Yellow nail syndrome accompanied by minimal-change nephrotic syndrome: A case report
2022-06-22YaNanZhangMeiHuaWangWenChengYuWeiChengJinPengCongXuePengHuangFangFangWang
INTRODUCTION
Yellow nail syndrome (YNS) is a rare disorder characterized by yellow nails, lymphedema, and respiratory manifestations; two of which are sufficient for the diagnosis of YNS. The complete triad is present only in 27% to 60% of patients[1], and symptoms may occur years apart, which delays diagnosis. Adults aged > 50 years are highly susceptible to this disease, and a few pediatric cases have been reported[2,3]. Currently, the pathogenesis of YNS has not been fully elucidated. Some cases have previously been reported in families[4], with most members acquiring the disease. Lymphatic involvement and microvasculopathy are the most important pathological changes. In this report, we describe a case of YNS with bilateral pleural, pericardial and peritoneal effusions as well as a secondary nephrotic syndrome.
CASE PRESENTATION
Chief complaints
Dyspnea, cough, expectoration and abdominal distension for 1 mo.
History of present illness
A 62-year-old man presented with a 1-mo history of dyspnea, cough, expectoration and abdominal distension. Due to mild proteinuria, hypoalbuminemia and elevated blood creatinine levels, he was diagnosed with glomerulonephritis at the local hospital, and was treated with diuretics and drugs to lower urine protein levels. Despite treatment, dyspnea worsened. Therefore he was referred to our hospital for further treatment.
History of past illness
The patient reported no history of hepatitis, tuberculosis or heart disease before.
He mourned for him in black raiment for forty days; and then, a few days later, his second son, Prince Qamas, extracted from him leave to go too; and he, also, was put to death
Personal and family history
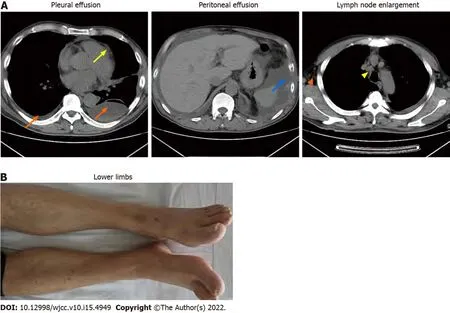
Lung involvement in YNS, which occurs in 56%-71% of the patients, diversely affects some parts of the respiratory tract with a variety of clinical manifestations[5]. Chronic cough, pleural effusion and bronchiectasis are common pulmonary manifestations of YNS[12]. In a meta-analysis, 68.3% of the YNS patients had bilateral pleural effusions and 95% of effusions were described as exudates (median protein level: 4.2 g/dL) with lymphocytic predominance in 96%[13]. In our case, bilateral pleural effusions were the main clinical manifestation (Figure 1C) and presented as chylothoraxexudates. These findings are consistent with those of a previous report[14]. Thoracic duct and lymphatic vessel rupture or obstruction in the thoracic cavity is associated with lymph accumulation in the pleural cavity to produce chylothorax. Besides, the patient developed pericardial and peritoneal effusions (Figure 1C). As far as we know, this is the first report about multiple effusions caused by YNS.
Physical examination
Physical examination revealed multiple effusions in the chest, pericardium and abdominal cavity,accompanied by nonpitting edema of the chest and abdominal walls, as well as pitting edema of both lower limbs (heavier in the right lower limb). The patient’s toenails were thickened and yellow, with increased curvature and slow growth (0.2 mm/wk), as were his nails (Figure 1A).

Laboratory examinations
YNS.
Effusions in these areas, subcutaneous edema, pleural thickening, and enlarged axillary as well as mediastinal lymph nodes were confirmed by computed tomography (CT) (Figure 1C). Positron emission tomography (PET)/CT scans revealed multiple symmetrical distributions of enlarged lymph nodes in the neck, chest, abdomen, pelvis, and left ethmoid sinusitis (Figure 1C). Doppler echocardiography revealed pericardial effusion and a mild decrease of the left ventricular diastolic function.Radionuclide lymphoscintigraphy revealed interrupted lymphatic vessels of the right lower limb, with the imaging agent being accumulated in subcutaneous tissues, inguinal lymph nodes on the right side were not clear, and lymphatic vessels of the left lower limb exhibited collateral circulations (Figure 1D).
That was all that the rascal11 wanted, and he put on directly his most humble12 air, and begged the woman in his softest voice to loosen his bonds, which her hurting him sorely
Imaging examinations
When Charles went to Switzerland for a ski vacation, Diana missed him terribly. He called her after a day or two, and told Diana he had something important to ask her.
FINAL DIAGNOSIS
Clinical assessment revealed mild proteinuria (0.32 g/24 h), severe hypoalbuminemia (23.39 g/L),elevated serum creatinine levels (139 umol/L) and D-dimer (3270 pg/mL) levels. Even though white blood cell counts were elevated (11.33 × 10
/L), the neutrophil/lymphocyte ratio was normal. Blood coagulation, electrolytes, serum lipids, antinuclear antibodies, extractable nuclear antigens spectrum,antineutrophil cytoplasmic antibodies, immunoglobulin (κ and λ light chains), hepatitis virus detection,double-stranded DNA, tumor markers, T-cell interferon- release assays and B-type natriuretic peptide were all normal. We performed bilateral thoracentesis and abdominal puncture to detect tuberculosis and tumors. Both pleural and peritoneal effusions were composed of exudates, mainly lymphocytes(60% and 77%, respectively). Chyle test of the pleural fluid was positive. There were no tumor cells in the pleura, pleural as well as peritoneal effusions (Figure 1B), and the tuberculosis nucleic acid test was negative. Lymph node biopsy (right axillary) (Figure 1B) revealed proliferative lesions of the lymphoid tissue, lymphatic sinuses and lymphoid follicles. The toenails were negative for fungi or parasites.
“If human beings are not drowned,” asked the little mermaid, “can they live forever? do they never die as we do here in the sea?” “Yes,” replied the old lady, “they must also die, and their term of life is even shorter than ours
TREATMENT
The patient was treated with vitamin E (0.6 g/d) and clarithromycin (0.5 g/d).
OUTCOME AND FOLLOW-UP
Cheng W and Wang MH analyzed and interpreted the patient data regarding the disease; Cong JP and Wang MH performed the histological examination of the pleura and pleural effusion; Huang XP performed the histological examination of kidney; Zhang YN and Wang FF was major contributors in writing the manuscript;Yu WC reviewed and corrected the manuscript; all authors issued final approval for the version to be submitted.

DISCUSSION
The first case of YNS was reported by Heller in 1927. The prevalence of YNS has not been fully established; however, based on the number of reported cases, it is estimated that it is less than 1/1000000[5]. Moreover, its pathogenesis has not been conclusively evaluated. At present, it is considered to be as a result of abnormal lymphatic functions, including lymphatic dysplasia, chylothorax and obstructed lymphatic drainage caused by lymphatic vessel damage, among others. YNS patients also present with various comorbidities, including nephrotic syndrome, endocrine diseases,infections and malignant tumors[6-9]. There may also be complications caused by abnormal lymphatic functions in different parts.
Yellow nail is a characteristic manifestation of YNS. The patients have dark nail discoloration, which varies from pale yellow to more or less dark green, thickening of the nail layer, excess bending,onycholysis and slow growth[5]. These physical signs can appear alone, without lymphedema or respiratory manifestations. Our patient’s toenails were thickened and yellow, with increased curvature and slow growth (0.2 mm/wk), as were his nails (Figure 1A). Microscopic examination of nail slices revealed that normal loose fibrous blood vessels had been replaced with dense collagen fibers[10].Accumulation of the lipofuscin pigment explains the yellow discoloration. These pathological changes are attributed to poor lymph drainage under the nail[11].
The patient reported no personal or family history.
So, you know, it s just this kind of feeling I can t convey8 it clearly! The train life is impressive9 on everybody; we had a lot of activities, for example giving a speech on a stage or singing together or playing basketball
Lymphedema has been reported in 29%-80% of previous cases, and may be the first signal to seek medical care[12]. Lymphedema mainly affects both lower limbs[14]. Lymphoscintigraphy is an effective imaging modality that is widely used for differential diagnosis of lymphedema and for determining the extent of the disease[15]. Lymphoscintigraphy of this case revealed that lymphatic vessels of the right lower limb were interrupted and collateral circulation appeared in the lymphatic vessels below the left knee which resulted in edema of both lower limbs (Figure 1D).
Sinusitis is common among YNS patients. A previous study reported that 44 of 85 YNS patients had chronic rhinosinusitis, which presented with nasal/postnasal drainage (94%), obstruction/congestion(81%), facial pain/pressure (33%) and anosmia (8%)[16]. Sinusitis of this patient was confirmed by imaging studies, with no obvious symptoms (Figure 1C). There are many causes of sinusitis, including microbial infections, allergies, and abnormal anatomical structures. The lymphatic tissue plays an important role in immune responses.
The main therapeutic options for YNS include clinical management of yellow nails, pleural effusion and lymphedema. Vitamin E is also a potential therapeutic option, although its efficacy and putative mechanisms have not been established. Somatostatin analogs, primarily octreotide, have also been used to treat pleural effusions and lymphedema, with varying outcomes[5]. In YNS patients, anti-inflammatory activities of macrolides might improve systemic inflammation, which reduces lymphedema and promotes nail growth[22]. Algain[23] reported the first and only case of a YNS patient who failed to respond to fluconazole and vitamin E, but showed near-complete recovery after administration with terbinafine and topical minoxidil. In this case, the patient was administered with vitamin E, clarithromycin and oral metoprolol. Subsequently, his dyspnea, pleural effusions, pericardial effusions, ascites and systemic edema (Figure 2A and B) were relieved, hypoalbuminemia was also corrected, while proteinuria gradually reduced.
Then he realized that he had come to a witch s house, but because it was dark, and he could go no further, he entered. In any event, he was not afraid.
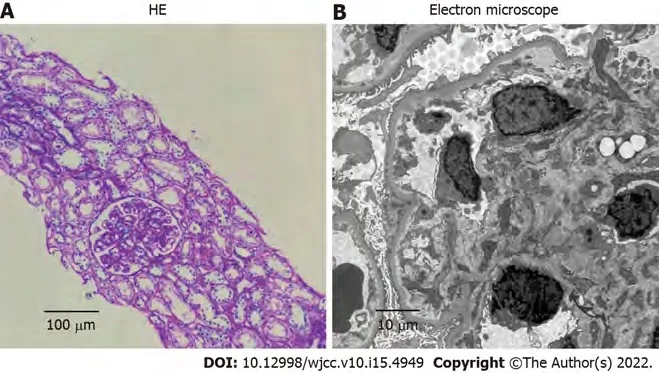
In addition, YNS patients can also present with multiple comorbidities, including nephrotic syndrome, endocrine diseases, infections, and malignant neoplasms. There are three reports on the presence of nephrotic syndrome in YNS[17-19]; two of which were minimal nephritic syndrome change.At the time of reporting, clinical examination of this case was almost complete, and diseases associated with related symptoms such as infections, tumor and immunity excluded. Due to heavy proteinuria, a diagnosis of nephrotic syndrome was made, and subsequent renal biopsy confirmed minimal-change nephrotic syndrome (Figure 3), similar to a previous report[19]. The pathogenic association between YNS and minimal change nephrotic syndrome is unclear. Yáñez
[18] suggested a causal relationship between the two disorders. Gupta
[20] found a striking deficiency of naive CD4
and CD8
T cells and total B cells, and increased transitional B cells in YNS patients. Furthermore, the dysfunction of T cells and B cells has been confirmed to play a central role in minimal change nephrotic syndrome[21].We postulate that YNS patients may have extensive lymphatic dysfunctions, and renal lymphatic drainage is blocked, resulting in antibody stasis and deposition in the glomerular capillary network,leading to pathophysiological changes of nephrotic syndromes.
The brothers were at once set at liberty, while Sir Red, for his wickedness, was hanged on the highest tree that could be found, and so he got the reward he deserved
CONCLUSION
The classic triad is not present in many cases of YNS, especially in comorbid cases, leading to delayed or missed diagnosis. Once YNS is considered, it is recommended to improve relevant examinations of the lymphatic system for further determinations. There is a need to establish a more systematic, comprehensive as well as standardized diagnosis and treatment options for this disease.
FOOTNOTES
After 1 mo of treatment, dyspnea, pleural effusions, pericardial effusions, ascites and systemic edema were relieved (Figure 2A). However, proteinuria was significantly elevated (4.87 g/24 h). Renal biopsy confirmed minimal-change nephrotic syndrome (Figure 3A and B). The combination of clinical and laboratory findings revealed that the patient had nephrotic syndrome. Therefore, he was treated with oral metoprolol (8 mg/d). Two months later, his proteinuria had been relieved. The clinical course and therapy of the patients are shown in Figure 4.
All study participants, or their legal guardian, provided informed written consent prior to study enrollment.
The authors declare that they have no conflict of interest.
The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
China
9. The stove vanished: she had only the remains of the burnt-out match in her hand: Vision number one. This vision directly addresses the girl s coldness.
Ya-Nan Zhang 0000-0002-5382-6944; Mei-Hua Wang 0000-0002-7876-0726; Wen-Cheng Yu 0000-0001-8274-2742; Wei Cheng 0000-0002-2965-5698; Jin-Peng Cong 0000-0003-2638-8667; Xue-Peng Huang 0000-0002-1578-6219;Fang-Fang Wang 0000-0003-1954-5660.
Liu JH
Kerr C
Liu JH
1 Aslam MZ, De Loughry G, O'Brien B. Anaesthesia and orphan diseases: Yellow nail syndrome.
2020;37: 728-730 [PMID: 32692084 DOI: 10.1097/EJA.0000000000001169]
2 Hsu TY, Lin CC, Lee MD, Chang BP, Tsai JD. Titanium Dioxide in Toothpaste Causing Yellow Nail Syndrome.
2017; 139 [PMID: 27940507 DOI: 10.1542/peds.2016-0546]
3 Cecchini M, Doumit J, Kanigsberg N. Atypical presentation of congenital yellow nail syndrome in a 2-year-old female.
2013; 17: 66-68 [PMID: 23364154 DOI: 10.2310/7750.2012.12015]
4 Razi E. Familial yellow nail syndrome.
2006; 12: 15 [PMID: 16638408]
5 Vignes S, Baran R. Yellow nail syndrome: a review.
2017; 12: 42 [PMID: 28241848 DOI:10.1186/s13023-017-0594-4]
6 Emerson PA. Yellow nails, lymphoedema, and pleural effusions.
1966; 21: 247-253 [PMID: 5914998 DOI:10.1136/thx.21.3.247]
7 Beer DJ, Pereira W Jr, Snider GL. Pleural effusion associated with primary lymphedema: a perspective on the yellow nail syndrome.
1978; 117: 595-599 [PMID: 629489 DOI: 10.1164/arrd.1978.117.3.595]
8 Lewis M, Kallenbach J, Zaltzman M, Conlan A, Zwi S, Abramowitz J. Pleurectomy in the management of massive pleural effusion associated with primary lymphoedema: demonstration of abnormal pleural lymphatics.
1983; 38: 637-639[PMID: 6612658 DOI: 10.1136/thx.38.8.637]
9 Uchida T, Uchida Y, Takahashi M, Masaki K, Sato H, Iemura H, Shinomiya S, Nakamura H, Nagata M. Yellow Nail Syndrome in Which Intranodal Lymphangiography Contributed to the Diagnosis.
2021; 60: 3599-3603 [PMID:34092726 DOI: 10.2169/internalmedicine.6499-20]
10 DeCoste SD, Imber MJ, Baden HP. Yellow nail syndrome.
1990; 22: 608-611 [PMID: 2319021 DOI:10.1016/0190-9622(90)70081-r]
11 Norton L. Further observations on the yellow nail syndrome with therapeutic effects of oral alpha-tocopherol.
1985;36: 457-462 [PMID: 4075838]
12 Piraccini BM, Urciuoli B, Starace M, Tosti A, Balestri R. Yellow nail syndrome: clinical experience in a series of 21 patients.
2014; 12: 131-137 [PMID: 24134631 DOI: 10.1111/ddg.12216]
13 Valdés L, Huggins JT, Gude F, Ferreiro L, Alvarez-Dobaño JM, Golpe A, Toubes ME, González-Barcala FJ, José ES,Sahn SA. Characteristics of patients with yellow nail syndrome and pleural effusion.
2014; 19: 985-992[PMID: 25123563 DOI: 10.1111/resp.12357]
14 Maldonado F, Ryu JH. Yellow nail syndrome.
2009; 15: 371-375 [PMID: 19373089 DOI:10.1097/MCP.0b013e32832ad45a]
15 Kwon HR, Hwang JH, Mun GH, Hyun SH, Moon SH, Lee KH, Choi JY. Predictive role of lymphoscintigraphy undergoing lymphovenous anastomosis in patients with lower extremity lymphedema: a preliminary study.
2021; 21: 188 [PMID: 34879819 DOI: 10.1186/s12880-021-00713-1]
16 Gutierrez CN, Low CM, Stokken JK, Choby G, O'Brien EK. Characterization of Sinus Disease in Patients with Yellow Nail Syndrome.
2020; 34: 156-161 [PMID: 31603343 DOI: 10.1177/1945892419881253]
17 Cockram CS, Richards P. Yellow nails and nephrotic syndrome.
1979; 101: 707-709 [PMID: 534618 DOI:10.1111/j.1365-2133.1979.tb05651.x]
18 Yáñez S, Val-Bernal JF, Fernández-Llaca H. Yellow nails and minimal change nephrotic syndrome.
1999; 82:180-182 [PMID: 10364711 DOI: 10.1159/000045395]
19 Sakiyama T, Shimizu T, Funakoshi T, Saito M. Case of yellow nail syndrome accompanied by nephrotic syndrome.
2016; 43: 585-586 [PMID: 26704457 DOI: 10.1111/1346-8138.13239]
20 Gupta S, Samra D, Yel L, Agrawal S. T and B cell deficiency associated with yellow nail syndrome.
2012; 75: 329-335 [PMID: 21995335 DOI: 10.1111/j.1365-3083.2011.02653.x]
21 Kim SH, Park SJ, Han KH, Kronbichler A, Saleem MA, Oh J, Lim BJ, Shin JI. Pathogenesis of minimal change nephrotic syndrome: an immunological concept.
2016; 59: 205-211 [PMID: 27279884 DOI:10.3345/kjp.2016.59.5.205]
22 Matsubayashi S, Suzuki M, Suzuki T, Shiozawa A, Kobayashi K, Ishii S, Iikura M, Izumi S, Kudo K, Sugiyama H.Effectiveness of clarithromycin in patients with yellow nail syndrome.
2018; 18: 138 [PMID: 30111321 DOI: 10.1186/s12890-018-0707-4]
23 Algain M. Yellow Nail Syndrome Successfully Treated with Oral Terbinafine and Topical Minoxidil.
2021; 14: 249-252 [PMID: 33746514 DOI: 10.2147/CCID.S301197]
杂志排行

World Journal of Clinical Cases的其它文章
- Diet and intestinal bacterial overgrowth: Is there evidence?
- Spontaneous liver rupture following SARS-CoV-2 infection in late pregnancy: A case report
- Metastasis of liver cancer to the thyroid after surgery: A case report
- Solitary primary pulmonary synovial sarcoma: A case report
- Knot impingement after arthroscopic rotator cuff repair mimicking infection: A case report
- Clear aligner treatment for a four-year-old patient with anterior crossbite and facial asymmetry: A case report