Acupoint application therapies for essential hypertension:a systematic review and Meta-analysis
2022-07-28LIUWeiXIONGXingjiangQIAOLuminCHENYuyiLIYixuanSUXingCHUFuyongLIUHongxu
LIU Wei,XIONG Xingjiang,QIAO Lumin,CHEN Yuyi,LI Yixuan,SU Xing,CHU Fuyong,LIU Hongxu
LIU Wei,CHU Fuyong,LIU Hongxu,Department of Cardiology,Beijing Hospital of Traditional Chinese Medicine,Capital Medical University,Beijing 100010,China
XIONG Xingjiang,Department of Cardiology,Guang′anmen Hospital,China Academy of Chinese Medical Sciences,Beijing 100053,China
QIAO Lumin,Department of Emergency,Yinchuan Chinese Medicine Hospital,Ningxia 750001,China
CHEN Yuyi,Department of Oncology,Beijing Hospital of Traditional Chinese Medicine,Capital Medical University,Beijing 100010,China
LI Yixuan,Community Healthcare Center of Shangzhuang Town,Beijing 100053,China
SU Xing,Department of Medical Administration Division,Beijing Mentougou Hospital of Traditional Chinese Medicine,Beijing 102300,China
Abstract OBJECTIVE:To evaluate the efficacy and safety of acupoint application therapies (AA) for hypertension.METHODS:We searched PubMed,EMBASE,the Cochrane Center Controlled Trials Register,Chinese National Knowledge Infrastructure,Chinese Scientific Journal Database,and Wanfang Med Online Database from their inceptions to October 7,2019.No language restriction was applied.We included randomized clinical trials testing AA against Western Medicine,AA versus placebo,AA combined with Western Medicine versus Western Medicine.Study selection,data extraction,quality assessment,and data analyses were conducted according to the Cochrane standards.RESULTS:Totally 41 trials with 3772 participants were included.The methodological quality of the included trials was evaluated as generally low.AA plus Western Medicine significantly lowered systolic blood pressure(BP) [weighted mean difference (WMD):-10.36,95%confidence intervals (CI):-12.62,-8.10;P < 0.000 01],diastolic BP (WMD:-5.71,95% CI:-7.30,-4.13;P <0.000 01),and total effect [risk ratio (RR):1.23,95% CI:1.15,1.32;P < 0.000 01].The BP-lowering effect of AA was significantly higher than that of placebo [systolic BP(SBP):−8.05,95% CI:-8.67,-7.43;P < 0.000 01;diastolic BP (DBP):-6.66,95% CI:-7.31,-6.01,P <0.000 01].The total effect also improved significantly from baseline with AA than placebo (RR:10.85,95% CI:4.71,24.98;P < 0.000 01).Traditional Chinese Medicine symptoms score were significantly reduced by AA compared with Western Medicine (WMD:-1.75,95% CI:-2.52,-0.99;P < 0.000 01),10 trials reported adverse events,indicating that the safety of SSYX Capsule is still uncertain.CONCLUSIONS: Application therapies may be considered a safe and beneficial for the treatment of hypertension and can reduce BP and improve the total effect.Further well-designed trials are needed to support our conclusions.
Keywords:hypertension;systematic review;acupoint application
1.INTRODUCTION
Hypertension is one of the leading causes of disability and premature deaths worldwide.1It is a major risk factor for vascular diseases,including coronary artery disease,renal failure,heart failure and stroke.2Unfortunately,the prevalence of hypertension is rapidly growing in developing countries,which are undergoing epidemiological transitions,economic improvement,urbanization,and longer life expectancy.3Despite the availability of effective antihypertensive treatments and guideline recommendations on the management of high blood pressure,the hypertension control rate remains unsatisfactory,and the vertigo,headache,insomnia and other symptoms of most patients have not improved.4Therefore,the complementary and alternative therapy noticed by growing number of hypertension patients might be a good choice for some people.5Complementary and alternative medicine (CAM) is a self-care option,which includes Traditional Chinese Medicine (TCM),yoga,acupuncture and massage.6,7Acupoint application (AA) is an external treatment method of traditional Chinese medicine to treat diseases,which is called percutaneous drug delivery in modern pharmacy.8,9In China,TCM practitioners utilize AA in combination with conventional Western drugs to generate more beneficial effects in reducing blood pressure (BP).10,11However,there is no critically appraised evidence such as systematic reviews or metaanalyses on potential benefits and harms of AA for hypertension to justify their clinical use and their recommendation.Therefore,the present systematic review is the first to evaluate the effectiveness of AA for EH.
2.MATERIALS AND METHODS
2.1.Inclusion criteria
Randomized controlled trials (RCTs) that met the following criteria were enrolled into the present review:(a) the participants were diagnosed with EH;(b) the study must be an RCT;(c)the study compared AA alone or combined with conventional Western Medicine with conventional Western Medicine or placebo;(d) the primary outcomes were defined BP,including systolic blood pressure (SBP),diastolic blood pressure (DBP),and total effect,the three grades were based on the evaluation criteria obtained from the total effect of AA on BP,according to the Guidelines of Clinical Research of New Drugs of Traditional Chinese Medicine.(e) the secondary outcome was the symptoms score.The response to the treatment of the symptoms score for hypertension,which was assessed based on the criteria in the Guiding Principles of Clinical Research on New Drugs of Traditional Chinese Medicine (2002).
2.2.Search strategy and data extraction
In the update of this systematic review,databases we searched,including PubMed,EMBASE,the Cochrane Center Controlled Trials Register,Chinese National Knowledge Infrastructure,Chinese Scientific Journal Database,and Wanfang Med Online Database,from inception to October 7,2019.Seven search components were applied:“hypertension”,“essential hypertension”,“high blood pressure”,“Acupoint Application”‚“Acupuncture Point Application”,“Randomized Controlled Trial”,and “controlled clinical trial”.
The reference lists of the selected articles were also manually screened for possible related new studies.There were no language restrictions.The bibliographic data,including the name of the author/s,age,title,participation,gender of the subjects,publication year,intervention characteristics (frequency,intensity,duration,type and level of supervision),outcomes and adverse effects,and composition of the Chinese medicine for AA,were registered.Duplicate studies were excluded.The study inclusion was performed by two authors (Xiong Xingjiang and Chu Fuyong) using the predefined inclusion and exclusion criteria.Disagreements were resolved by discussion with a third investigator (Liu Hongxu).
2.3.Methodological quality assessment
Two independent reviewers (Chu Fuyong and Liu Wei)assessed each publication using the the Cochrane Handbook for Systematic Review of Interventions.
2.4.Data analysis
The statistical software programme RevMan 5.3 was used to estimate the computation of all the effects [with 95% confidence intervals (CI)].Continuous outcomes were presented as weighted mean difference (WMD),and the pooled risk ratio (RRwith 95%CI) was computed.TheI 2statistic was used to assess the variability between studies.
3.RESULTS
3.1.Study selection and characteristics
The present search strategy initially identified 214 articles.A total of 187 publications remained after reviewing the titles,and removing the duplicated publications.The remaining articles were assessed for eligibility,and 56 of these fulfilled the inclusion criteria.Finally,41 studies 12-52 were included in the Metaanalysis (15 were excluded for the reasons listed in PRISMA 2009 Flow Diagram).There were a total of 3772 subjects in these studies,which ranged from 45 to 201.The baseline age of these subjects ranged within 32-87 years old,and the duration of the total treatment time ranged within 2-96 weeks.These studies were all conducted in China.
3.2.Methodological quality
The quality of these 41 studies was low,based on criterion of the Cochrane handbook.The detailed information is presented in Figures 1 and 2.Several trials(n=11) were judged as having a low risk of bias in the random sequence generation using the random number table.Approximately all of these studies were assessed as having an unclear risk of bias due to insufficient descriptions in allocation concealment,the blinding of the outcome assessment,the blinding of participants and(or) personnel,and selective outcome reporting.Merely two studies22,31reported the information of the follow-up,while four studies18,22,32,52reported the dropouts without a detailed description.

Figure 1 PRISMA 2009 Flow diagram
3.3.Effects of the interventions
3.3.1 Total effect
A total of 29 trials with 2559 hypertensive patients,which compared AA combined with Western Medicine to Western Medicine,were identified.The Meta-analysis revealed that AA combined with Western Medicine has a significant beneficial effect in the total effect to Western Medicine (RR:1.23,95%CI:1.15,1.32;P <0.000 01;Figure 3).We provided the subgroup analysis based on different Western Medicine.14 trials13-16,25,28-30,34,36-30,36discovered AA combined CCB showed better effect compared to CCB alone (RR:1.16,95%CI:1.10,1.22;P <0.000 01,I2=12%).There were statistically differences on the AA combined with ARB groups to ARB using alone in two trials12,37(RR:1.44,95%CI:1.09,1.92;P=0.01,I2=12%).Two studies50,52compared AA with placebo,and a significant improvement in the total effect was observed by AA (RR:10.85,95%CI:4.71,24.98;P<0.000 01,I2=0%).Merely three trials47-49presented AA alonevs.Western Medicine,but no significant effect was found for total effect between these two groups (RR:1.07,95%CI:0.86,1.32;P=0.55).
3.3.2 Blood pressure
Compared with conventional medicine,23 individual trials reported a reduction in BP after the treatment favored AA plus conventional medicine.Furthermore,there was a statistically significant mean decrease in SBP in the combination group,when compared with Western Medicine group (WMD:−10.36,95%CI:−12.62,−8.10;P<0.000 01;Figure 4).In relation to the diastolic blood pressure (DBP),22 studies14-19,21,25-28,30-33,36-37,39,41,44-46demonstrated a better effect that favor AA combined with conventional medicine (WMD:−5.71,95%CI:−7.30,−4.13;P<0.000 01;Figure 5).We did a subgroup analysis based on a variety of western drug types.11 trials14-16,25,27-28,30,33,36,39,46discovered the better effect on both SBP and DBP (SBP:−7.39,−9.67 to−5.12;DBP:−5.88,−9.94 to −8.83) when compared combination with CCB alone.AA-ARB37showed better effect compared to ARB for SBP and DBP (SBP:−8.66,−9.37 to −7.95;DBP:−6.88,−7.59 to −6.17).

Figure 2 Risk of bias graph
The main outcome measures were the SBP or DBP in two RCTs that used AA,when compared to placebo.50,51The mean differences in SBP and DBP were−8.05 mm Hg (SBP:−8.05,95%CI:−8.67,−7.43;P<0.000 01,I2=0%) and −6.66 mm Hg (DBP:−6.66,95%CI:−7.31,−6.01;P <0.000 01,I2=0%).
3.3.3 TCM symptoms score
Six studies16,18,20,26,28,39examined the impact of AA combined with Western Medicine on the TCM symptoms score.Significant decreases in the TCM symptoms score were observed with the combination of AA and Western Medicine (WMD:−1.75,95%CI:−2.52,−0.99;P <0.000 01).
3.4.Adverse effects (AEs)
A total of 10 trials described information about the AEs.No AE was described in seven trials,20,25,29,30,34,42,51while one trial17reported AEs without the details of AA.One trial37reported the AEs,which included one case with elevated alanine aminotransferase (3.8%) and one case with tachycardia (3.8%),while in the control group,two cases had elevated alanine aminotransferase (4.2%),one case had hypotension (2.1%),one case had nausea(2.1%),and one case had cough (2.1%).One trial47reported the AEs,which included two cases with increased blood viscosity (2%),two cases with hypokalemia (2%),and one case with hyperlipidemia(1%) in the AA group,and five cases with increased blood viscosity (5%),four cases with hypokalemia (4%),three cases with hyperlipidemia (3%),and three cases with gout (3%) in the controlled group.No serious AEs were described.
3.5 Publication bias
The funnel plot analysis of the outcomes of SBP are presented in Figure 6 to evaluate the publication bias.Publication bias was present,according to the asymmetric plot.

Figure 3 Forest plot of comparison:acupoint application therapies combined with Western Medicine versus Western Medicine for total effect
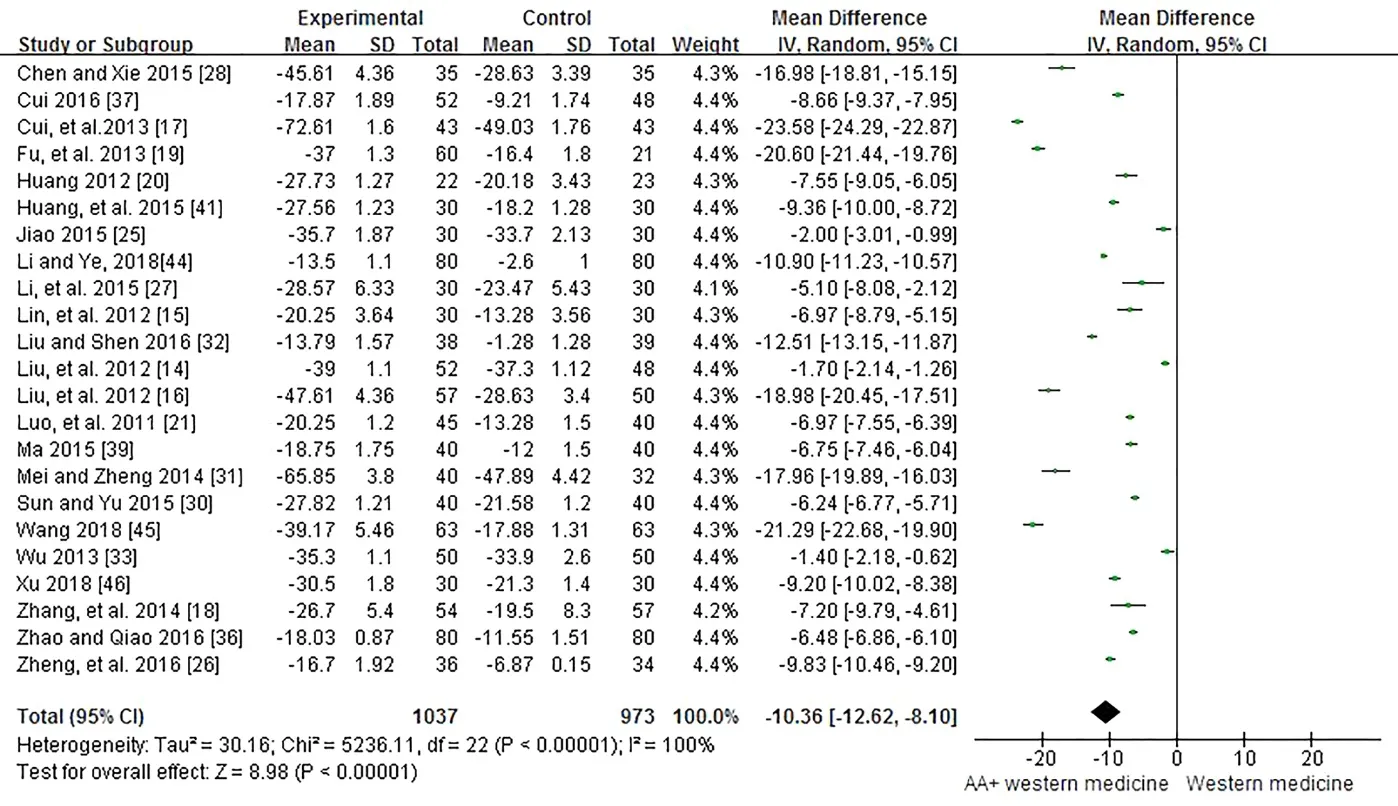
Figure 4 Forest plot of comparison:acupoint application therapies combined with Western Medicine versus Western Medicine for systolic blood pressure

Figure 5 Forest plot of comparison:acupoint application therapies combined with Western Medicine versus Western Medicine for diastolic blood pressure

Figure 6 Funnel plot of the trials that compared AA combined with Western Medicine with Western Medicine for SBP
4.DISCUSSION
The present systematic review is the first to investigate the effects of AA on hypertension,and offer recommendations for future research.The present Metaanalysis provided the clinical efficacy of a single treatment and the combination with Western Medicine,and it was found that this had more superior efficacy and fewer side effects,when compared to Western Medicine alone.The 31 acupuncture points in all the included studies were summarized,and the most commonly used acupoints were,as follows:Yongquan (19.0%),Shenque(8.6%),Sanyinjiao (8.0%),Shenshu (7.4%),and Quchi(6.0%).In the present review,23 studies reported the AA intervention on BP outcomes.The combination of AA and Western Medicine significantly lowered the SBP of 10.36 mm Hg and DBP of 5.71 mm Hg,when compared to Western Medicine.When compared to placebo,AA as adjuvant therapy significantly decreased the SBP by 8.05 mm Hg and the DBP by 6.66 mm Hg.In the total effect,the Meta-analysis revealed a significant effect on the treatment of AA combined with Western Medicine.In addition,the effect in the treatment of AA alone was obviously better than placebo.In summary,AA can be used as a complementary and alternative therapy for hypertension.Although antihypertensive drugs have made great progress,and BP could be well-controlled,dizziness,headache,nausea and other symptoms still troubles hypertension patients.In the present study,AA significantly relieved the symptoms and lowered the effect on the TCM symptoms score,when compared to Western Medicine.This shows that AA can be used as a great adjutant therapy for hypertension patients with uncomfortable symptoms.
The present review had the following limitations.The majority of the included trials were assessed to have one or more high risks of bias.Although all studies declared randomization,merely 11 studies used the random number table in the sequence generation,while the other 30 trials merely mentioned “randomly allocating” with no details.It is indeed difficult to implement the doubleblind method,but this is still the best design for randomized controlled studies.No trials described allocation concealment,the blinding of participants and personnel,and the blinding of outcome assessment,which lead to the inability to judge whether the study was properly conducted.Merely two trials reported information on the follow-up,and four trials mentioned the dropouts with specific reasons.In addition,the incomplete outcome data was not revealed in all trials.There was some heterogeneity in the data collection in the systematic evaluations of AA.First,moderate to high heterogeneity was observed,which represented a difficulty in establishing the true impact of AA,although most of these factors were explored through the subgroup and meta-regression analyses.Different interventions,including the criteria of participants,manipulation methods,and frequency/duration of the treatments,the composition of Chinese herbs for AA,and the selection of the acupoint,resulted to heterogeneity.Second,Figures 6 was asymmetrical.Therefore,publication bias might exist to affect the results of the present analysis.AA has been widely used for EH in China.Positive results have been reported in most of the included studies,while some negative results could not be reported.Therefore,a certain degree of potential selective bias might exist in this conclusion.The publications were limited to the Chinese language in this review,which may also have led to the omission of important works.In conclusion,this Meta-analysis showed that AA could improve the symptoms of hypertensive patients,and reduce BP,suggesting that AA is effective for the treatment of hypertension.However,the stability of our results would be affected due to the poor methodological quality and high heterogeneity in the trials.Future RCTs with a larger sample size and high methodological quality are required to evaluate the effectiveness of AA in treating EH,on the account of the poor quality of methodology.
杂志排行

Journal of Traditional Chinese Medicine的其它文章
- Biosynthesis of titanium dioxide nanoparticles using Hypericum perforatum and Origanum vulgare extracts and their main components,hypericin and carvacrol as promising antibacterial agents
- Protective effect of resveratrol on rat cardiomyocyte H9C2 cells injured by hypoxia/reoxygenation by regulating mitochondrial autophagy via PTEN-induced putative kinase protein 1/Parkinson disease protein 2 signaling pathway
- Efficacy of aqueous extract of flower of Edgeworthia gardneri (Wall.)Meisn on glucose and lipid metabolism in KK/Upj-Ay/J mice
- Effect of manipulation on cartilage in rats with knee osteoarthritis based on the Rho-associated protein kinase/LIM kinase 1/Cofilin signaling pathways
- Baicalin inhibits inflammation of lipopolysaccharide-induced acute lung injury via toll like receptor-4/myeloid differentiation primary response 88/nuclear factor-kappa B signaling pathway
- Modified Gexiazhuyu decoction (膈下逐瘀汤加减方) alleviates chronic salpingitis via p38 signaling pathway