eirini-Kanella Panagiotopoulou,Minas Bakirtzis, Aristeidis Konstantinidis, Georgios Labiris
Ophthalmology Department, University Hospital of Alexandroupolis, Dragana 68100, Alexandroupolis, Greece
Abstract
● KEYWORDS: digital reading chart; paper reading chart;presbyopia; low vision chart; reading acuity
INTRODUCTION
Adequate visual capacity is essential for the adaptation to the environment, contributing to our better perception of the world. All modern activities of daily living are vision‐intensive. Adequate vision imposes no limits to the social,professional and personal objectives of the patient; within this context it should address tasks in the near, intermediate, and distant environment[1].
Current social and professional mandates, require perfect or almost perfect near and intermediate visual capacity, since the use of computers, tablets, and smartphones is an integral part of our lives.
Reading comprehension is defined as the ability to process text, to understand its meaning and to integrate with what the reader already knows. However, several factors interfere with reading capacity with the most prevalent one being presbyopia[2].
Presbyopia is the outcome of the age‐related elasticity changes in the crystalline lens and its capsule. It manifests as a reduction in the amplitude of accommodation accompanied by inability of the longitudinal muscle fibers of the ciliary body to contract efficiently[3‐7]. Prevalence of presbyopia is predicted to reach 1.8 billion by 2050[8‐10].
Further to presbyopia, a series of other conditions interfere with normal intermediate and near visual capacity. Among them are cataract, age‐related macular degeneration (AMD),glaucoma, and systemic diseases that affect the physiology of the retina such as diabetic retinopathy (DR) and hypertension[2].It becomes obvious that since the reduction of the intermediate and near vision is associated with numerous ocular and systemic diseases, the evaluation of the reading capacity of the patient is part of the routine ophthalmological examination both for adults and adolescents. However, no common methodology exists in the quantification of reading capacity. A series of reading tests have been developed, both printed and digital, which introduce reading parameters that are supposed to reflect reading capacity.
Within this context, primary objective of this study was to conduct a systematic review on all available reading tests both conventional and digital and explore their integrated characteristics.

Table 1 Study design
MATERIALS AND METHODS
This systematic review followed the Preferred Reporting Items for Systematic Reviews (PRISMA) statements checklist.Study design adopted the mandates of the Problem/Population,Intervention, Comparison, Outcome (PICO) framework. PICO framework defined the selection criteria. Participants included patients with near distance reading difficulties before or after cataract surgery. The studied reading tests included both normal vision populations and low vision patients. Intervention consisted of cataract surgery or reading glasses. Some of the surveys compared digital reading charts with conventional ones. Outcome concerned the accordance between digital and paper reading charts and their application in everyday life and clinical routine.
The systematic search for relevant studies was performed by two independent reviewers based on PubMed, Google Scholar and Springer databases using the following search terms:digital chart AND paper chart, reading acuity (RA), presbyopia AND digital chart, computer AND reading test, reading chart AND near vision AND electronic devices AND low vision chart.
The search was conducted between February and March 2021. Search filters and language restrictions were not used in the initial search. The results were checked and only articles with titles relative to the subject were selected. Both comparative and descriptive studies were included in this review. Articles not available in English, French or German were excluded. When the eligible articles were not available in full text, abstracts were used as a source of information.Year of publication ranged from 1980 to 2020. All potential conflicts on the review process were resolved by a third senior reviewer (Labiris G). This article refers to a literature review that uses published data so it is not required to be approved by a Scientific Board.
RESULTS
Totally 35 articles (11 descriptive studies and 24 comparative studies) were included in the present systematic review(Table 1). Among them, 21 were prospective studies. Nine of the comparative studies dealt with digital charts, while eight studies studied near vision and its characteristics. Three of the studies compared different typed charts for near vision[11‐48]. A PRISMA flow chart is demonstrated in Figure 1.
Reading ParametersThe following are the most commonly used parameters in the assessment of reading capacity as suggested by the articles that were included in our systematic review.
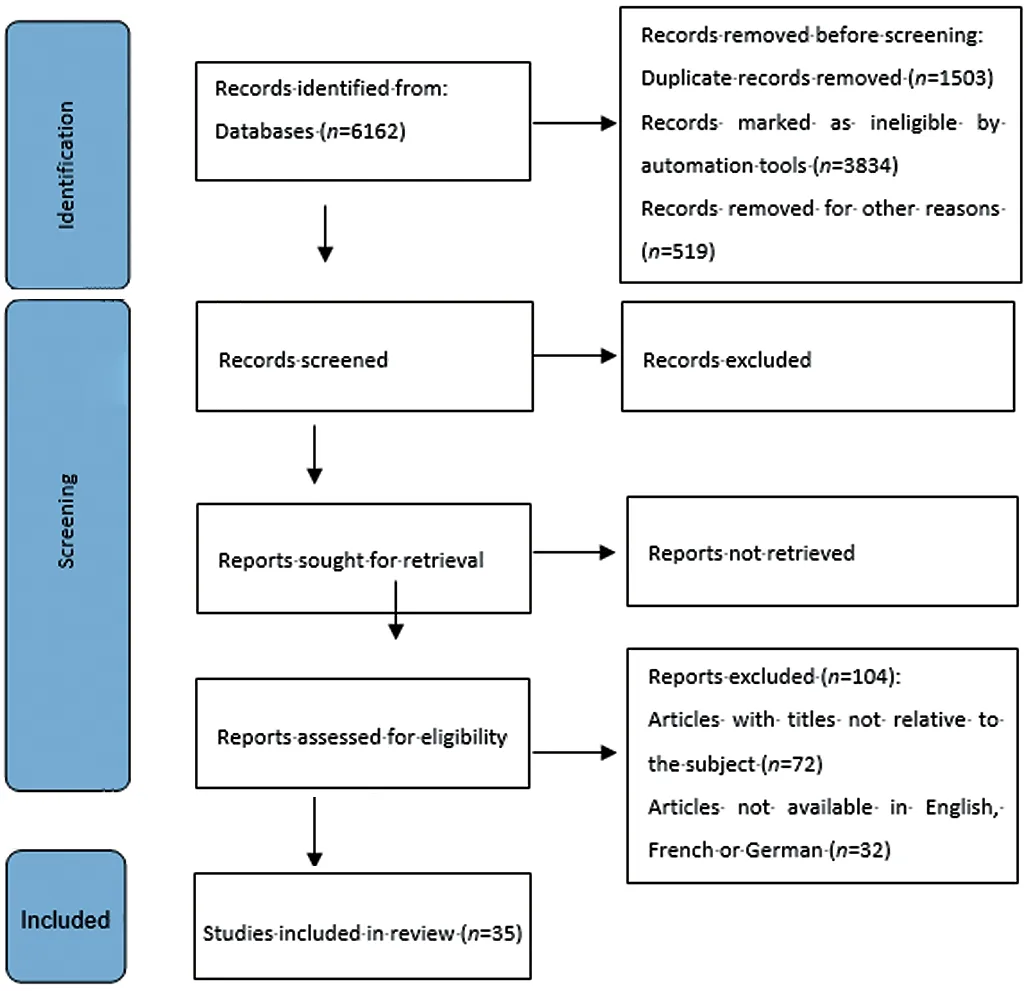
Figure 1 PRISMA 2020 flow diagram for new systematic reviews.
Reading speedReading speed (RS) [in words per minute(wpm)]=60×(10-errors)/(time in seconds), where errors is the number of mistakes made by the patient in the current sentence and time (in seconds) is the patient’s reading duration of the current sentence[11‐15]. However, certain differences in the measuring methods were identified in the assessment of RS.Rhiuet al[14]calculated RS as letters per minute. Participants were asked to first read silenty and then aloud the sentences in question and they measured reading‐only and reading‐and‐speaking speed. Hirnschallet al[18]did not take into consideration errors that were made while reading and patients were asked to read continuously without pausing. They also excluded sentences read with a reading speed less than 80 wpm from the statistical evaluation, stating that the reading speed of 80 wpm is the minimum to allow comprehensive recreational reading.
Reading acuityRA is defined as the smallest print that the patient can read without making significant errors,calculated by the following formula: RA (logMAR)=1.4-(sentences×0.1)+(errors×0.01) for the MNREAD and IUREAD charts[12,15]whereas for the Radner charts it is calculated by:log reading acuity determination (logRAD) score=logRAD for lowest line read+(0.005×syllables of incorrectly read words). Threshold RA was determined as the last sentence that could be read completely[13]. For the LPO Rosenbaum pocket screener, RA was recorded based on the last line for which all letters were correctly identified[16]. For the ETDRS chart,results were recorded by the examiner based on the smallest line for which four or more charts were identified correctly measured in logMAR[17].
Maximum reading speedMaximum reading speed (MRS)measured in wpm, is defined as the patient’s reading speed when reading is not limited by print size, and calculated by averaging the reading speed of the sentences with print size larger than the Critical Print Size (CPS)[12‐13,15].
Critical print sizeCPS measured in logMAR, is defined as the smallest print size sentence that can be read with reading speed greater than or equal to the average reading speed of the larger logMAR print sentences minus 1.96 times the standard deviation (SD) of the reading speed of these sentences[15].Hirnschallet al[18]defined this parameter as the smallest log‐scaled print of lowercase letters read with a speed of more than 80 wpm and it was expressed in mm.
Reading accessibility indexReading accessibility index(ACC) is defined as the mean reading speed of the 10 largest print sizes of the MNREAD acuity chart at 40 cm(1.3 to 0.4 logMAR), divided by 200 wpm, which is the mean reading speed of normally sighted young adults aged 18 to 39 years old.
Our review indicated that for the reliable measurement of reading parameters certain precautions should apply.
Memorization controlMemorization was avoided by using different chart and sentence sets for all trial runs[15]and by randomizing the order of the chart used first (printed or electronic)[13,16‐18]. In addition, a large number of sentences,randomly selected for each trial, was employed[12].
Distance monitoringFor digital application of reading charts, various methods that measure distance between the patient and the screen were utilized to minimize interference with true visual capacity metrics. Participants’ pupillary distance (PD) was monitored by a face‐tracking algorithm within the iPad app to ensure minimal distance change. When a ±4 cm deviation was detected, there was a warning to readjust the distance and retake the test[41]. Hirnschallet al[18]did not set a constant reading distance for their experiments but let the patients choose it, while measuring it with video stereophotogrammetry. Other studies monitored distance with the help of an examiner[13]using a tape meter and close observation[16‐17]for both printed and digital charts.
Time measurementRegarding printed versions, all studies timed the process with a stopwatch controlled by examiners[12‐13,15,18]. It is believed that the examiner’s response time from the time the patient starts reading until they press the stopwatch button can overestimate reading speed, thus creating the need for more automated methods. The subject’s voice was recorded by microphone and an in‐app stopwatch measured reading duration from text presentation to whenever the patient pressed the stop button[13,18]. The examiner could visually inspect recordings to mark the start and end of sentences[12].For the MNREAD application, a touch on the screen set the timer on simultaneously with the presentation of sentences,while a second touch stopped it, automatically recording reading time[15].
Error managementIn printed charts, error trapping is done by the examiner. Certain digital charts offer the option of voice recording in order to confirm potential errors by the patient[12‐13]. In the MNREAD app, a screen appeared after each sentence for the examiner to appoint the number of errors[15].Reliable reading assessment with digital reading tests heavily depends on the specific characteristics of the display. These characteristics are[19‐21]:
Gamma functionThis is a mathematic function that was used to derive the potential range of display of contrast targets on the devices. L=νγ were L represents the luminance of the display, ν is the signal voltage and γ is the slope of the line of best fit in a log(L) versus log(V) function (gamma).
LuminanceLuminance is a measure of luminous intensity of light travelling in a given direction, per unit area. The SI unit for luminance is candela per square meter (cd/m2). In real‐life positioning, luminance can differ between central and peripheral targets at different screen locations on a tablet display. Battery level can also affect luminance levels[20].Nearby light sources could also affect luminance, not so much at perpendicular viewing, but when there is screen rotation of a certain degree[21].
ContrastThe contrast ratio (CR) is a property of displays,defined as the ratio of the luminance of the brightest color(white) to that of the darkest color (black). The higher the CR,the better.
Stability of displayIt is important to determine the time it takes to reach within 1% variation of the final luminance value for a certain display in order to better control and standardize display settings. There have been a few studies mostly on tablet displays, but again research was limited on certain device models. For the iPad 3 the results for the time needed for display stability varied after the switched‐off state, ranging from 15 to 1min. Therefore, 15min of screen function was advised before conducting tests with the device[19]. It took approximately 13min for the iPad mini Retina display to reach within 1% variation of the final luminance value[20]. As for the Google Nexus 10 and the Galaxy Tab 2 10.1, the longest it took the screen to stabilize was after 24h of switched‐off state and was 10 and 8min respectively[21].
Screen resolutionConsidering that the most common reading distance is typically 33–40 cm, higher resolutions would allow for 6/6 or even 6/5 vision testing. Regarding tablets, Tahiret al[21]suggest that for satisfactory vision testing a screen resolution of at least 100 pixels per cm is needed. Lower pixel densities, such as less than 132 ppi, 1024×768 pixels have been linked with a small, but nonsignificant decrease in reading speed when compared to reading a printed book[15].
Conventional Reading ChartsStandardization of the conventional reading charts begun 20 years ago, focusing primarily in clinical settings. Standardization process included the evaluation of the reproducibility, comparability, validity,interpretation and reliability of each reading test[22‐23].
Nowadays, numerous reading tests are in clinical use, with the majority of them untested for their validity. The prevalent Jaeger reading charts that are used in clinical settings are not standardized[24]and do not address the criteria established by the International Council of Ophthalmology (ICO) or the EN ISO 8596 directive[24‐26]. These standards include a logarithmic progression of print sizes, the calibration of test conditions, chart design, the specification of the distance test at all instances, the use of continuous text and a typeset material where the height of lower‐case formats is at five minutes of arc. The following conventional printed reading tests comply with the ICO recommendations: the Sloan Reading Cards, the Bailey‐Lovie Word Reading Charts, the MNREAD charts,the RADNER Reading Charts, the Colenbrander Continuous Text Near Vision Cards, the Smith‐Kettlewell Reading Test(SKread), the Oculus Reading Probe II, the C‐Read Charts and the Arabic‐BAL Chart[24,26‐28].
Sloan reading cards: They use continuous text paragraphs with a variable length sizes. The smallest print size corresponds to a decimal acuity of 0.4 at the distance of 40 cm. Progression of print size is logarithmic.
The Bailey‐Lovie Word Reading Charts: Uses unrelated words arranged in a logarithmic progression of size while each group of words is of approximately equal difficulty[29].
The MNREAD charts: This test is comprised of 60 characters including spaces, with a period at the end of a three‐line sentence. They are suitable for low vision patients, as well[11].The RADner reading charts: This test includes a series of comparable sentences that consist of 14 words in three lines,27–28 characters per line and 22–24 syllables. Word length,position of words, number of characters, lexical difficulty,and linguistic characteristics are on a par with each other. The Radner Reading Charts are available in German, Spanish,English, French, Dutch, Italian, Swedish, Danish, Portuguese,Turkish, Hungarian, and Romanian, and further languages are in progress[30].
The Colenbrander Continuous Text Near Vision Cards: The sentences used have 44 characters including spaces and a different number of words, nine to 11 words. They are translated in 12 languages[32].
The Smith‐Kettlewell Reading Test (SKread): Each test paragraph contains six single letters and ten random words with 60 characters including spaces in total but the number of words is equal in all paragraphs[31]. The Smith‐Kettlewell Reading Test was introduced to test the performance of low‐vision patients, to locate scotomas and determine their magnification needs[32‐33].
The Oculus Reading Probe II: It uses text from a book by Sven Hegin and from The Jungle Book by Rudyard Kipling. It also includes symbols of music, Landolt rings, and tumbling Es and is available in German[32].
Eschenbach and Zeiss reading tests using long sentences also try to test low vision patients, while the Keeler Reading Test Types test speed and fluency of patients with low‐vision[30].The C‐READ consists of three charts. Each chart consists of sixteen 12‐character simplified Chinese sentences crafted from first‐ to third‐grade textbooks[27].
Digital Reading ChartsConsidering the rapid development of today’s technology, numerous electronic devices are within reach for more and more people. Adequate visual ability is essential for a good quality of life and a medium of self‐assessment could further improve patients’ daily living[34].Smartphones and tablet devices with high‐definition screens are capable to host digital reading tests that could be used for self‐examination, as well[35]. However, the evaluation of the digital reading tests and near‐vision acuity charts is required prior to their introduction in clinical settings. Yeunget al[47]recently reviewed all available digital visual acuity charts that supported self‐examination. From a total of 42 digital charts, 20 were based on conventional printed charts and only 4 of them were validated. Lewis and Smith[35]developed the first digital chart, that tested visual acuity using Arabic numbers, displayed to light‐emitting diode (LED) or liquid crystal display (LCD) type numerals and was comparable in difficulty to Snellen letters. Their digital test was able to measure the visual acuity of young and healthy individuals and store their outcomes into a computer[35]. The RAD‐RD©is an automated computer program based on the RADNER reading charts that was developed to assess reading speed and reading acuity. It uses a computer and a microphone that records readers’ voice and automatically determines the start and end of vocalization[46]. The Salzburg‐Advanced is an electronic reading desk that can assess patients with AMD, DR and multifocal or accommodating intraocular lens. It can simulate a natural reading environment and calculate near or intermediate vision and reading speed at different illumination and contrast conditions. It is available in 10 languages[18]. The MNREAD test also underwent a digital transition, simplifying and standardizing testing methods, automating scoring methods,providing easy data sharing and increasing portability, with several test versions available on a single device. MNREAD allows high accuracy near vision testing by measuring CPS and Reading Acuity[36]. The IURead can be performed on a computer, tablet or mobile phone in order to test reading speed and reading acuity. It can be used for research purposes as it has 422 single sentences and can provide multiple repeats without reusing sentences and is also useful for low vision patients and presbyopes[12]. The Democritus Digital Acuity Reading Test—DDART is a web‐based reading test that requires no installation to a local computer. It provides text size calibration, automatic reading timing due to audio recording and automatic calculation of RA, MRS, CPS and ACC[37]. Rhiuet al[14]selected sixty‐three Korean sentences, adjusted them to match the design principles of the MNREAD chart and tested reading speed binocularly in a population with normal vision at 40 cm. A 3rdgeneration retina display iPad on maximum brightness was used to display the sentences. The app included a stop clock to automatically calculate reading speed in letter per minute and words per minute.
DISCUSSION
Our systematic review attempted to contribute to the body of knowledge on the present status of reading assessment.As mentioned above, reading capacity reflects near and intermediate vision capacity which is necessary for the citizen in the 21stcentury, as the majority lead a busy lifestyle with tasks that require adequate vision at all distances. Therefore, it is essential to find the most suitable means of examination that is reliable, efficient, reproducible and not time consuming.
Conventional printed reading charts still dominate in clinical settings, however the most prevalent of them (i.e., Jaeger type charts) are not validated and their outcomes should be interpreted with caution. Reliable reading capacity assessment is done only by the printed reading tests that comply with the ICO recommendations: the Sloan Reading Cards, the Bailey‐Lovie Word Reading Charts, the MNREAD Charts,the RADNER Reading Charts, the Colenbrander Continuous Text Near Vision Cards, the Smith‐Kettlewell Reading Test(SKread), the Oculus Reading Probe II, the C‐Read Charts and the Arabic‐BAL Chart[24,26‐28].
Digital reading tests are gaining popularity both in clinical and research settings since they offer reliability and ease of use. Furthermore, some can also be used from the safety of one’s home and are easy to undertake and evaluate without the presence of an examiner being necessary. However,devices on the market are numerous with varying display qualities and standards which makes it difficult to evaluate and compare results from different devices. All screens require a precise standardization of the luminance, which needs time to constantly change and calibrate. Therefore, certain precautions should apply both in the examination procedure and the characteristics of the digital display. Digital reading charts are differentiated in standard computer‐based applications that require installation either in a computer or a tablete.g.,Advanced VISION Test and web‐based onese.g., DDART that require no installation. It becomes obvious that web‐based reading tests offer the advantage of functionality independent of the underlying hardware and consume minimal resources in the host computer.
Taking into consideration the advances of modern technology and the need for time‐saving and standardized tests to aid clinical work, it seems that validated digital reading tests(computer‐based and web‐based ones) are set to prevail in clinical and research settings. All digital reading tests that were presented in this systematic review demonstrate adequate validity, reliability, and ease of use. It is upon the ophthalmologist’s personal point of view to select the most compatible one with the clinical or research setting it is used for.
ACKNOWLEDGEMENTS
Conflicts of Interest:Ntonti P,None;Mitsi C,None;Chatzimichael E,None;Panagiotopoulou EK,None;Bakirtzis M,None;Konstantinidis A,None;Labiris G,None.
杂志排行
International Journal of Ophthalmology的其它文章
- Visual perception alterations in COVID-19: a preliminary study
- COVID-19 pandemic impact on ocular trauma in a tertiary hospital
- Apolipoprotein A1 suppresses the hypoxia-induced angiogenesis of human retinal endothelial cells by targeting PlGF
- Comparison of vegetable oils on the uptake of lutein and zeaxanthin by ARPE-19 cells
- Identifying a novel frameshift pathogenic variant in a Chinese family with neurofibromatosis type 1 and review of literature
- Recurrence risk factors of intravitreal ranibizumab monotherapy in retinopathy of prematurity: a retrospective study at one center