Intraoperative endoscopic retrograde cholangiopancreatography for traumatic pancreatic ductal injuries:Two case reports
2022-05-18AndrewCanakisVarunKesarCalebHudspathRaymondKimThomasScaleaPeterDarwin
INTRODUCTION
Pancreatic duct (PD) injuries are uncommon (occurring in 3% to 12% of traumas),primarily due its protective retroperitoneal location.They can be difficult to diagnose due to non-specific symptoms and delayed findings on imaging[1].A delay in diagnosis can result in severe complications,such as a pancreatic fistula,hemorrhage,or abscess by which obtaining a fast and accurate diagnosis is paramount[2,3].
Standard therapy for high grade pancreatic injury with traumatic PD disruption is operative.As the duct itself is not amenable to repair,surgical options are resection and/or simple drainage accepting the inevitable pancreatic fistula.Major pancreatic resection is morbid and can produce nutritional cripples and render patients diabetic.Preoperative imaging is often inaccurate or not feasible.The limited sensitivity (52%) of computed topography (CT) is further complicated by timing,as CT scans performed in less than 24 h of presentation can often miss PD injuries as inflammatory associated changes are yet to manifest[1,4,5].There is also poor sensitivity associated with magnetic resonance cholangiopancreatography (MRCP) imaging,and many times unstable patients may not be suitable for such imaging[4,6].
The diagnosis of PD transection is often suspected at the time of laparotomy.Knowing whether the PD is actually transected can be difficult.Visual inspection can over diagnose these injuries leading to unnecessary surgery.One would prefer to limit major pancreatic procedures to those patients with hemorrhagic shock or those without other options.
While endoscopic retrograde cholangiopancreatography (ERCP) is the most accurate method for assessing PD integrity and extent of injury,its wide spread use is hindered due to limited resources,local expertise and difficulty performing the procedure itself in an emergent,operative setting[1,7].ERCP can also be therapeutic as PD stenting can be performed at the time of diagnosis.Stenting a duct that is transected can be challenging but if successful,the duct may heal around the stent and limit the need for major pancreatic resection.In this case series,we present two cases treated at a major urban trauma center where PD injuries were diagnosed with intraoperative ERCP and treated with sphincterotomy and stenting.
CASE PRESENTATION
Chief complaints
Multiple gunshot wounds (GSWs).
History of present illness
A 27-year-old male presented with four GSWs to the chest and abdomen.
Of course not, said the old man. But, if it did, you need not worry. She would never divorce you. Oh, no! And, of course, she will never give you the least, the very least, grounds for-uneasiness.
Upon arrival he was found to have penetrating GSWs to the left shoulder,left axilla,right flank,and subxiphoid areas.
History of past illness
Both patients had no specific history of past illness.
Personal and family history
No pertinent personal or family history of both patients.
Physical examination
A 16-year-old female initially presented to an outside hospital with severe upper quadrant abdominal pain following blunt abdominal trauma.She remained at the hospital for two days with an inability to tolerate per oral intake,nausea,and vomiting.
Upon arrival she was afebrile (37 ℃),normotensive (119/71 mmHg) but tachycardic (130 beats per min) with abdominal tenderness to palpation.
Attracted by the sweet perfume he flew lower, and perceived some large and beautiful gardens filled with the rarest flowers, and with fountains throwing up their clear waters into the air in a hundred different shapes
In the churchyard where the walls were surrounded with sandClara lay buried. Jurgen did not seem to know this; it did not enterhis mind, which could only retain fragments of the past. EverySunday he went to church with the old people, and sat theresilently, staring vacantly before him. One day, when the Psalms werebeing sung, he sighed deeply, and his eyes became bright; they werefixed upon a place near the altar where he had knelt with his friendwho was dead. He murmured her name, and became deadly pale, andtears rolled down his cheeks. They led him out of church; he toldthose standing round him that he was well, and had never been ill; he,who had been so grievously afflicted, the outcast, thrown upon theworld, could not remember his sufferings. The Lord our Creator is wise and full of loving kindness- who can doubt it?
The Prince and all the courtiers were delighted to see their beloved King again, but they had to submit themselves to more frequent absences than ever on his part
Laboratory examinations
Labs on admission were notable for a white blood cell (WBC) count 10.9 K/mcL,hemoglobin 12.5 g/dL,platelets 430 K/mcL,international normalized ratio 1,aspartate transaminase (AST) 315,alanine transaminase (ALT) 282,alkaline phosphatase (ALP) 72,total bilirubin 0.2,amylase 127 units/L,lipase 59 units/L and lactate 6.8 nmol/L.He was resuscitated and imaging was obtained.
Labs were notable for a WBC 16.6 K/mcL,Hg 11 g/dL,AST 23,ALT 12,ALP 74,total bilirubin 2.3 mg/dL,lipase 1160 units/L and amylase 441 units/L.
Imaging examinations
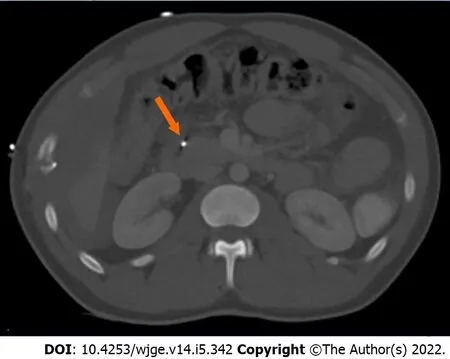
Computed tomography angiography of the chest abdomen and pelvis revealed significant injuries,including but not limited to a left ventricle apex cardiac injury,laceration of liver lobe segments two and six,a pancreatic artery pseudoaneurysm (measuring 1.4 cm),and shrapnel wounds to the gallbladder,duodenum,pancreatic head,and hepatic flexure (Figure 1).There was no mention of pancreatic leak.
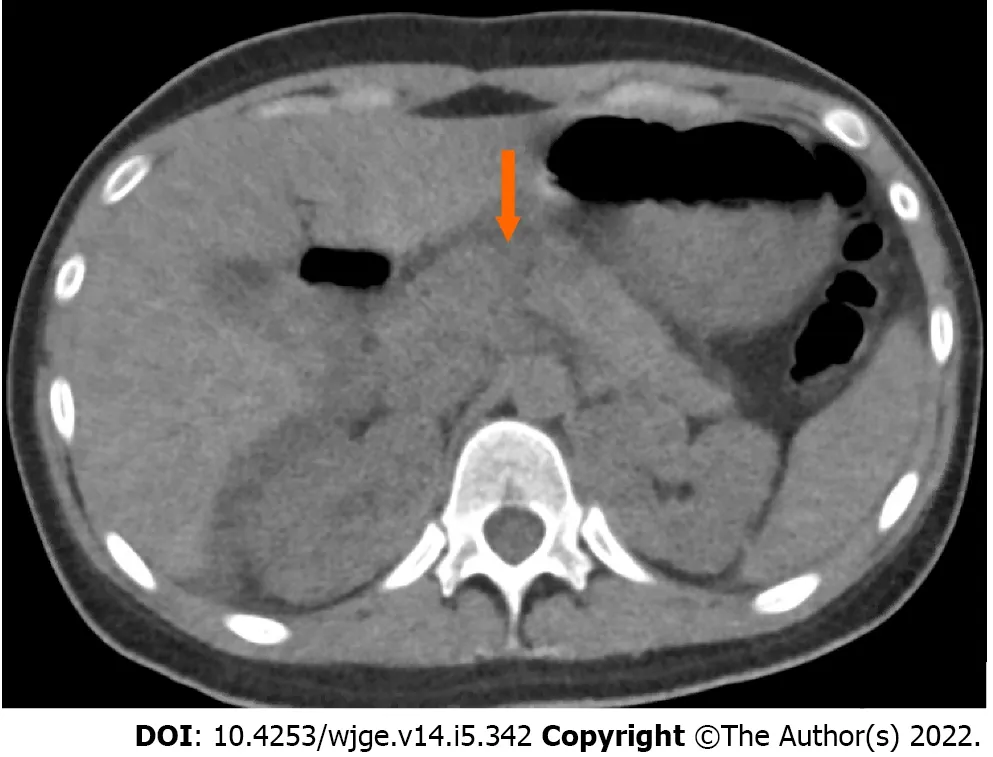
A CT of the abdomen demonstrated a grade III pancreatic injury (thickness pancreatic transection involving the proximal tail and neck),large hemoperitoneum,and a 1 cm posterior splenic laceration for which she was transferred to our center for surgical care (Figure 2).
Further diagnostics
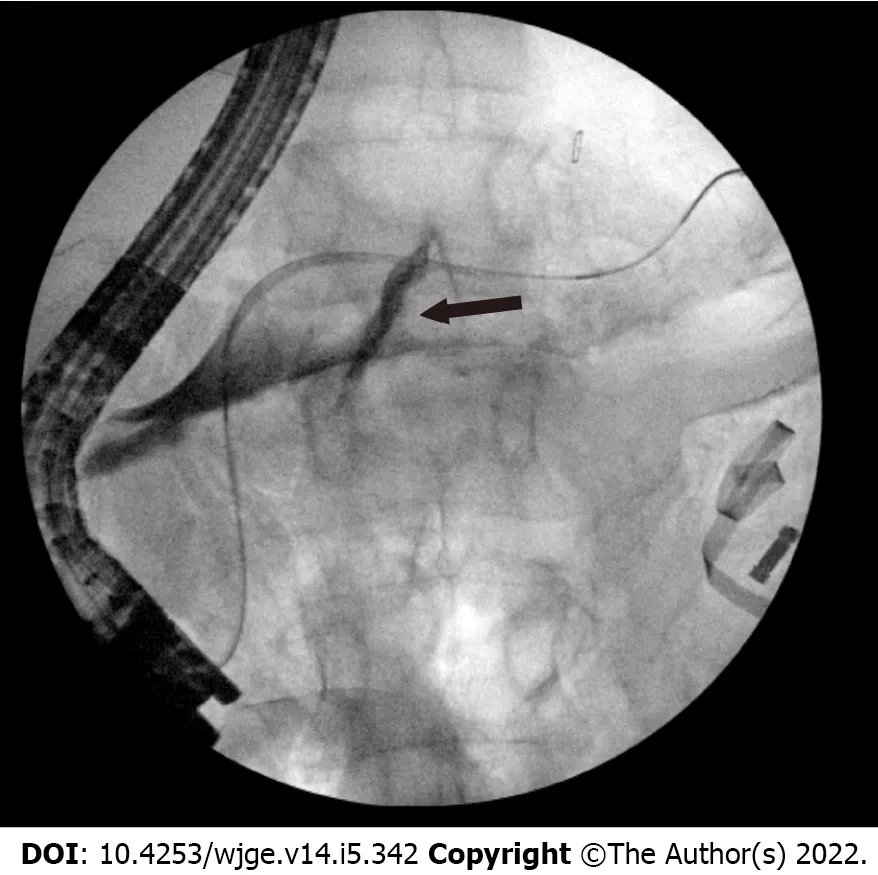
He immediately went to the operating room (OR) for exploratory laparotomy where he underwent a non-anatomic bilateral liver resection,cholecystectomy,colon resection with end colostomy,gastric wedge resection,small bowel resection (20 cm) with anastomosis.He had a highgrade injury to his pancreatic head that would have required a Whipple to treat but it was not clear that he had a major PD injury.An intraoperative ERCP demonstrated a ventral PD leak in the head of the pancreas (Figure 3).

She was sent directly to the OR,where an exploratory laparotomy revealed 500 mL of pancreatic ascites which was evacuated from the lesser sac and right upper quadrant.There was concern for PD disruption at proximal aspect of the pancreatic tail.An intraoperative ERCP demonstrated a PD leak in the body (Figure 4).
When he came to the forest the little old grey man met him likewise, and greeting him, said, Give me a piece of your cake and a drink out of your bottle; I am so hungry and thirsty. Dummling answered, I have only cinder-cake and sour beer; if that pleases you, we will sit down and eat. 17 So they sat down, and when Dummling pulled out his cinder-cake, it was a fine sweet cake, and the sour beer had become good wine. So they ate and drank, and after that the little man said, Since you have a good heart, and are willing to divide what you have, I will give you good luck. There stands an old tree,18 cut it down, and you will find something at the roots. Then the little man took leave of him.
One of them Beauty recognized as the stately lady she had seen in her dreams; the other was also so grand and queenly that Beauty hardly knew which to greet first
FINAL DIAGNOSIS
Both patients were diagnosed with PD leaks.
TREATMENT
I hesitated. The thought of these brought up another loss. The last time I made potato pancakes was two and a half years ago. I had taken off my engagement ring to make the dough2, and never found it again. Since then, I resisted using that recipe even though I really liked those pancakes. It s sort of silly, but whenever I considered making them, I felt resentful of their participation3 in my loss, as if they were partly to blame.My mom should know better than to suggest these, I thought. (I don t even remember her ever making them.) She knew how upset I was about losing my ring. I had always called her whenever I lost something, even when I was away at college, even from across the country, even when I traveled abroad. She had a knack4 for helping5 me find my way to lost things, except for this time.


Similarly,in case 2,a 4 mm ventral sphincterotomy was performed followed by placement of a 5 Fr by 13 cm plastic stent into the dorsal pancreatic duct (Figures 6 and 7).There was no evidence of bile leakage.Her pancreas widely drained.The time from hospital admission to ERCP was 5.65 h.The procedure was technically successful with no adverse events.Her abdomen was left open.The next day,a MRCP confirmed placement of the pancreatic duct stent,which traversed the area of pancreatic transection with the tip of the stent residing in the tail of the pancreas.Two days after her initial surgery,she returned to the OR for abdominal re-exploration,pancreatic debridement,omentopexy,and primary closure.

OUTCOME AND FOLLOW-UP
Patient 1 was eventually discharged with a 25 d hospital length of stay.In the outpatient setting he underwent repeat ERCP with stent removal 84 d after discharge,with leak resolution and no further symptoms.The second patient’s hospital length of stay was 22 d,and she was discharged without any major ERCP or pancreatic related complications.She underwent a repeat ERCP with stent removal 59 d following its initial placement with resolution of ductal injury.
Grampy stretched his long leg out straight and reached his huge hand deep into the pocket. I could hear the familiar jangling of the loose change he always carried. Opening his fist, he exposed a mound10 of silver coins. There must have been a million dollars there. He instructed me to pick out a dime11. I obeyed. After he deposited the rest of the change back into his pocket, he stood up.
DISCUSSION
This series demonstrates the efficacy,safety,and feasibility of intraoperative ERCP as a diagnostic and therapeutic tool.In this case series the average time from admission to ERCP occurred within 5.95 h.Both patients also underwent successful stent removal without any post-ERCP complications and resolution in the PD injury.
Clinical manifestations and management of PD leaks are largely dependent on the leak’s size and location,where the integrity of the main duct influences prognosis[8].In the setting of ductal injury,high pressure gradients cause pancreatic juices to flow outwards;as such,transpapillary stenting reduces the pressure gradient with preferential flow through the stent into the duodenum in order for the injury to properly heal.At our center,we always perform a sphincterotomy with stent placement instead of employing nasobiliary catheter,with well documented success in cases of hepatic trauma as well[9].
The role of intraoperative ERCP in the trauma setting is not yet well defined.In a study of 71 patients with pancreatic injury,50 of whom underwent immediate laparotomy,there was a 14% complication and 20% mortality rate[4].In that study,intraoperative ERCP was not used.Instead,intraoperative visual inspection was undertaken to investigate for ductal injury.Four patients deemed not to have a leak developed pancreatic leaks with abscess formation.ERCP should be considered in the setting of traumatic pancreatic injury with a questionable PD injury.Its high diagnostic accuracy cannot be matched by any combination of a CT abdomen,serum amylase or peritoneal lavage[10].In a large PD trauma series,an abdominal CT missed the diagnoses of major PD injury in 40.7% (11/27) of patients[11].Furthermore,in a prospective study of 14 patients with PD injury,those undergoing ERCP greater than 72 h following trauma had higher rates of pancreatic complications and longer hospital stays[12].In our series,both patients underwent ERCP immediately with no ERCP related complications or delayed lengths of hospital stays.One could postulate that early intraoperative ERCP effectively contained the leak and contributed to these positive outcomes.
ERCP with early stenting has also proven to be an effective and safe option in pediatric cases[13,14].Yet,there has been some concern regarding the development of strictures,though it’s unclear if such a complication occurs from the trauma itself or stent-induced changes[7].In a small study analyzing long term outcomes for pancreatic stenting from blunt trauma the authors found that only 50% (3/6) of stents were successfully removed at 12,19,and 39 mo[15].Such complications were not seen in our patients,likely because the stents were removed significantly earlier with minimal stent exchanges.
Studies exploring pancreatic trauma have not detailed intraoperative timing,which may be an important aspect for reducing complications as well.In a study of 43 patients with major PD trauma,15 underwent stenting as the first treatment modality with a median time from trauma to ERCP of 6 d[12].Within this group,there were 17 related complications including pseudocyst formation (8),PD stricture (4),distal pancreatic atrophy from injury site (3),and pancreatic fistulas (2).They also reported two deaths,one of which was related to severe pancreatitis where the stent was removed 8 d after insertion.The other death was attributed to a patient with severe alcoholic liver cirrhosis-unrelated to the stent.In another study of 48 patients with pancreatic trauma (26 blunt and 22 penetrating),the median time from presentation to ERCP was 38 d and only seven patients had a stent inserted for a pancreatic fistula (7) and a MPD stricture (1),whereby all patients avoided surgery[16].While variable complications have been reported,the heterogeneity of presentations at different centers must be considered.The studies mentioned above did not employ,early intraoperative ERCP.
The logistics of performing intraoperative ERCP can limit its use,especially in cases of poly-trauma.Wise use of this novel technique requires commitment and flexibility from the surgeons and gastroenterologists.In instances of trauma,PD injury,duodenal injury and papilla edema may also increase the difficulty of the procedure itself,thereby increasing the chances of complications such as post-ERCP pancreatitis[17].In both of our cases,there were no immediate or long term complications from the ERCP.Patient 1 did require upsizing from 5 Fr to 7 Fr stent,which is commonly seen.ERCP may be underutilized due to operator comfortability,lack of awareness of the value of endoscopic treatment in this setting,and equipment availability in the OR.Our high-volume trauma center is unique and is equipped to handle these situations with quick and effective mobilization of resources including on call therapeutic endoscopy.
CONCLUSION
“If you can’t allow your partner to have latitude26 in what he or she eats, then maybe your problem isn’t about food,” said Susan Jaffe, a psychiatrist in Manhattan
Knowing he felt this way, I decided4 one year to bypass the usual shirts, sweaters, ties and so forth5. I reached for something special just for Mike. The inspiration came in an unusual way.
Following the diagnostic ERCP,the first patient,underwent a pancreatic sphincterotomy followed by plastic pancreatic stent placement (5 Fr by 10 cm) (Figure 5).The main pancreatic duct (MPD) was intact.There were no technical challenges or associated complications from the procedure itself.The time from admission to ERCP was 6.35 h (Table 1).A drain was placed,and output decreased from 600 cc/d to 300 cc/d over two days.The drain amylase level was > 24000 units
L.Six days after the ERCP,his labs improved with an AST 46,ALT 77,ALP 89,and a total bilirubin 0.3.His hospital course was protracted related to non-pancreatic complications.He developed an intra-abdominal abscess communicating with the right abdominal wall wound.A CT abdomen pelvis did not show signs of a leak.However,he underwent a repeat ERCP with PD stent exchange to a larger 7 Fr by 10 cm plastic stent 18 d later due to a persistent leak on pancreatogram,with no further issues.
Blunt abdominal trauma.
In conclusion,this case series emphasizes the utility of intraoperative ERCP in cases of severe pancreatic trauma.Further studies are needed to clarify the optimal timing and safety outcomes in this setting.
Canakis A reviewed the literature and drafted manuscript;Kesar V,Hudspath C,Kim RE,and Darwin P participated in the therapeutic endoscopic care of the patient;Scalea TM was the patient’s trauma surgeon;Darwin P conceptualized the case series idea;Darwin P and Scalea TM provided critical revisions;all authors have read and approve the final manuscript.
Informed Consent was obtained for this case series.
Raymond Kim is a consultant to Medtronic and Cook medical.All other authors have no potential conflicts (financial,professional,or personal) that are relevant to the content presented in this manuscript.
The authors have read the CARE Checklist (2016),and the manuscript was prepared and revised according to the CARE Checklist (2016).
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
United States
Andrew Canakis 0000-0002-6646-6693;Varun Kesar 0000-0002-2422-0249;Caleb Hudspath 0000-0003-3321-5182;Raymond E Kim 0000-0003-3057-8316;Thomas M Scalea 0000-0001-8794-4108;Peter Darwin 0000-0002-3049-393x.
Zhang H
A
I hope we ve got what it takes to make our love last. As a bride, I had Scott s wedding band engraved17 with Robert Browning s line Grow old along with me! We re following those instructions.
Zhang H
1 Rogers SJ,Cello JP,Schecter WP.Endoscopic retrograde cholangiopancreatography in patients with pancreatic trauma.
2010;68:538-544 [PMID:20016385 DOI:10.1097/TA.0b013e3181b5db7a]
2 Ho VP,Patel NJ,Bokhari F,Madbak FG,Hambley JE,Yon JR,Robinson BR,Nagy K,Armen SB,Kingsley S,Gupta S,Starr FL,Moore HR 3rd,Oliphant UJ,Haut ER,Como JJ.Management of adult pancreatic injuries:A practice management guideline from the Eastern Association for the Surgery of Trauma.
2017;82:185-199 [PMID:27787438 DOI:10.1097/TA.0000000000001300]
3 Ando Y,Okano K,Yasumatsu H,Okada T,Mizunuma K,Takada M,Kobayashi S,Suzuki K,Kitamura N,Oshima M,Suto H,Nobuyuki M,Suzuki Y.Current status and management of pancreatic trauma with main pancreatic duct injury:A multicenter nationwide survey in Japan.
2021;28:183-191 [PMID:33280257 DOI:10.1002/jhbp.877]
4 Schellenberg M,Inaba K,Bardes JM,Cheng V,Matsushima K,Lam L,Benjamin E,Demetriades D.Detection of traumatic pancreatic duct disruption in the modern era.
2018;216:299-303 [PMID:29910071 DOI:10.1016/j.amjsurg.2018.06.002]
5 Phelan HA,Velmahos GC,Jurkovich GJ,Friese RS,Minei JP,Menaker JA,Philp A,Evans HL,Gunn ML,Eastman AL,Rowell SE,Allison CE,Barbosa RL,Norwood SH,Tabbara M,Dente CJ,Carrick MM,Wall MJ,Feeney J,O'Neill PJ,Srinivas G,Brown CV,Reifsnyder AC,Hassan MO,Albert S,Pascual JL,Strong M,Moore FO,Spain DA,Purtill MA,Edwards B,Strauss J,Durham RM,Duchesne JC,Greiffenstein P,Cothren CC.An evaluation of multidetector computed tomography in detecting pancreatic injury:results of a multicenter AAST study.
2009;66:641-6;discussion 646 [PMID:19276732 DOI:10.1097/TA.0b013e3181991a0e]
6 Fulcher AS,Turner MA,Yelon JA,McClain LC,Broderick T,Ivatury RR,Sugerman HJ.Magnetic resonance cholangiopancreatography (MRCP) in the assessment of pancreatic duct trauma and its sequelae:preliminary findings.
2000;48:1001-1007 [PMID:10866243 DOI:10.1097/00005373-200006000-00002]
7 Bhasin DK,Rana SS,Rawal P.Endoscopic retrograde pancreatography in pancreatic trauma:need to break the mental barrier.
2009;24:720-728 [PMID:19383077 DOI:10.1111/j.1440-1746.2009.05809.x]
8 Larsen M,Kozarek R.Management of pancreatic ductal leaks and fistulae.
2014;29:1360-1370 [PMID:24650171 DOI:10.1111/jgh.12574]
9 Anand RJ,Ferrada PA,Darwin PE,Bochicchio GV,Scalea TM.Endoscopic retrograde cholangiopancreatography is an effective treatment for bile leak after severe liver trauma.
2011;71:480-485 [PMID:21206287 DOI:10.1097/TA.0b013e3181efc270]
10 Barkin JS,Ferstenberg RM,Panullo W,Manten HD,Davis RC Jr.Endoscopic retrograde cholangiopancreatography in pancreatic trauma.
1988;34:102-105 [PMID:2452762 DOI:10.1016/s0016-5107(88)71272-9]
11 Kim HS,Lee DK,Kim IW,Baik SK,Kwon SO,Park JW,Cho NC,Rhoe BS.The role of endoscopic retrograde pancreatography in the treatment of traumatic pancreatic duct injury.
2001;54:49-55 [PMID:11427841 DOI:10.1067/mge.2001.115733]
12 Kim S,Kim JW,Jung PY,Kwon HY,Shim H,Jang JY,Bae KS.Diagnostic and therapeutic role of endoscopic retrograde pancreatography in the management of traumatic pancreatic duct injury patients:Single center experience for 34 years.
2017;42:152-157 [PMID:28343030 DOI:10.1016/j.ijsu.2017.03.054]
13 Halvorson L,Halsey K,Darwin P,Goldberg E.The safety and efficacy of therapeutic ERCP in the pediatric population performed by adult gastroenterologists.
2013;58:3611-3619 [PMID:24026405 DOI:10.1007/s10620-013-2857-9]
14 Canty TG Sr,Weinman D.Treatment of pancreatic duct disruption in children by an endoscopically placed stent.
2001;36:345-348 [PMID:11172431 DOI:10.1053/jpsu.2001.20712]
15 Lin BC,Liu NJ,Fang JF,Kao YC.Long-term results of endoscopic stent in the management of blunt major pancreatic duct injury.
2006;20:1551-1555 [PMID:16897285 DOI:10.1007/s00464-005-0807-0]
16 Thomson DA,Krige JE,Thomson SR,Bornman PC.The role of endoscopic retrograde pancreatography in pancreatic trauma:a critical appraisal of 48 patients treated at a tertiary institution.
2014;76:1362-1366 [PMID:24854301 DOI:10.1097/TA.0000000000000227]
17 Cheng CL,Sherman S,Watkins JL,Barnett J,Freeman M,Geenen J,Ryan M,Parker H,Frakes JT,Fogel EL,Silverman WB,Dua KS,Aliperti G,Yakshe P,Uzer M,Jones W,Goff J,Lazzell-Pannell L,Rashdan A,Temkit M,Lehman GA.Risk factors for post-ERCP pancreatitis:a prospective multicenter study.
2006;101:139-147 [PMID:16405547 DOI:10.1111/j.1572-0241.2006.00380.x]
杂志排行
World Journal of Gastrointestinal Endoscopy的其它文章
- Acute upper gastrointestinal bleeding:A stitch on time saves nine
- Why is endosonography insufficient for residual diagnosis after neoadjuvant therapy for esophageal cancer? Solutions using muscle layer evaluation
- Endoscopic ultrasonography drainage and debridement of an infected subcapsular hepatic hematoma:A case report
- Recognition of esophagitis in endoscopic images using transfer learning
- Lessons learned:Preventable misses and near-misses of endoscopic procedures
- Endobiliary biopsy