Clinical study on Tuina plus physical agents for lateral collateral ligament injury of ankle in gymnasts
2022-08-16HULijun胡丽君WANGJunliang王峻良LIUGang刘刚LIUKunpeng刘鲲鹏GUFei顾非
HU Lijun (胡丽君), WANG Junliang (王峻良), LIU Gang (刘刚), LIU Kunpeng (刘鲲鹏), GU Fei (顾非)
1 Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine,Shanghai 200437, China
2 Sports Hospital of Shanghai Elite Sport Training Administrative Center, Shanghai 202162, China
Abstract
Keywords: Tuina; Massage; Sprains and Strains; Ankle Injuries; Visual Analog Scale; Lateral Ligament, Ankle; Gymnastics
Lateral collateral ligament injury of ankle is a common disorder in gymnasts. Ligament injury accounts for 80.5% of sports-induced ankle injuries[1],with the lateral collateral ligament injury being the most common[2]. A study observed 14 elite female gymnasts(aged between 14 and 21 years old) and found that all the gymnasts suffered acute or subacute injuries to their feet or ankles over a period of more than three years[3]. Relevant studies have shown that after an ankle sprain, the medial and lateral collateral ligaments may heal in a relatively loose position, which is easy to cause ankle instability. Lateral ankle instability is the most common condition that may affect normal ankle function[4].
Physical agents are a routine treatment for lateral collateral ligament injury of ankle in gymnasts[5].However, this therapy only deals with acute injury via emergency treatment, and it takes a long time to repair.In addition, its effect on ankle dysfunctions after an injury is not satisfactory. In this regard, it is necessary to explore some more effective treatments for lateral collateral ligament injury of ankle[6].
Tuina (Chinese therapeutic massage) in traditional Chinese medicine (TCM) has a long history in treating diseases, with the effects of balancing Yin and Yang,unblocking meridians, promoting blood and Qi circulation, regulating tendons, and adjusting Zang-Fu organs. Lateral collateral ligament injury of ankle falls under the category of “tendon injury” in TCM. Different Tuina manipulations can be selected according to individual conditions[7-8]. In addition, Tuina belongs to non-drug therapy, in line with the treatment principles and needs of competitive athletes. In this study, we observed the efficacy of Tuina plus physical agents for lateral collateral ligament injury of ankle in gymnasts to explore the application of Tuina in the rehabilitation of competitive athletes.
1 Clinical Materials
1.1 Diagnostic criteria
The diagnostic criteria referred to the diagnostic criteria for ankle injury described in theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[9]. History of ankle trauma or sprain; pain and swelling around the ankle; ankle movement dysfunctions, and decreased range of flexion, extension, and bending; types Ⅰ-Ⅱlateral collateral ligament injury of ankle shown by musculoskeletal ultrasound.
1.2 Inclusion criteria
Met the above diagnostic criteria; met the conditions of anterior talofibular ligament and/or calcaneofibular ligament injuries; aged between 12 and 30 years old,with injury duration more than 24 h; without any treatment, or after treatment passing one-month washout period; signed the informed consent.
1.3 Exclusion criteria
Those who suffered from an ankle fracture,dislocation, ligament rupture, medial ligament injury,Achilles tendon injury, or peripheral nerve injury; those with cardiovascular disease or severe hematopoietic system disease; those with severe skin injury or skin disease involving the area to be treated.
1.4 Statistical methods
IBM SPSS for Windows version 25.0 software was applied for data analysis. Measurement data conforming to normal distribution were described by mean ± standard deviation (±s), and those not conforming to normal distribution were described by median (lower quartile, upper quartile) [M (QL, QU)].Groupt-test was used to compare the result at the same time point between the two groups, multivariate analysis of variance (ANOVA) was used to compare different treatment time points between the two groups, and repeated measure ANOVA was used to analyze the influence of group and time factors and the interaction between group and time factors.Mann-WhitneyU-test was used for data not conforming to normal distribution. Enumeration data were expressed as frequency or percentage. Chi-square test,continuous correction Chi-square test, or Fisher exact analysis was used according to specific circumstances and expected values in the table.α=0.05 was the test level.P<0.05 indicated statistical significance.
1.5 General data
This study was reviewed and approved by the Ethics Committee of Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine (Approval No. 2020-198).A total of 64 gymnasts were included, all gymnasts from the Shanghai (Chongming District) Competitive Sports Training and Management Center, and divided into an observation group and a control group according to a full analysis set based on the intention-to-treat principle,with 32 cases in each group. There was no statistical significance in comparing the gender, age, or disease duration between the two groups (P>0.05), indicating that the two groups were comparable (Table 1).

Table 1. Comparison of the general data between the two groups
2 Methods
2.1 Observation group
Patients in the observation group were treated with Tuina plus physical agents.
2.1.1 Tuina treatment
The treatment referred to the Tuina manipulations described in theTuina Therapeutics[10].
Methods:The patient took a supine position. First,An-Pressed and Rou-Kneaded the area around the affected ankle for 1 min. Dian-Digitally An-Pressed Kunlun (BL60), Qiuxu (GB40), Jiexi (ST41), Taixi (KI3),and Ashi point. Each point was treated for about 1 min(Figure 1a). Then An-Pressed and Rou-Kneaded the affected area from the outside of the lateral ankle and calf to Yanglingquan (GB34), especially Qiuxu (GB40),Xuanzhong (GB39), and Yanglingquan (GB34). Each point was treated for about 2 min, 6 min in total (Figure 1b). Next, applied one-thumb Tui-Pushing manipulation to the affected area and gradually expanded to the surrounding area. This treatment lasted for 2 min(Figure 1c). An-Pressed Qiuxu (GB40) and Yanglingquan(GB34). Each point was treated for 2 min. Finally,Ca-Rubbed the dorsum of the foot, ankle, and calf with vaseline ointment until the patient experienced hot sensations on the treated area (Figure 1d). This treatment lasted for 2 min. The Tuina treatment lasted for 20 min. After treatment, used elastic bandage to fix the affected ankle. The patients were treated once every other day for three months.
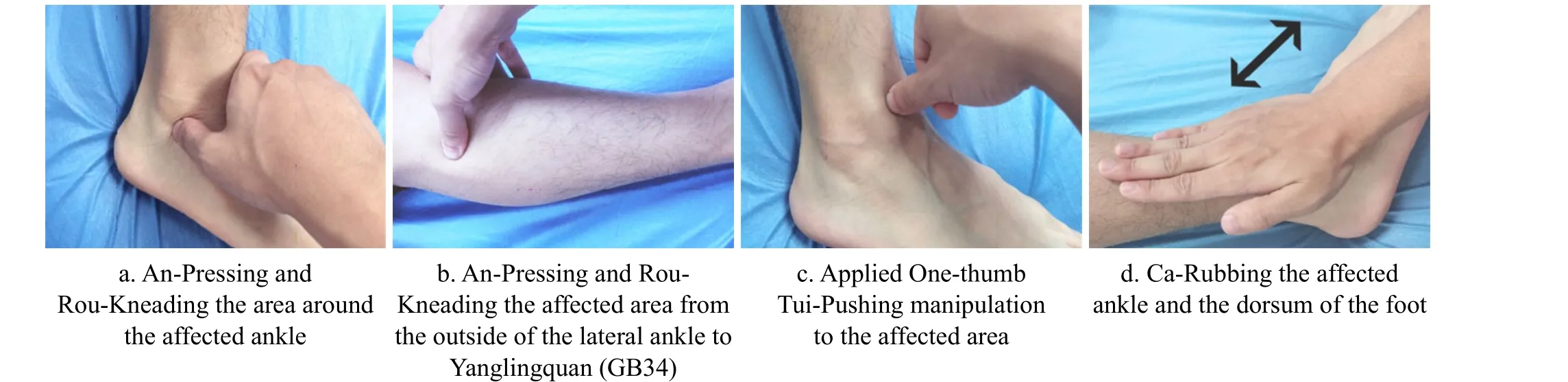
Figure 1. Tuina treatment
2.1.2 Physical agents
Physical agents included ultrasound and microwave treatment.
Ultrasound treatment: The patient took a sitting position to receive treatment with the US-100 ultrasonic therapeutic instrument. Applied the coupling gel evenly on the affected area with the ultrasonic probe, and placed the ultrasonic probe perpendicularly to the skin of the affected area. Then moved the probe linearly or circularly. The moving speed was 2 cm/s. The treatment intensity was 0.8 W/cm2, and the treatment lasted for 10 min.
Microwave treatment: The patient took a sitting position and was treated with the MT3 microwave treatment machine. Placed the radiator 1-2 cm above the affected part with a power of 30 W. Each treatment lasted for 10 min.
The patients were treated once every other day for three months.
2.2 Control group
The patients in the control group only received the identical physical agents as in the observation group,with the same treatment methods and time.
3 Observation of Clinical Efficacy
3.1 Observed items
3.1.1 Pain evaluation indicator
The pain was evaluated by visual analog scale (VAS).VAS <1 point indicated no pain; VAS ≥1 point but <3 points indicated mild pain; VAS ≥3 points but <6 points indicated moderate pain; VAS ≥6 points indicated severe pain.
Each patient was measured once before treatment,after one month of treatment, and after by the end of treatment.
3.1.2 American Orthopedic Foot and Ankle Society ankle-hindfoot scale (AOFAS-AHS)
The full score of AOFAS-AHS was 100 points,including pain (40 points), function (50 points), and alignment (10 points). The higher the AOFAS-AHS score,the healthier the ankle hindfoot.
Each patient was measured once before treatment,after one month of treatment, and by the end of treatment.
3.2 Efficacy evaluation criteria
According to the efficacy criteria for ankle injury in theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicineand AOFAS-AHS score, the efficacy criteria of this study were formulated.
Cured: The symptoms and signs disappeared, with the AOFAS-AHS score ≥90 points.
Markedly effective: The symptoms and signs almost disappeared, with the AOFAS-AHS score ≥75 points but <90 points.
Effective: The symptoms and signs were improved,with the AOFAS-AHS score ≥50 points but <75 points.
Invalid: There was no significant change in the symptoms or signs, with the AOFAS-AHS score <50 points.
3.3 Results
3.3.1 Comparison of the clinical efficacy
The clinical efficacy of the 64 patients in the two groups is as follows. After treatment, the total effective rate was 96.9% in the observation group and 90.6% in the control group. The markedly effective rate was 75.0% in the observation group and 46.9% in the control group. We compared the clinical efficacy between the two groups via Mann WhitneyU-test.There was no statistical difference in the total effective rate between the two groups (P=0.10); the markedly effective rate of the observation group was higher than that of the control group, indicating statistical significance (P<0.05). It is shown in Table 2.
3.3.2 Comparison of the VAS score
After treatment, the VAS scores showed a downward trend in both groups, and there was statistical significance within the same group between different treatment time points (P<0.05). The VAS scores of the observation group after one and three months of treatment were lower than those of the control group,indicating statistical significance (P<0.05). The results showed that the pain of patients in both groups was relieved after treatment, and the degree of improvement in the observation group was more notable than that in the control group (Table 3).

Table 2. Comparison of the clinical efficacy between the two groups (case)
Table 3. Comparison of the VAS score between the two groups ( ±s point)

Table 3. Comparison of the VAS score between the two groups ( ±s point)
Note: Compared with the same group before treatment, 1) P<0.05
Group n Before treatment After one month of treatment After three months of treatment F-value P-value Observation 32 6.94±0.91 3.97±0.601) 0.88±0.661) 2321.38 <0.001 Control 32 6.91±0.93 5.41±0.881) 2.19±0.641) 721.73 <0.001 Z-value 0.02 59.10 64.79 P-value 0.89 <0.001 <0.001
3.3.3 Comparison of the AOFAS-AHS score
After treatment, the AOFAS-AHS scores in both groups increased, and there was statistical significance within the same group between different treatment time points (P<0.05). After one month of treatment,there was no statistical significance in comparing the AOFAS-AHS score between the two groups (P>0.05).After three months of treatment, the AOFAS-AHS score in the observation group was higher than that in the control group, indicating statistical significance (P<0.05).The results showed that both treatment methods could improve the ankle symptoms and signs, and the observation group was superior to the control group(Table 4).
There was an interaction between treatment factors and time (P<0.05); that is, there was statistical significance in the change of ankle symptoms and signs between the two groups after treatment, and the observation group was superior to the control group(Table 5).
Table 4. Comparison of the AOFAS-AHS score between the two groups ( ±s point)

Table 4. Comparison of the AOFAS-AHS score between the two groups ( ±s point)
Note: Compared with the same group before treatment, 1) P<0.05
Group n Before treatment After one month of treatment After three months of treatment F-value P-value Observation 32 57.22±10.13 69.06±9.251) 79.53±8.741) 105.33 <0.001 Control 32 57.22±10.13 64.91±11.411) 73.03±12.481) 142.08 <0.001 Z-value 0.11 2.56 5.82 P-value 0.74 0.12 0.02

Table 5. Analysis of variance results for repeated measures data
4 Discussion
VAS score is a common method used to evaluate pain intensity[11]. This study showed after three months of treatment, there were statistical differences in the VAS score in the same group between the three treatment time points (P<0.05), which indicates that both methods can relieve pain. The overall change of the VAS score showed statistical significance between the two groups (P<0.05), that is, there was a significant difference within the groups before and after treatment,and the inter-group differences also showed significant,indicating that the efficacy of the observation group was superior to that of the control group. There was statistical significance in comparing the numerical changes in the VAS score between the two groups, and there was an interaction between time and group. After one month of treatment, there was statistical significance in comparing the improvement of the VAS score between the two groups (P<0.05), indicating that conventional physiotherapy plus Tuina can more quickly relieve the pain of patients than conventional physiotherapy alone. Following lateral collateral ligament injury of ankle, inflammatory infiltration may occur. Under this condition, metabolism may lead to a local acidic environment to stimulate nerve endings and subsequently cause pain[12-13]. TCM holds that obstruction and malnourishment may cause pain.Lateral collateral ligament injury of ankle may lead to stagnation of blood and Qi as well as blockage of meridians, which may subsequently cause pain. By unblocking meridians, lubricating joints and regulating tendons, Tuina manipulations can promote the recovery of ankle injury[14]. The Tuina manipulations adopted in this study, including one-thumb Tui-Pushing, Dian-Digital An-Pressing, An-Pressing, and Rou-Kneading, can unblock meridians by stimulating the points around the ankle, thus accelerating the elimination of stasis, and subsequently alleviate pain. Tuina has a significant analgesic effect on aseptic inflammation, which may be related to the increase of endogenous analgesic substances in the blood (such as serum endorphins,acetylcholine, norepinephrine, and dopamine) induced by Tuina manipulations[15-16]. The stimulation of Tuina can inhibit the pain signal from crossing the gate control system of the posterior horn of the spinal cord and thus reduce the pain perception[17]. Some scholars have proposed that pain is mainly transmitted by fine fiber nerves, while the feelings produced by An-Pressing,Rou-Kneading, and Ca-Rubbing manipulations are transmitted by coarse fiber nerves that have an inhibitory effect on fine fiber nerves. This may be another mechanism illustrating that Tuina can relieve pain[18]. Some studies believe that inhibitory reflex exists in the central nervous system. Tuina manipulations can induce the sensations of heaviness and soreness. When the pain impulse is transmitted to the system, the impulse generated by the heavy and sore sensations may reach the brain to interfere with the pain signal, reflexively weaken the pain signal and then inhibit pain, similar to pain attention diversion[19].
AOFAS-AHS scoring system, with reliability and validity, is applicable to any ankle disorder[20]. The scale evaluates the ankle functions from pain, function, and alignment. Pain, dysfunctions, and alignment changes may occur after lateral collateral ligament injury of ankle. The changes after treatment can be manifested by the AOFAS-AHS score. This study showed that after three months of treatment, there was statistical significance in comparing the AOFAS-AHS score in the two groups (P<0.05), indicating that the ankle symptoms and signs of the two groups were improved.After one month of treatment, there was no statistical significance in comparing the AOFAS-AHS score between the two groups (P>0.05). After three months of treatment, there was statistical significance in comparing the AOFAS-AHS score between the two groups (P<0.05), suggesting that the improvement of ankle symptoms and signs in the observation group was more notable than that in the control group. There was an interaction between time and group (P<0.05); that is,there was statistical significance in comparing the change of ankle symptoms and signs after treatment between the two groups, and the efficacy of the observation group was superior to that of the control group.
In the early stage of ligament injury, peripheral hematoma or edema may occur, and the clinical manifestations are pain and swelling of the ankle. The pathogenesis is mostly Qi stagnation and blood stasis.The treatment principles are to eliminate blood stasis and relieve pain. During this period, athletes can adopt rest, ice compress, pressure bandage, and raise up the affected limb when lying in bed to reduce swelling and pain. If necessary, manipulations for regulating tendons can be used. The manipulations should not be performed forcefully but along the pathways of the tendons and bones to correct tendon subluxation and bone dislocation. This is conducive to restoring the stability of the lower limb alignment and ankle[21].
In the middle stage of ligament injury, granulation tissue may form, and hematoma and edema may gradually dissipate. The treatment principles are to relax tendons and unblock collaterals. An-Pressing and Rou-Kneading manipulations can be adopted to accelerate the metabolism of necrotic substances[22].The local points on the lower limbs are mainly selected,including Kunlun (BL60), Qiuxu (GB40), Jiexi (ST41), Taixi(KI3), Xuanzhong (GB39), Yanglingquan (GB34), and Ashi point.
Kunlun (BL60), mainly used to treat heel pain, can unblock meridians, promote Qi circulation, and relieve pain. Qiuxu (GB40) is a Yuan-Primary Point. Yuan-Primary Points can clear heat, reduce swelling, unblock meridians, and benefit joints. They have clear effects in treating lateral ankle pain and swelling[23]. In addition to unblocking meridians, Jiexi (ST41) can regulate Qi and blood. It is mainly used to treat ankle disorders and pain of the lower limbs caused by Bi-Impediment syndrome.Taixi (KI3) is a Yuan-Primary Point and also a Shu-Stream Point. The kidney governs bones and generates marrow.Taixi (KI3) can tonify the kidney, and strengthen tendons and bones. It is mainly adopted to treat ankle pain.Xuanzhong (GB39) and Yanglingquan (GB34) are located above the lateral ankle. They can help with the recovery of ankle ligaments. The Ashi point can regulate Qi,relieve pain, relax tendons, and unblock collaterals[24].
Finally, apply the Ca-Rubbing manipulation to heat the lateral malleolus and its surrounding area with vaseline ointment. The heat can reach the deep to accelerate blood circulation[25]. We recommend that athletes use elastic bandages to fix their ankles for self-protection. The fixation of an elastic bandage makes the ligament heal in the tension position, which helps to maintain the stability of the ankle[26].
After treatment in the early and middle stages, most patients can recover. A few patients with severe injury may experience hematoma organization, scar formation,and adhesion, resulting in muscle spasms and ankle stiffness. In TCM, this condition is caused by Qi stagnation and blood stasis. The treatment principles are to soften hardness and dissipate masses. Specifically,first of all, apply An-Pressing and Rou-Kneading manipulations to relax and improve lower limb muscle tension. Then apply Ban-Pulling and Yao-Rocking manipulations to the affected ankle in a wider range to loosen the tissue adhesion, dissipate the masses, and thus improve the range of motion of the joint. Finally,apply Ca-Rubbing manipulation to further promote the absorption of pathological products, and fix the ankle joint in a more stable position with bandages.
Based on pattern identification in different stages,lateral collateral ligament injury of ankle can be treated by Tuina manipulations. This therapy can reduce swelling, relieve pain, regulate tendons, unblock collaterals, soften hardness, and dissipate masses[27].After Tuina treatment, fixing the ankle with a bandage helps to strengthen the ankle stability, improve alignment, and subsequently promote recovery[28].
This study found that Tuina plus physical agents can treat sports-induced injury and provide a strong guarantee for competitive sports. In view of the sensitivity of drug intervention in competitive sports,TCM external treatment has huge potential. In this study, we mainly took scales as observation indicators,and we hope to adopt imaging indicators in future research to further explore the mechanism of Tuina therapy. In addition, taking the treatment of lateral collateral ligament injury of ankle as the starting point,we hope to promote and verify the efficacy of Tuina for other sports-induced injuries and thus carry forward the TCM external treatment.
Conflict of Interest
There is no potential conflict of interest in this article.
Acknowledgments
This work was supported by Shanghai Leading Clinical Specialty of Shanghai Municipal Health Commission (上海市卫生健康委员会上海市临床重点专科, No.shslczdzk04001); Research Project of Yueyang Hospital of Integrated Traditional Chinese and Western Medicine,Shanghai University of Traditional Chinese Medicine (上海中医药大学附属岳阳中西医结合医院科研课题, No.2019YYQ11).
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received: 24 June 2021/Accepted: 29 October 2021
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Research on clinical application of manual therapy to tumor-related adverse reactions
- Observation on efficacy of thumbtack needle combined with pediatric Tuina for constipation in children caused by liver depression and Qi stagnation
- Efficacy of knee-balancing manipulation plus heat-sensitive moxibustion for knee osteoarthritis and its influence on CTX-Ⅰ, TRACP-5b,ADAMTS-4, and MMP-3
- Clinical observation of warm needling moxibustion plus lumbar traction for lumbar disc herniation
- Clinical observation of acupuncture plus acupoint sticking therapy for insomnia and its influence on subjective and objective sleep indicators
- Effects of acupuncture on nutritional status in patients in a persistent vegetative state:a prospective randomized controlled study