Palliative care needs and symptom burden in younger and older patients with end-stage renal disease undergoing maintenance hemodialysis: A cross-sectional study
2022-11-05XuefeiWngQiuyinShiYongzhenMoJingLiuYingyingYun
Xuefei Wng ,Qiuyin Shi ,Yongzhen Mo ,Jing Liu ,Yingying Yun
a School of Nursing,Department of Medicine,Soochow University,Suzhou,Jiangsu,China
b Zhongda Hospital Affiliated to Southeast University,Nanjing,Jiangsu,China
c Jiangsu Province Official Hospital,Nanjing,Jiangsu,China
d Nanjing BenQ Medical Center,Nanjing,Jiangsu,China
Keywords:End-stage renal disease Hemodialysis Needs assessment Palliative care Quality of life Symptom burden
ABSTRACT Objectives: To investigate the current situation of palliative care needs and the symptom burden in patients with end-stage renal disease (ESRD) undergoing maintenance hemodialysis (MHD),and to explore whether there are differences between younger and older patients.Methods:This cross-sectional study was conducted in the hemodialysis centers of two tertiary hospitals from November 2021 to June 2022.Participants were selected by convenience sampling.Sociodemographics,clinical characteristics,the Palliative Care Outcome Scale (POS),the Dialysis Symptom Index(DSI),and health-related quality of life(EQ-5D-3L) were used for evaluation.Descriptive statistics,between-group comparisons,and correlation analysis were used to analyze the data.Results:A total of 236 patients were enrolled,including 118 younger and 118 older patients.The total median (P25,P75) POS score was 16.0 (12.0,23.0),and the score was higher in older patients (P <0.01).The mean total number of symptoms in MHD patients was 15.04 ± 5.06,and the overall median symptom severity score was 59.0(52.0,71.0);these scores were higher in the older group(P <0.01).The most common symptom was dry mouth (91.5%),followed by itching (83.1%),and dry skin (82.2%).Additionally,palliative care needs were significantly associated with symptom burden and health-related quality of life (HRQOL).Conclusions:The results showed that patients with ESRD undergoing MHD have a significant symptom burden and moderate palliative care needs,which are more severe in older patients.Therefore,interdisciplinary teams should be formed to actively manage patients’ symptoms and meet the physical,psychological,social,and spiritual needs related to palliative care to improve patients’ HRQOL.
What is known?
· Patients undergoing maintenance hemodialysis (MHD),especially older MHD patients,have poor health-related quality of life (HRQOL).
· Palliative care plays an important role in symptom management and HRQOL improvement for patients with limited survival and incurable diseases.
What is new?
· Preliminary investigation in more economically developed areas of China shows that patients with end-stage renal disease(ESRD) who receive MHD have a significant symptom burden and moderate palliative care needs.
· Older patients have a heavier symptom burden and greater palliative care needs than younger patients.
· Unmet needs related to physical,emotional,psychosocial,spiritual,informational,and practical matters are associated with symptom burden and HRQOL.
1.Introduction
The global prevalence of chronic kidney disease (CKD) is 9.1%(697.5 million people),and there are 132.3 million CKD patients in China [1].End-stage renal disease (ESRD) is the final stage of CKD and can only be prolonged by renal replacement therapy such as hemodialysis,peritoneal dialysis,or kidney transplantation.Maintenance hemodialysis (MHD) is the main treatment option in the mainland of China.According to the Chinese National Renal Data System in 2020,there were approximately 632,000 MHD patients[2].
ESRD remains an incurable disease,although current treatments can extend survival.Older patients are more likely to have complications and shorter survival in the process of treatment compared with younger patients [3].One study noted that the mortality rate for 1 year of dialysis was 54.5% for those over 65 years of age and up to 70.6% for those over 85 years of age [4].Notably,compared with patients with cancer,chronic obstructive pulmonary disease,and congestive heart failure,older ESRD patients have higher rates of hospitalization,admissions to intensive care,and other intensive treatments during the last month of life[5].
Owing to the dual effects of the disease itself and hemodialysis treatment,patients often experience a variety of symptoms such as fatigue,dry skin,sleep disorders,muscle cramps,itching,and other physical symptoms,as well as psychological symptoms such as anxiety,worry,and depression,which impose a huge burden on patients’ lives [6,7].Because older patients are prone to multiple chronic conditions and functional impairment,their symptom burden is heavier and their health-related quality of life(HRQOL)is worse than that of younger patients [8].
Palliative care is an approach to improve the HRQOL of patients and their families in the face of problems associated with lifethreatening illnesses,through preventing and alleviating suffering by means of early identification and accurate assessment and treatment of pain and other physical,psychosocial,and spiritual problems[9].In 2015,Kidney Disease:Improving Global Outcomes(KDIGO) [10] highlighted the urgent need to integrate palliative care services to optimize the quality of care for ESRD patients,and recommended that palliative care should be available throughout the whole course of ESRD care with or without dialysis.
Symptom assessment and management are the first steps of palliative care[11].A previous study showed that palliative care can significantly reduce the burden of symptoms and negative emotions of patients[12].Moreover,patients who choose palliative care are more likely to select the treatment method and place of death in line with their own wishes,and hospitalization rates and medical expenses are reduced [13,14].
Palliative care for ESRD patients is well developed in Canada,the United Kingdom,Australia,and New Zealand,and achieves satisfactory results[15].Although the role of palliative care for patients with non-malignant diseases has been emphasized in the mainland of China,the main population using palliative care consists of advanced cancer patients [16].The prerequisite for implementing palliative care is to identify the patient’s needs [9].The understanding of needs within palliative care is underpinned by a holistic and multidimensional approach to the suffering of patients and their families as a result of unmet physical,psychological,social,and spiritual needs[17].A previous study investigated the palliative care needs of patients with cancer and non-cancer (ESRD,heart failure,and chronic obstructive pulmonary patients)and found that both groups had symptom management needs [18].Similarly,a systematic review of the palliative care needs of patients with malignant and non-malignant diseases in Africa showed that palliative care needs embodied physical,emotional,information,relationship,practical support,financial,and spiritual aspects[17].
To achieve early identification and management of patients’symptoms and other psychological,social,and spiritual problems,and to improve patients’ HRQOL,specific palliative care needs related to ESRD patients should be identified for future service planning and implementation.Therefore,this study sought to understand the symptom burden and palliative care needs of patients with ESRD undergoing MHD,and to preliminarily analyze whether there is a relationship between palliative care needs,symptom burden,and HRQOL.Additionally,given the differences in personal characteristics and survival between younger and older patients,another objective of this study was to explore whether age-related differences in symptom burden and palliative care needs,so as to further identify priority populations and provide precise care to ensure maximum treatment benefit.
2.Methods
2.1.Study setting and participants
From November 2021 to June 2022,a cross-sectional study was conducted in hemodialysis centers of two tertiary hospitals in Nanjing,Jiangsu Province,China.The main source of samples was the hemodialysis center of BenQ Medical Center,which is the Jiangsu provincial blood purification technology training base,with 110 beds and 450 MHD patients.The other source was the hemodialysis center of Jiangsu Province Official Hospital,which has 24 beds and 62 MHD patients,mainly older patients.
A total of 236 MHD patients who met the following eligibility criteria were enrolled in this study: 1) CKD stage V (estimated glomerular filtration rate of 15 ml/(min·1.73 m2)or less calculated using the Cockcroft-Gault formula);2) duration of hemodialysis treatment ≥3 months,regular hemodialysis ≥2 times per week;3)age ≥18 years;and 4) normal cognitive function and no impairment in language communication.Patients with other serious diseases such as cancer or recent traumatic events were excluded.
2.2.Variables and measures
2.2.1.Socio-demographics and clinical characteristics
Relevant socio-demographic details were self-reported,including age,sex,education level,marital status,living status(situation regarding co-residents),employment situation,and monthly household income.Clinical data,including primary cause of disease and dialysis age,were recorded.
2.2.2.The Palliative Care Outcome Scale
Palliative care needs were assessed using the validated,selfreported Palliative Care Outcome Scale (POS),which is now widely used to investigate the palliative care needs of patients with chronic or progressive disease,regardless of the diagnostic and clinical settings[19-21].The POS consists of 12 items.The first 10 items assess the physical,emotional,psychological,spiritual,provision of information,and support domains on a scale of 0(best)to 4 (worst),with a total score range of 0-40[22].The POS has been validated in the Chinese population (Cronbach’s α=0.746) [23],and Cronbach’s α in this study was 0.809.The source scale is available for free download from the POS website(https://pos-pal.org/maix/pos-downloads.php) [24],and the right to use the Chinese version of POS was approved by the original author.
2.2.3.The Dialysis Symptom Index
The Dialysis Symptom Index (DSI) developed by Weisbord [25]was used to assess the presence and severity of symptoms in hemodialysis patients.This tool includes the 30 most common symptoms of dialysis patients,each targeting a specific physical or emotional symptom.Participants were asked to report the presence (yes or no) of each symptom in the previous week and when the symptom was present.The severity of the symptom is then assessed using a 5-point Likert scale(1=“not at all bothersome”to 5=“bothers me very much”).The symptom burden was evaluated using two parameters [26,27].First,the overall symptom burden score was generated by the mean number of symptoms reported,ranging from 0 to 30.Second,an overall symptom severity score was calculated by multiplying the number of symptoms reported(0-30) by the mean intensity of symptoms (1-5),with scores ranging from 0 to 150.A Mandarin version of the DSI was tested to ensure good reliability and validity (Cronbach’s α=0.87) [28].Cronbach’s α for the DSI in this study was 0.836.The authors obtained permission to use the research instruments.
2.2.4.Health-related quality of life
HRQOL was measured using the EQ-5D-3L scale(an instrument developed by the EuroQol Group,including 5 dimensions with 3 problem levels),which has been widely used in dialysis populations[29].This tool contains five dimensions (mobility,self-care,usual activities,pain/discomfort,and anxiety/depression),and each dimension is rated on a 3-point scale from 1 (“no problems”) to 3(“extreme problems”)[30].The total score was then converted into a value(EQ-5D Index)by using the Chinese weighting schemes;the EQ-5D Index ranges from-0.149(worst)to 1(perfect health state)[31].The authors obtained permission for the use of research tools.
2.3.Data collection
Convenience sampling was used to complete the data collection.Before the start of the investigation,participants were introduced to the purpose and significance of the study.After informed consent was obtained,two trained personnel collected the face-to-face data.For participants who had reading or comprehension difficulties,the researcher read the content of the questionnaire verbatim and helped the participants to complete the questionnaire.The questionnaire took 15-20 min to complete.A total of 238 questionnaires were distributed and 236 valid questionnaires were recovered,with an effective recovery rate of 99.2%.
2.4.Ethical consideration
Prior to the investigation,the study was approved by the Committee of Clinical Research Ethics of Jiangsu Province Official Hospital (2022-006),and written consent was obtained from the cooperative unit.Participants were aware of their rights and responsibilities,understood the confidentiality of the information,and were told they could terminate the inquiry at any time.All participants provided oral or written informed consent.
2.5.Data analysis
SPSS 26.0 was used for the statistical analysis of data.Continuous variables were described by mean and standard deviation or median and interquartile range,and categorical variables were described by frequency and percentage.Differences between the groups were assessed using Mann-Whitney tests for continuous variables,and the chi-square test for categorical variables.Correlations between variables were analyzed using Pearson’s correlation test.The level of statistical significance was set at P <0.05.
3.Results
3.1.Sample characteristics
A total of 236 MHD patients were enrolled in this study and were divided into two groups according to age: 118 younger patients (age <65 years) and 118 older patients (age ≥65 years).Table 1 presents the socio-demographic and clinical characteristics of participants of the two age groups.Briefly,the median age of the patients was 64.5 years (54.0,70.0);63.6% of patients were male and more than two-thirds of patients had an education level below senior high school.Most of the patients were married (83.1%) and living with families (92.8%).The majority of younger patients(72.9%)and older patients(99.2%)were retired or unemployed.The monthly household income of 28% of patients was less than 5,000 CNY.
3.2.Palliative care needs
Table 2 shows the total and item-specific scores of the POS and the comparison between the younger and older groups.The total median POS score was 16.0 (12.0,23.0),and older patients had higher median scores than younger patients (P <0.01).From the overall sample,the item of family anxiety had the highest median score,followed by information needs,support,practical matters,other symptoms,and wasted time.Apart from the items of information needs and wasted time,median scores for each item of the POS were higher in older patients than in younger patients,and the differences were statistically significant (P <0.05).
3.3.Symptom burden
The mean total number of symptoms in MHD patients was 15.04 ± 5.06,and was greater in older patients than in younger patients (16.02 ± 5.10 versus 14.07 ± 4.86,P <0.01).Table 3 presents the 10 most common symptoms,in descending order commencing with dry mouth(91.5%),itching(83.1%),and dry skin(82.2%).Most importantly,the symptom of feeling tired or lacking energy (86.4%) was also common in older patients.The overall median symptom severity score was 59.0 (52.0,71.0),and was higher in the older group than the younger group(61.0 versus 55.5,P <0.01).Table 4 shows the top five scores for symptom severity.The highest median severity score for each symptom was dry mouth,followed by itching and dry skin.There were significant differences in other symptoms between the two groups(P <0.05),except for the symptom of dry skin.
3.4.Correlations of palliative care needs with symptom burden and HRQOL
The overall median HRQOL score was 0.78 (0.61,0.78),and the median score was lower in older patients than younger patients(0.71 versus 0.78,P <0.01).The relationship of palliative care needs with symptom burden and HRQOL in MHD patients is shown in Table 5.The results revealed that both total and item-specific POS scores were positively correlated with the overall symptom burden score(P <0.05)and the overall symptom severity score(P <0.01),and negatively correlated with HRQOL (P <0.01).
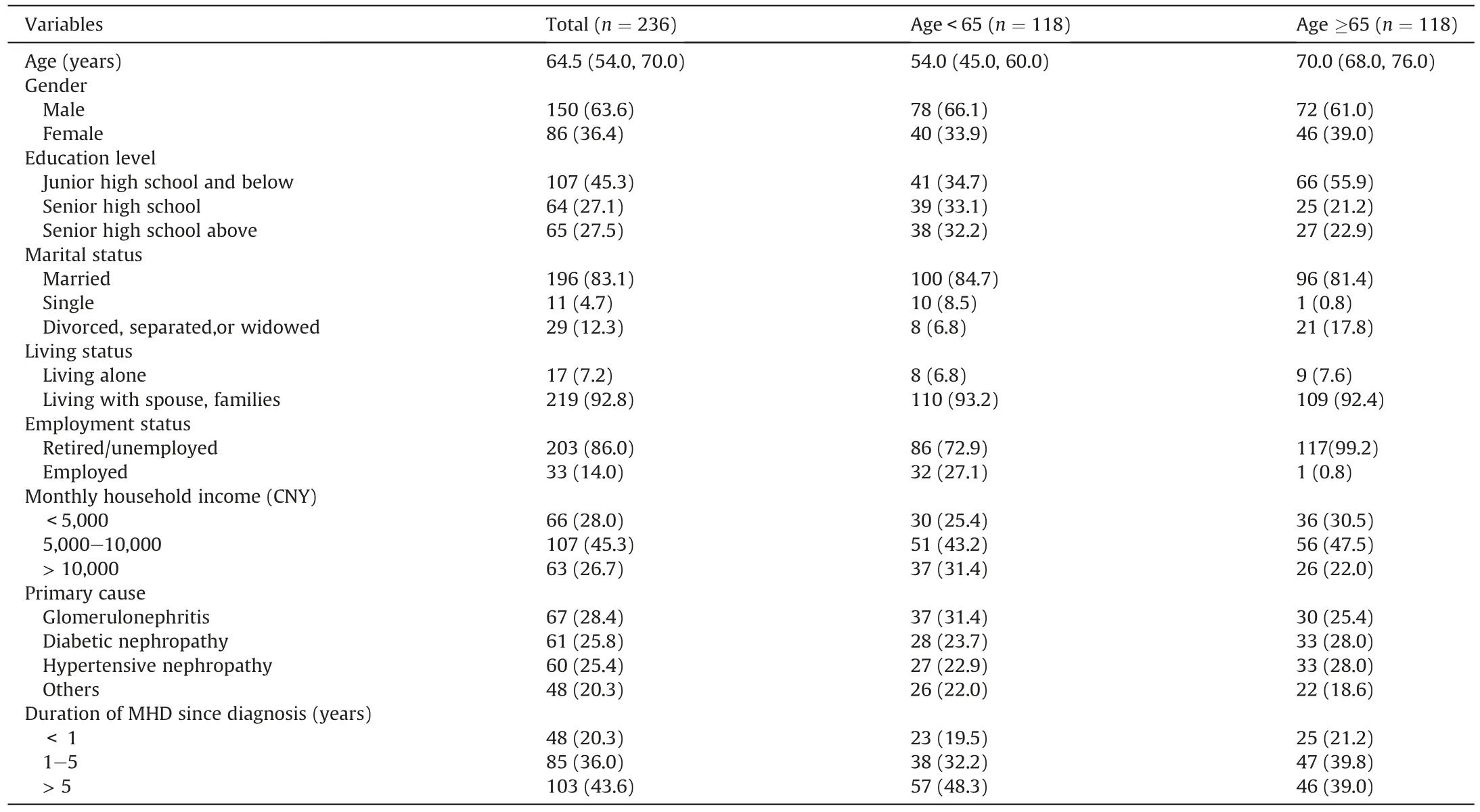
Table 1Socio-demographic and clinical characteristics of participants in the two groups.
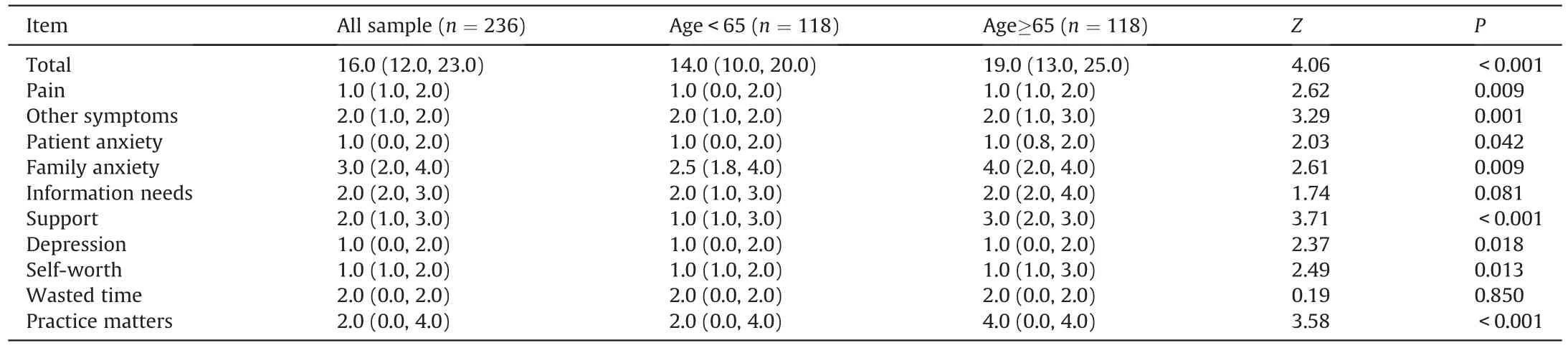
Table 2Palliative care needs and age-based comparisons.
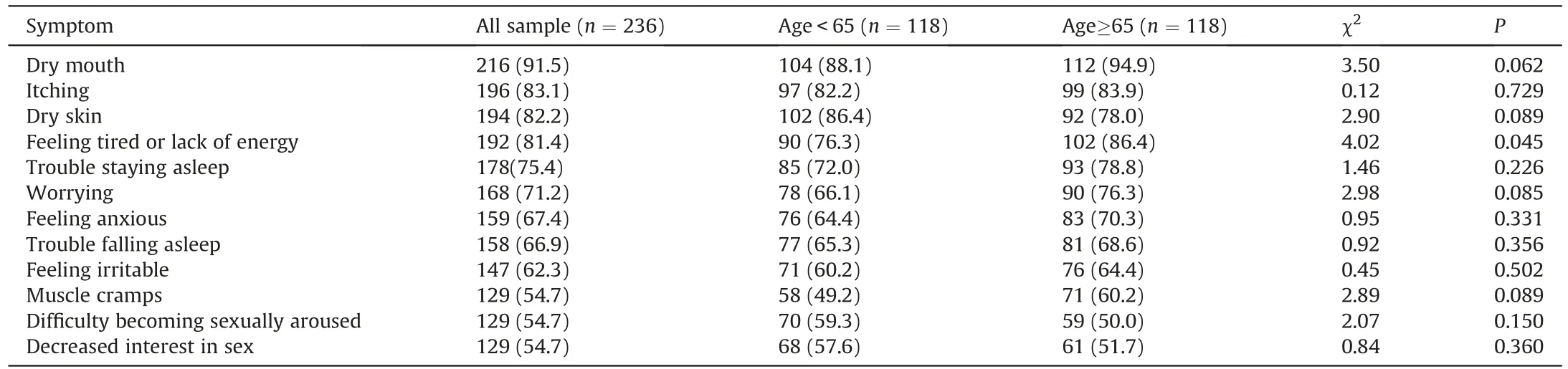
Table 3Top ten most common symptoms and age-based comparisons a.

Table 4Top five scores for symptom severity and age-based comparisonsa.
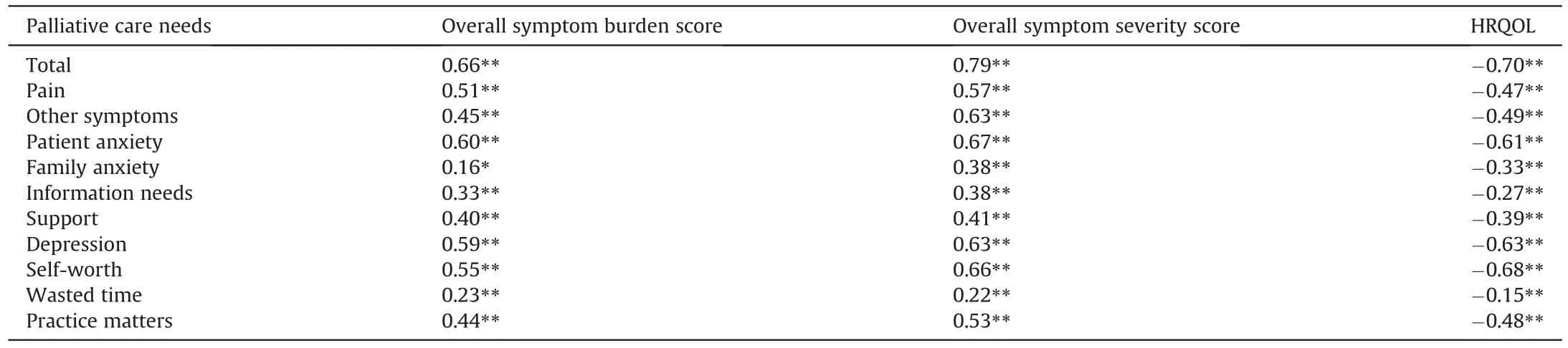
Table 5Correlation analysis of palliative care needs with symptom burden and health-related quality of life.
4.Discussion
4.1.MHD patients have moderate palliative care needs
The results of this study showed that the total median POS score of MHD patients was 16.0 (12.0,23.0),higher than that of otherserious diseases,such as advanced lung cancer (M=11;IQR=8)[20],severe chronic obstructive pulmonary disease (M=8;IQR=5)[20],and Parkinson’s disease(mean±SD=10.5±6.4)[32],suggesting that MHD patients have moderate palliative care needs.Of note,palliative care needs were higher in older patients,further validating the previous hypothesis.This may be because older adults have complex health care needs and often experience a longer burden of illness and symptoms.Furthermore,we found that both younger and older MHD patients had high levels of unmet needs,including management of other symptoms,family anxiety,information needs,time wasting,and practical matters.Although the current treatment prolongs patients’ survival time and alleviates some of the physical burden,the long-term and complex nature of the disease still poses enormous challenges to the lives of patients and their families,and increases their needs.Palliative care is holistic care provided by a multidisciplinary team that includes nephrologists,palliative care specialists,nurses,dietitians,chaplains,and social workers,focusing not only on the patient’s physical pain but also on the patient’s psychological,social,and spiritual needs [15].Studies in oncology and cardiac disease have shown improvements in the intensity of symptoms,negative emotions,and HRQOL among patients receiving palliative care compared with single standard specialized care [33,34].Additionally,compared with ESRD patients receiving palliative care services (mean± SD=10.20 ± 5.45),the POS score in this study was higher,indicating that MHD patients in our study had greater unmet needs,which further demonstrates the necessity of providing palliative care for patients [35].
Compared with the symptom control needs of advanced cancer patients,the MHD patients in this study had less need for pain control,but higher need for control of other symptoms[36].At the same time,we investigated the occurrence of various symptoms in patients and found that the average number of symptoms experienced by MHD patients was 15.04 ± 5.06,and the overall median symptom severity score was 59.0.Compared with younger patients,older adults presented with a greater number and severity of symptoms.This is consistent with the results of previous studies,indicating that MHD patients,especially older patients,have a severe symptom burden[8].We also found that the prevalence and severity of symptoms overlapped;that is,symptoms that occurred frequently tended to be more severe.Specifically,for patients in both age groups,the symptom with the highest prevalence and severity was dry mouth.Considering that poor fluid management may be closely related to dialysis-related hypotension,muscle spasm and cardiovascular complications,MHD patients are forced to control their water intake,resulting in dry mouth [37].Possibly related to mineral metabolism disorders [38],dry skin and itching symptoms were common and serious symptoms in this study.Finally,with increasing age,the organ function of the body deteriorates gradually,and the decreased physical activity resulting from declining self-care ability caused older patients in this study to experience fatigue commonly and severely [39].Notably,symptom management is a cornerstone of palliative care and can be routinely implemented in dialysis units[15].On the basis of the assessment of the patient’s symptoms,individualized symptom management is provided by the primary and specialized nephrology palliative care team,and includes not only active pharmacological treatment but also non-pharmacological treatment options such as cognitive behavioral therapy,acupuncture,and aerobic exercise,which jointly meet the physical and mental needs of the patient [15,40-42].
4.2.MHD patients’ caregivers need support
In addition to symptom management needs,unmet needs related to family anxiety in our study were the highest in both age groups,far exceeding the patient’s own anxiety level,and the results are similar to that of patients with late-stage lung cancer[20].Caregivers play an important role in the treatment of the disease,and they often face a serious caregiving burden,which greatly affects their HRQOL,psychological status,and even their own health status[43].This study found that older patients’family anxiety was more severe than that of younger patients,which was similar to the findings of Shah et al.[44].The possible reason is that because the patients’ physical functions are less healthy due to aging,their family will consume more time,and the burden of care will be heavier.Fortunately,palliative care is a unified care unit for patients and caregivers,and its role in improving the caregiver burden and HRQOL has been well validated [45,46].
4.3.Main unmet needs of MHD patients
Compared with previous studies in patients with advanced cancer and other non-cancer diseases [20,32,36],MHD patients in this study demonstrated significantly greater unmet needs related to information given,time wasting,and practical matters.The longterm nature and complexity of the disease increase the need for information on treatment modalities,prognosis,and selfmanagement.Although the difference in this study was not statistically significant,given that older adults have relatively poor health knowledge and understanding,coupled with more complex disease conditions,it is difficult to reach shared decisions and patients tend to have greater information needs [47,48].Moreover,time consumption was a common problem reported by patients in this study,considering that the patient’s regular hemodialysis treatment 2-3 times a week largely limits the patient’s daily activities.This is especially relevant for younger patients,who are forced to give up work and future plans.Finally,the patients’needs in terms of practical matters such as financial and personal issues are also huge.Economic considerations include in-hospital costs such as dialysis,drugs,examinations,and hospitalization,plus outof-hospital costs such as nutrition,nursing,transportation,and hotels.These direct and indirect costs place a heavy financial burden on patients and families [49].Additionally,personal problems are mainly reflected in those with poor self-care ability,especially older patients with declining physical and cognitive function,whose demands for medication,eating and other practical affairs will increase [50].In summary,ESRD patients on MHD have different needs compared with patients with other malignant or non-malignant diseases,so it is necessary to form an interdisciplinary palliative care team for kidney disease patients to actively evaluate and intervene in problems such as insufficient information,practical matters,and time consumption of patients during the whole treatment process,and give comprehensive supportive care based on the existing treatment environment and the patients’own conditions.
Ultimately,the findings of the present study suggest that unmet needs,such as physical,emotional,psychosocial,spiritual,informational,and practical matters related to palliative care,were significantly associated with the symptom burden and HRQOL,which was consistent with findings in Parkinson’s disease patients[32].The burden of symptoms not only aggravates the physical needs of patients,but also increases the load of psychosocial,information,practical matters,and other challenges that the disease and treatment brings to patients,resulting in more unmet needs and worsening HRQOL.Therefore,it is necessary to integrate palliative care and standard nephropathy practice at an early stage.To manage patients’symptoms,special attention should be paid to the psychological and mental status,information awareness,time consumption,economic,and personal conditions of patients and family members,to meet their holistic needs and improve their HRQOL.
4.4.Limitations of this study
This study had the following limitations.First,the study sample consisted mainly of patients with ESRD on MHD,excluding patients who chose other treatment modalities.Thus,the palliative care needs of patients with ESRD who choose peritoneal dialysis,renal transplantation,and comprehensive conservative treatment should be further investigated.Second,although the POS scale has been previously used in chronic non-malignant diseases,including nephropathy,and has good reliability and validity[35,51],this scale is not specific to nephropathy.The POS family has developed the Integrated Palliative Outcome Scale-Renal (IPOS-Renal) to identify the palliative care needs of patients with renal disease [52],but there is no Chinese version.In the future,tools to identify the palliative care needs of renal disease patients should be developed.Third,this study focused only on the relationship between palliative care needs and the symptom burden.The research team will further explore what other factors affect palliative care needs.Finally,these study participants were selected from only two hemodialysis centers;the study scope should be expanded further to comprehensively understand the palliative care needs of patients with ESRD.
5.Conclusions
This study showed that patients with ESRD undergoing MHD have a significant symptom burden and moderate palliative care needs,which are more severe in older patients.Furthermore,this study found that palliative care needs were significantly associated with symptom burden and HRQOL.In the future,interdisciplinary teams should actively manage the symptoms of patients to meet the physical,psychosocial,spiritual,information,and practical needs related to palliative care to improve the HRQOL of patients.
CRediT authorship contribution statement
Xuefei Wang:Conceptualization,Methodology,Formal analysis,Investigation,Data curation,Writing -original draft,Writing -review &editing.Qiuyin Shi:Conceptualization,Methodology,Formal analysis,Data curation,Writing -original draft,Writing -review &editing.Yongzhen Mo:Conceptualization,Methodology,Validation,Formal analysis,Data curation,Writing -review &editing,Project administration.Jing Liu:Conceptualization,Investigation,Data curation,Writing-review&editing.Yingying Yuan:Conceptualization,Investigation,Data curation.
Funding
Social Development Project of Key R&D Program of Science and Technology Department of Jiangsu Province.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of competing interest
There is no conflict of interest.
Acknowledgments
The researchers are grateful to all patients at the two hemodialysis centers who participated in the study.Also,we must express our gratitude to Ms Fan for her contribution to the statistics of this paper,and Helen Jeays,BDSc AE,from Liwen Bianji (Edanz) for editing the English text of this manuscript.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.09.015.
杂志排行

International Journal of Nursing Sciences的其它文章
- Effects of equine-assisted interventions on older adults’ health: A systematic review
- Multicenter application of a nursing workload measurement scale in adult hospitalization units
- Exploring social movement concepts and actions in a knowledge uptake and sustainability context: A concept analysis
- Lived experiences with unmet supportive care needs in pediatric cancer: Perspective of Chinese children and their parents
- Development and validation of a nomogram for predicting the risk of pressure injury in adult patients undergoing abdominal surgery
- Factors influencing the optimal selection of central venous access devices: A qualitative study of health care team members’perspectives