Increasing rim height depth for safe femtosecond laserassisted capsulotomy in intumescent white cataracts with liquified cortex
2022-09-14BeatrizVidalVillegasJosAntonioGegndezFernndezBrbaraBurgosBlascoDavidDiazValleRicardoCuiaSardiaRosalaMndezFernndezPedroArriolaVillalobosMayteArioGutirrezJoseManuelBentezdelCastillo
Dear Editor,
Continuous curvilinear capsulorhexis is an essential part of modern cataract surgery, as it safely enables phacoemulsification procedures and permits a stable intraocular lens (IOL) bag implantation. Intumescent white cataracts with a hard nucleus and a liquefied cortex have been categorized as type I. When, in this type of cataract, the anterior capsule is opened with a cystotome the liquified cortex exits to the anterior chamber causing rapid lens decompression,nuclear displacement and sometimes capsulorhexis tearing
a feared complication that largely compromises the results of the surgery.
The study was conducted in accordance with the principles of the Declaration of Helsinki. The informed consent was obtained from the subjects.
Recently, two automatic anterior capsulotomy techniques have been introduced: the selective laser capsulotomy (SLC)and the femtosecond laser capsulotomy (FLC)
. Both offer a technical advantage over classical manual capsulorhexis:they are performed in a closed anterior chamber (AC) and may thus have lower rates of anterior capsule tearing
.
However, it is still controversial whether FLC is superior to SLC or to manual capsulorhexis in cataract surgery and specially in complicated cases
. FLC has been documented to produce a better-centered capsulotomy and may thus cause less IOL decentration and tilt than manual capsulorhexis
but may produce a less resistant capsulorhexis edge
and higher incidence of capsular tears, although these facts remain controversial
.
FLC is a very quick automatic procedure that may take between 1 and 3s and is performed normally using standard treatment parameters recommended by every laser system
. Although these parameters are set before the procedure, they can be modified to increase the success of complete capsulotomies and there is scarce literature on how they can be modified to improve the surgical results. One of the parameters that is set for FLC is capsulotomy rim height depth (CRHD). This parameter determines the height of the cylinder (with a definite diameter and rim height depth which incorporates the anterior capsule and anterior and posterior safety margins) that corresponds to the site where the laser shots are applied during FLC.
In type I white hypermature cataracts with liquefied cortex,the most difficult surgical step is performing a complete capsulorhexis, as the reported rates of incomplete manual capsulorhexis may represent up to 28% in intumescent white cataracts and only 0.8%-4.0% in normal cataracts
. However,the rate of capsular tears may be higher with FLC than with manual capsulorhexis
. Furthermore, it is not known whether FLC is superior to manual capsulorhexis in complicated cases
. We think that FLC has some advantages that may prevent the development of capsular tears in these cases,namely: 1) it is performed with a closed anterior chamber;2) is executed at a high intraocular pressure and therefore the pressure difference between the aqueous humor and the intumescent lens is smaller; and 3) the settings of the different parameters can be modified and optimize the procedure.
孙日东,郭立新,程明建,等.贝塞尔高斯光束在各向异性湍流中的传输特性[J].光子学报,2018,47(12):1201002
在各种形式的自我报告(self-report)类语料中,日记是最少受研究人员研究设计框定的。和分级任务、访谈一样,日记也主要是建立在被试对过往经历的主观回忆基础上。与其他任何形式自我报告不同的是,日记(至少是“研究人员本人日记”,self-study diaries)完全是由日记主人主导的,日记的内容、形式、写作时间等均不受任何特定语料引发任务、实验设计或社交活动的限制。
After FLC, two clear corneal incisions were made manually and a solution of 0.06% trypan blue (Blue Color Caps
Bausch and Lomb) was injected into the AC to visualize the anterior capsule. In the first four cases, in which the CRHD cylinder lost contact with the anterior capsule, we found an incomplete capsulorhexis with capsular tags in the inferior, nasal and/or temporal regions (Figure 1). After application of dispersive viscoelastic (Viscoat
, Alcon), manual completion of the capsulorhexis with forceps was carried out uneventfully in these four patients. Then phacoemulsification (Stellaris™,Bausch and Lomb) and IOL implantation were carried out in all patients.
The laser was set to perform a 5.3 mm diameter anterior capsulotomy using the following predetermined recommended parameters: pulse frequency 80 KHz, pulse duration 400-550fs, line spacing of 4.0 μm, spot spacing of 6.0 μm and pulse energy of 6.40 μJ. We used a 5.3 capsulorhexis diameter because animal studies have suggested this size as ideal for various reasons, including capsular strength
. The CRHD was set at 500 µm in the first patient and at increasing heights in the following patients.
[7][8][9]毛泽东:《毛泽东选集》(第一卷),北京:人民出版社,1991 年,第 229、236、224 页。
本研究显示,实验组老年非小细胞肺癌患者满意水平高于对照组,P<0.05;实验组术后治疗的依从性评分、住院时间优于对照组,P<0.05;护理前两组血气分析的相关指标以及焦虑情绪相似,P>0.05;护理后实验组血气分析的相关指标以及焦虑情绪优于对照组,P<0.05。实验组术后肺部感染及呼吸衰竭等老年非小细胞肺癌并发症发生率低于对照组,P<0.05。
In this letter we emphasize the importance of the CRHD settings for FLC in intumescent white cataracts. We present the results obtained in a case series that included the first five patients with hypermature white cataract with liquified cortex that were operated consecutively by the same surgeon(Gegúndez Fernández JA) using FLC. The etiology was:senile in four cases and Fuch’s uveitis syndrome in one case(Figure 1C). The patients were dilated with 3 consecutive drops of tropicamide (colirio de 1% tropicamida
, Alcon) and topic anesthesia was attained with 3 consecutive eyedrops containing a combination of 1% tetracaine and 4% oxibuprocaine (Colirio anestésico doble
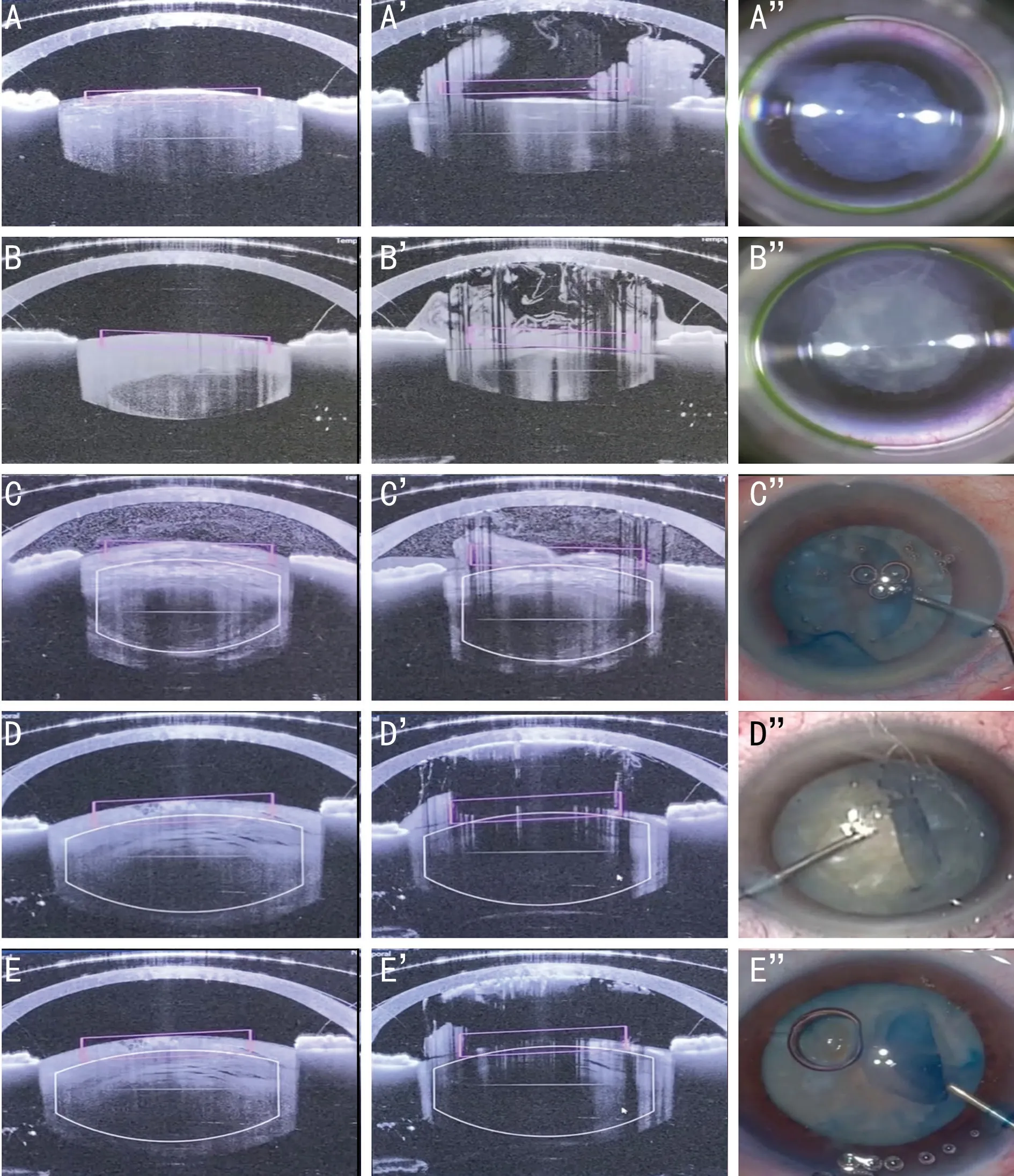
, Alcon). A curved lens applanation suction ring was docked onto the ocular surface, bathed in saline solution.The femtosecond laser was then used only for capsulotomy,but the rest of the surgery was performed manually to avoid introducing more variables. FLC was carried out using the Victus Femtosecond Laser Platform (Bausch and Lomb,Rochester, NY, USA) that has an in-built REALEYEZ sweptsource optical coherence tomography (SS-OCT) Software that allows live visualization of the procedure (Figure 1).
When initiating the FLC we observed in all patients that as soon as the anterior capsule was disrupted by the first laser shots, intralenticular bubbles formed that exited from the lens to the AC, accompanied by milky liquefied cortex (Figure 1).During the completion of the FLC, we observed a posterior displacement of the central anterior capsule and loss of volume of the capsular bag. As a consequence of these movements, in the first four patients the cylinder that represents the CRHD that can be observed in the live OCT as a rectangle (Figure 1), lost contact with the anterior capsule in some areas and therefore the subsequent laser shots did not reach the anterior capsule.Because we observed these phenomena in the first patient in which we were using a CRHD of 500 µm, in the following consecutive patients, we increased the CRHD to 600, 700, 800,and 1000 µm and only in the last case the CRHD cylinder did not lose contact with the anterior capsule and therefore laser shots reached the anterior capsule in all the circumference of the capsulotomy (Figure 1).
FLC uses individual pulses applied to laser spots that do not overlap because they are normally set at 5-6 µm separation
.This separation between spots could be responsible of leaving uncut capsular material between them
, thus producing an incomplete capsulorhexis. However, it has been documented that these capsular uncuts, named tags or bridges after FLC in most instances can be easily liberated manually
, and only very rarely produce radial capsular tears
, and this has been the case in our patients.
The completeness of the FLC could also be influenced by factors other than the separation of the laser spots, such as eye movements during the procedure or the type of the cataract:white hypermature cataracts with liquified cortex
often show incomplete capsulotomies after FLC, as in our first four patients. We show that this occurs because as soon as the first capsular opening is made, the liquid cortex exits the capsule producing a posterior displacement of the anterior capsule that exits the field of action of the laser
. However, we also document that this can be avoided increasing the CRHD up to 1000 µm. We have applied this height in our subsequent cases with excellent results.
In conclusion, we document that FLC is a safe technique in white hypermature cataracts with liquified cortex but that in this procedure it is important, in order to obtain a complete capsulotomy, to increase the CRHD setting prior to capsulorhexis.
None;
None;
None;
None;
None;
None;
None;
None;
None.
1 Perrone D, Albertazzi R. Argentinian flag sign. Video Journal Cat Refract Surg. Vol.17, Issue 1. 2001. https://eyetube.net/series/vjcrgsvolume17-issue1/argentina-flag-sign---migab?redirected=true
2 Chee SP, Chan NSW, Yang YN, Ti SG. Femtosecond laser-assisted cataract surgery for the white cataract.
2019;103(4):544-550.
3 Daya S, Chee SP, Ti SG, Packard R, Mordaunt DH. Comparison of anterior capsulotomy techniques: continuous curvilinear capsulorhexis,femtosecond laser-assisted capsulotomy and selective laser capsulotomy.
2020;104(3):437-442.
4 Kanclerz P, Alio JL. The benefits and drawbacks of femtosecond laserassisted cataract surgery.
2021;31(3):1021-1030.
5 Zhong YY, Zhu YN, Wang W, Wang K, Liu X, Yao K. Femtosecond laser-assisted cataract surgery versus conventional phacoemulsification:comparison of internal aberrations and visual quality.
2022;260(3):901-911.
6 Abell RG, Darian-Smith E, Kan JB, Allen PL, Ewe SYP, Vote BJ. Femtosecond laser-assisted cataract surgery versus standard phacoemulsification cataract surgery: outcomes and safety in more than 4000 cases at a single center.
2015;41(1):47-52.
7 Reyes Lua M, Oertle P, Camenzind L,
. Superior rim stability of the lens capsule following manual over femtosecond laser capsulotomy.
2016;57(6):2839-2849.
8 Wu BM, Williams GP, Tan A, Mehta JS. A comparison of different operating systems for femtosecond lasers in cataract surgery.
2015;2015:616478.
9 Zhu YN, Chen XY, Chen PQ, Xu W, Shentu XC, Yu YB, Yao K.Lens capsule-related complications of femtosecond laser-assisted capsulotomy versus manual capsulorhexis for white cataracts.
2019;45(3):337-342.
猜你喜欢
杂志排行

International Journal of Ophthalmology的其它文章
- What can we learn from negative results in clinical trials for proliferative vitreoretinopathy?
- Suggestions on gut-eye cross-talk: about the chalazion
- A novel mutation of RPGR in a Chinese family with X-linked retinitis pigmentosa
- Novel technique of penetrating keratoplasty in high-risk grafts with significant corneal neovascularization
- COVlD-19 infection with keratitis as the first clinical manifestation
- Corneal histomorphology and electron microscopic observation of R124L mutated corneal dystrophy in a relapsed pedigree