Central pancreatectomy for benign or low-grade malignant pancreatic tumors in the neck and body of the pancreas
2022-10-11YiWenChenJianXuXiangLiWeiChenShunLiangGaoYanShenMinZhangJianWuRiShengQueJunYuTingBoLiangXueLiBai
Yi-Wen Chen, Jian Xu, Xiang Li, Wei Chen, Shun-Liang Gao, Yan Shen, Min Zhang, Jian Wu, Ri-Sheng Que,Jun Yu, Ting-Bo Liang, Xue-Li Bai
Yi-Wen Chen, Jian Xu, Xiang Li, Wei Chen, Shun-Liang Gao, Yan Shen, Min Zhang, Jian Wu, Ri-Sheng Que, Jun Yu, Ting-Bo Liang, Xue-Li Bai, Department of Ηepatobiliary and Pancreatic Surgery, The First Affiliated Ηospital, Zhejiang University School of Medicine, Ηangzhou 310000, Zhejiang Province, China
Ting-Bo Liang, Xue-Li Bai, Department of Pancreatic Disease, Zhejiang Provincial Key Laboratory, Ηangzhou 310000, Zhejiang Province, China
Ting-Bo Liang, Xue-Li Bai, The Study of Pancreatic Disease, Zhejiang Provincial Innovation Center, Ηangzhou 310000, Zhejiang Province, China
Ting-Bo Liang, Xue-Li Bai, The Study of Ηepatobiliary & Pancreatic Diseases, Zhejiang Provincial Clinical Research Center, Ηangzhou 310003, Zhejiang Province, China
Ting-Bo Liang, Cancer Center, Zhejiang University, Ηangzhou 310058, Zhejiang Province, China
Abstract BACKGROUND For tumors in the neck and body of the pancreas, distal pancreatectomy (DP) has been the standard surgical procedure for the last few decades and central pancreatectomy (CP) is an alternative surgical option. Whether CP better preserves remnant pancreatic endocrine and exocrine functions after surgery remains a subject of debate.AIM To evaluate the safety and efficacy of CP compared with DP for benign or lowgrade malignant pancreatic tumors in the neck and body of the pancreas.METHODS This retrospective study enrolled 296 patients who underwent CP or DP for benign and low-malignant neoplasms at the same hospital between January 2016 and March 2020. Perioperative outcomes and long-term morbidity of endocrine/exocrine function were prospectively evaluated.RESULTS No significant difference was observed in overall morbidity or clinically relevant postoperative pancreatic fistula between the two groups (P = 0.055). Delayed gastric emptying occurred more frequently in the CP group than in the DP group (29.4% vs 15.3%; P < 0.005). None of the patients in the CP group had new-onset or aggravated distal metastasis, whereas 40 patients in the DP group had endocrine function deficiency after surgery (P < 0.05). There was no significant difference in the incidence of diarrhea immediately after surgery, but at postoperative 12 mo, a significantly higher number of patients had diarrhea in the DP group than in the CP group (0% vs 9.5%; P < 0.05).CONCLUSION CP is a generally safe procedure and is better than DP in preserving long-term pancreatic endocrine and exocrine functions. Therefore, CP might be a better option for treating benign or low-grade malignant neoplasms in suitable patients.
Key Words: Central pancreatectomy; Distal pancreatectomy; Endocrine function; Exocrine function; Morbidity
lNTRODUCTlON
With developments in diagnostic imaging systems, the diagnosis and incidence of benign or low-grade malignant pancreatic tumors have increased. For tumors in the neck and body of the pancreas, distal pancreatectomy (DP) has been the standard surgical procedure for the last few decades. DP is usually combined with splenectomy, and excessive pancreatic tissue is resected during the procedure. As a result, DP can lead to pancreatic endocrine or exocrine insufficiency[1,2]. Therefore, it could be beneficial to consider alternative approaches that preserve pancreatic exocrine and endocrine function in patients who require pancreatectomy.
Central pancreatectomy (CP) was first reported by Guillemin and Bessot[3] for the treatment of chronic pancreatitis and pancreatic transection injury, and the modern technique of CP can be attributed to Dagradi and Serio from the Verona group. In the CP procedure, the middle segment of the pancreas is removed and the distal pancreas and spleen are preserved. With this limited resection approach, the normal, uninvolved pancreatic parenchyma can be conserved, and thus, the risk of postoperative exocrine and endocrine dysfunction is reduced[4]. Given its advantages, some surgeons recommend CP as an alternative surgical option for tumors in the body or neck of the pancreas, as it may improve the quality of life of patients by preserving the pancreatic parenchyma and reducing the incidence of pancreatic endocrine and exocrine insufficiency. However, CP involves reconstruction of the digestive tract, and thus may result in a higher risk of postoperative morbidity than DP, especially with regard to the occurrence of postoperative pancreatic fistula (POPF)[5]. Several studies have compared the short- and long-term outcomes of the two procedures, but the efficacy and safety of CP compared to DP are unclear[6]. This study sheds light on this topic by evaluating and comparing the safety and efficacy of CP and DP for the treatment of benign or low-grade malignant pancreatic tumors in the neck and body of the pancreas based on perioperative outcomes and endocrine and exocrine function states.
MATERlALS AND METHODS
Study design and data collection
This study enrolled patients with benign or low-grade malignant neoplasms of the pancreas at the First Affiliated Hospital of Zhejiang University, School of Medicine (Hangzhou, China) between January 2016 and January 2021. The inclusion criteria were as follows: (1) Age of 18-75 years; (2) Eastern Cooperative Oncology Group performance status score of 0-1; (3) Pathological diagnosis of noninvasive intraductal papillary mucinous neoplasm, mucinous cystic neoplasm, serous cystic neoplasm (SCN), solid pseudopapillary neoplasm (SPN), or benign neuroendocrine tumor; and (4) Having received DP (with or without splenectomy) or CP. The exclusion criteria were as follows: (1) Patients with more than one primary pancreatic tumor; (2) Age younger than 18 years or older than 75 years; (3) Pathological diagnosis of invasive carcinoma or other types of lesions; or (4) Having received extra organ resection beyond the standard DP (with or without splenectomy) or CP. Finally, 296 patients were enrolled, of whom 34 underwent elective CP and 262 underwent DP. The study was approved by the institutional review board of the hospital.
Perioperative data and long-term clinical outcomes of endocrine and exocrine function were retrospectively collected and analyzed, including patient characteristics, type of surgery, preoperative radiologic imaging, and preoperative and postoperative laboratory test results. The distance between the tumor and left-side border of the superior mesenteric vein (SMV) was measured based on preoperative computed tomography images.
Postoperative complications
According to the International Study Group on Pancreatic Fistula criteria, POPF was defined as a measurable volume of drainage fluid with an amylase level more than three-times the upper limit of normal after postoperative day 3. Grade B or C of POPF was defined according to the clinical impact of POPF on the patient’s postoperative course. Delayed gastric emptying (DGE) has been classified into three grades according to its severity by the International Study Group of Pancreatic Surgery. Only grades B and C correspond to a DGE with clinical impact prolonging overall hospital stay. Postoperative morbidity was also graded according to Clavien-Dindo classification.
Evaluation of endocrine and exocrine functions
Fasting blood glucose was tested routinely in patients after surgery. Short- and long-term endocrine deficiency was defined as deterioration of endocrine function control capacity, as indicated by newonset diabetes mellitus (DM) after surgery and aggravation of DM (which meant that patients who had been previously diagnosed with and treated for DM required modified treatment after the operation). Exocrine function was evaluated based on the incidence of diarrhea after surgery.
Statistical analyses
Patient characteristics, surgical procedures, perioperative outcomes, endocrine and exocrine functions of the pancreas, and distance between the tumor and left-side border of the SMV were compared using thet-test or Wilcoxon signed-rank test for continuous variables and the chi-square test for categorical variables. Statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, United States).P< 0.05 was considered statistically significant.
RESULTS
Demographic characteristics of the patients
No significant differences were observed between the DP and CP groups regarding sex, age, preoperative body mass index, preoperative hypertension, preoperative DM, or pancreatic tumor size (Table 1). There was a difference in the distance between the tumor and left-side border of the SMV, but it was not significant. With regard to pathologic diagnosis, a higher proportion of patients in the CP group had cystic neoplasms (n= 31, 91.2%). Furthermore, the CP group also had a higher incidence of SCNs (n= 13, 38.2%) and SPNs (n= 13, 38.2%). The incidence of these lesions was similar within the DP group.
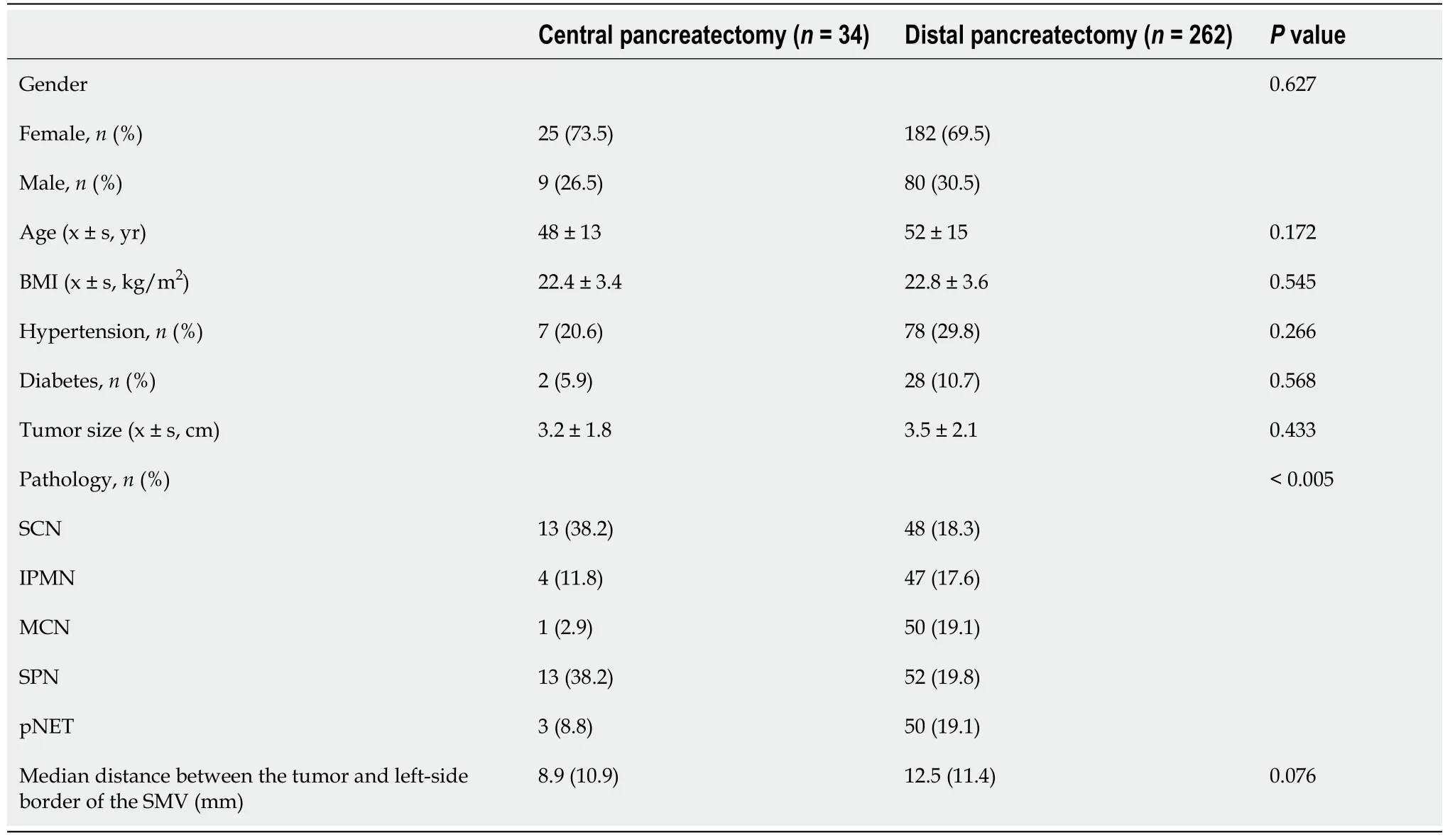
Table 1 Demographic and clinical characteristics of the patients
Perioperative outcomes
A significant difference in operation time was observed between the CP and DP groups (Table 2), which was significantly longer in the CP group. Laparoscopic surgery was more frequently performed in the DP group than in the CP group [75.8% (n= 197)vs26.5% (n= 9);P< 0.005]. No significant intergroup difference was observed in perioperative blood loss volume. It was reasonable that in the CP group, no patient received splenectomy, whereas in the DP group, 123 patients received DP associated with splenectomy, mainly due to the tissue adhesions or preoperative diagnosis of malignancy.

Table 2 Perioperative outcomes of the patients
No significant difference was observed in overall morbidity between the two groups (P= 0.370). Additionally, morbidities in the two groups were all within Clavien-Dindo grade IIIb. Regarding clinically relevant POPF, no significant difference was observed between the two groups. However, the incidence of DGE was significantly higher in the CP than in the DP group [29.4% (n= 10)vs15.3% (n= 41);P< 0.005]. Despite these findings, in the CP group, DGE was classified as grade A in most cases, and none of the patients had grade C DGE. No postoperative bleeding occurred in either group. No significant differences in chyle leakage, wound infection, or other complications were observed. The length of postoperative hospital stay was longer in the CP group, but the difference was not statistically significant (17.0 dvs11.0 d;P= 0.783). No in-hospital mortality was observed in either group, and none of the patients required readmission.
Pancreatic endocrine and exocrine functions
Regarding pancreatic endocrine function, none of the patients had new-onset or aggravated DM in the CP group, whereas 40 patients had endocrine function deficiency after surgery in the DP group (P< 0.05) (Table 3). Regarding exocrine function, only 2 (5.9%) patients had diarrhea immediately after surgery in the CP group, whereas 46 (17.5%) patients in the DP group had diarrhea immediately after surgery; however, the incidence was not significantly different. At 12 mo after surgery, however, the incidence of diarrhea was significantly higher in the DP group than in the CP group [0% (n= 0)vs9.5% (n= 25);P< 0.05]. These findings indicate that the incidence of exocrine function deficiency was significantly higher in the DP group.
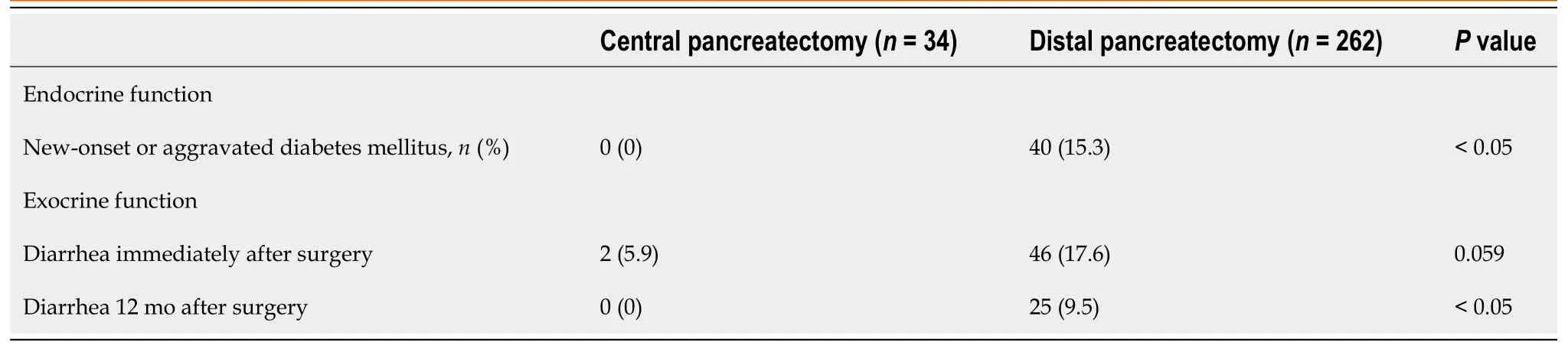
Table 3 Endocrine and exocrine function of the pancreas after surgery
DlSCUSSlON
Our study evaluated and compared the safety and efficacy of CP and DP for benign or low-grade malignant neoplasms in terms of perioperative outcomes and endocrine and exocrine functions. The results showed that CP had similar safety as DP, as the patients who underwent CP did not have more morbidities associated with surgery or more clinically relevant POPF compared to those who underwent DP. Furthermore, although CP was associated with a higher incidence of DGE, it was mild in most patients. Moreover, CP preserved the pancreatic parenchyma, and had significant advantages over DP for preserving pancreatic endocrine and exocrine functions.
Whether CP can preserve the exocrine and endocrine functions of the pancreas remains a subject of debate, even though there is some indication that CP could preserve the pancreatic volume compared with DP[5,7-12]. Shinet al[13] reported in a randomized controlled study that pancreatic parenchymal atrophy was frequently observed in patients who had clinically relevant POPF, indicating that clinically relevant POPF might reduce pancreatic parenchymal, especially in long-term outcomes. This might explain why some previous studies drew the conclusion that CP could not preserve exocrine and endocrine function, as in those studies, CP was associated with a higher incidence of clinically relevant
POPF than DP[5,7,9].
However, in this study, we found that new-onset or aggravated DM and diarrhea seldom occurred in the CP group compared to the DP group, indicating that exocrine and endocrine functions were indeed preserved with CP. In addition, a previous study compared postoperative body weight change between CP and DP and found that body weight improved within 2 years after CP, indicating that CP is an effective procedure in terms of exocrine function[8]. Thus, the findings to date, including those of the present study, generally indicate that CP is beneficial in terms of preserving pancreatic function. Since CP involves pancreaticojejunostomy and reconstruction of the digestive tract, it is reasonable that it might have a higher incidence of POPF than DP.
In this study, the incidence of diarrhea after surgery was not significantly higher in the DP group immediately after surgery but was significantly higher in the DP group after 12 mo. It is possible that the early preventive use of pancreatin after DP led to underestimation of the perioperative incidence of diarrhea. Several studies have reported that CP is associated with more morbidities (including POPF) than DP[5,7,9]. For example, a retrospective and propensity score-matched study reported that the CP procedure had more morbidities classified as Clavien-Dindo grade IIIa or worse than the DP procedure and required longer hospital stays[9]. However, in this study, the overall morbidities were similar between the two groups and there were no significant differences in the incidence of clinically relevant POPF, the most concerning morbidity. In our center, duct-to-mucosa is the most commonly used method in pancreaticojejunostomy, and this might be the reason why CP does not increase the incidence of clinically relevant POPF.
In most previous studies, open technique is performed in the CP procedure[14], although this does not mean that laparoscopy is not suitable for CP. Over the years, it has been accepted that laparoscopic surgery can be performed safely and effectively by experienced surgeons in suitable patients. Laparoscopic surgery has several apparent advantages over conventional open techniques, such as early postoperative recovery, short hospital stay, and minimally invasive incision[15-17]. In this study, laparoscopic CP was also performed in some patients, and it showed similar safety and efficacy. Therefore, it is likely that laparoscopic CP will be the mainstream choice for the treatment of benign and low-grade malignant pancreatic neck and body tumors in the future.
This study had some limitations. First, this was a retrospective analysis of patients from a single institution, so the results are subject to the biases and limitations inherent to retrospective studies. Additionally, a much lower number of patients underwent CP than DP, so this difference could also have introduced biases. Another limitation is the lack of standard criteria for evaluating exocrine function. In some studies, changes in stool elastase levels before and after surgery are used as an indicator of exocrine function[9], whereas in this study, the incidence of diarrhea was used as an indicator of exocrine function. The incidence of diarrhea caused by exocrine function deficiency may have been overestimated, since diarrhea could also be caused by other factors.
CONCLUSlON
In conclusion, we found that CP is a generally safe procedure, and has similar postoperative morbidity to DP. Further, CP is associated with better remnant pancreatic endocrine and exocrine functions after surgery. Therefore, CP might be a better option for the treatment of benign or low-grade malignant neoplasms in suitable patients as it can preserve distal pancreatic volume and improve patients’ quality of life.
ARTlCLE HlGHLlGHTS
Research background
For tumors in the neck and body of the pancreas, distal pancreatectomy (DP) has been the standard surgical procedure for the last few decades, and central pancreatectomy (CP) is an alternative surgical option.
Research motivation
Whether CP can better preserve remnant pancreatic endocrine and exocrine functions after surgery remains a subject of debate.
Research objectives
This study evaluated the safety and efficacy of CP compared with DP for benign or low-grade malignant pancreatic tumors in the neck and body of the pancreas.
Research methods
This retrospective study enrolled 296 patients who underwent CP or DP for benign and low-malignant neoplasms at the same hospital between January 2016 and March 2020. Perioperative outcomes and long-term morbidity of endocrine/exocrine function were prospectively evaluated.
Research results
No significant difference was observed in overall morbidity or clinically relevant postoperative pancreatic fistula (POPF) between the two groups (P= 0.055). Delayed gastric emptying occurred more frequently in the CP group than in the DP group (29.4%vs15.3%;P< 0.005). None of the patients in the CP group had new-onset or aggravated distal metastasis, whereas 40 patients in the DP group had endocrine function deficiency after surgery (P< 0.05). There was no significant difference in the incidence of diarrhea immediately after surgery, but at postoperative 12 mo, a significantly higher number of patients in the DP group than in the CP group had diarrhea (0%vs9.5%;P< 0.05).
Research conclusions
CP was a generally safe procedure and better than DP in preserving long-term pancreatic endocrine and exocrine functions. Therefore, CP might be a better option for treating benign or low-grade malignant neoplasms in suitable patients.
Research perspectives
The incidence of POPF might affect remnant pancreatic endocrine and exocrine functions after CP. Future prospective studies are needed with more CP cases and laparoscopic CP cases to verify this result. More reliable methods to evaluate pancreatic endocrine and exocrine functions are needed to obtain more accurate results.
FOOTNOTES
Author contributions:Bai XL and Liang TB made equal contributions in conception of the study, and review and finalization of the manuscript; Chen YW, Xu J, Li X, Chen W, Gao SL, Shen Y, Zhang M, Wu J, and Yu J reviewed and collected the data; Chen Y and Xu J analyzed the data; Chen Y wrote the manuscript; and all authors approved the manuscript.
Supported bythe National Natural Science Foundation of China, No. 82172859, 81801566, and 82071867; and the National Key Research and Development Program of China, No. 2019YFC1316000.
lnstitutional review board statement:This study was approved by the Ethics Committee of the First Affiliated Hospital of Zhejiang University, School of Medicine (No. 2022-199).
lnformed consent statement:Informed consent was exempted by the Ethics Committee of the First Affiliated Hospital of Zhejiang University, School of Medicine (No. 2022-199).
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORClD number:Yi-Wen Chen 0000-0003-4525-0954; Jian Xu 0000-0001-8132-8988; Xiang Li 0000-0002-5942-7282; Wei Chen 0000-0002-4395-6649; Shun-Liang Gao 0000-0002-4330-7139; Jian Wu 0000-0002-6325-0766; Ri-Sheng Que 0000-0003-3242-5639; Ting-Bo Liang 0000-0003-0143-3353; Xue-Li Bai 0000-0002-2934-0880.
S-Editor:Wang JJ
L-Editor:A
P-Editor:Wang JJ
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Oncologic aspects of the decision-making process for surgical approach for colorectal liver metastases progressing during chemotherapy
- Research progress on the immune microenvironment of the gallbladder in patients with cholesterol gallstones
- lrinotecan- vs oxaliplatin-based regimens for neoadjuvant chemotherapy in colorectal liver metastasis patients: A retrospective study
- Predictors of difficult endoscopic resection of submucosal tumors originating from the muscularis propria layer at the esophagogastric junction
- Liver transplantation with simultaneous splenectomy increases risk of cancer development and mortality in hepatocellular carcinoma patients
- Development of an innovative nomogram of risk factors to predict postoperative recurrence of gastrointestinal stromal tumors