Lessons learned:Preventable misses and near-misses of endoscopic procedures
2022-05-18AllaTurshudzhyanHoumanRezaizadehMichealTadros
INTRODUCTION
Today,endoscopy is considered one of the best diagnostic tools for screening and surveillance of gastrointestinal pathology.Since the beginning of the 21
century,endoscopy use has risen by more than 50%[1].With wider utilization of endoscopy,it has become more and more evident that the procedure quality is multifactorial and operator dependent[2].Consequently,lesions may be missed depending on the level of provider training,procedural skills,and attentiveness to subtle pathology.This prompted development of several quality metrics to provide guidance for operators[3-7].Despite proposed quality metrics,there is still a significant number of missed gastrointestinal cancers.A metaanalysis by Menon
[8] suggested that 11.3% of upper gastrointestinal (UGI) neoplasms are overlooked on the initial upper endoscopy (EGD).Around 2.1%-5.9% of colorectal polyps or cancers are missed on colonoscopy[9].The difference likely stems from the fact that endoscopic training has historically put emphasis on colorectal cancer prevention and screening,while there is usually less awareness around UGI neoplasms.
It should be noted that aside from neoplastic lesions,bleeding sources can be missed on endoscopy and only seen on repeat examination in patients with unexplained occult GI bleed or iron deficiency anemia with negative diagnostic work up[10].Missed lesions on endoscopy are a common reason for malpractice lawsuits[11],which further emphasizes the importance of quality improvement.Some of the common reasons for why pathology is overlooked are a hastily performed endoscopy that bypasses proper visualization of the scope’s entry and exit points,not taking endoscopic exam to completion,and not visualizing more distal bowel segments.
REVIEW
Using our personal experience with 4 patients who had lesions missed or near missed on endoscopy,we hope to expose some of the weaknesses and shortcomings of endoscopy.Our goal is to bring the attention of other gastroenterologists to these commonly missed areas that may go undetected.
Case 1
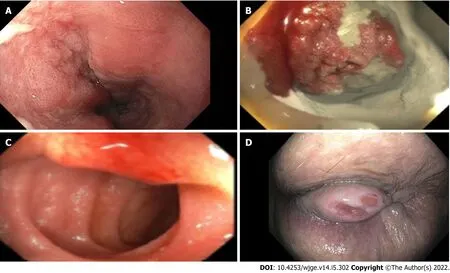
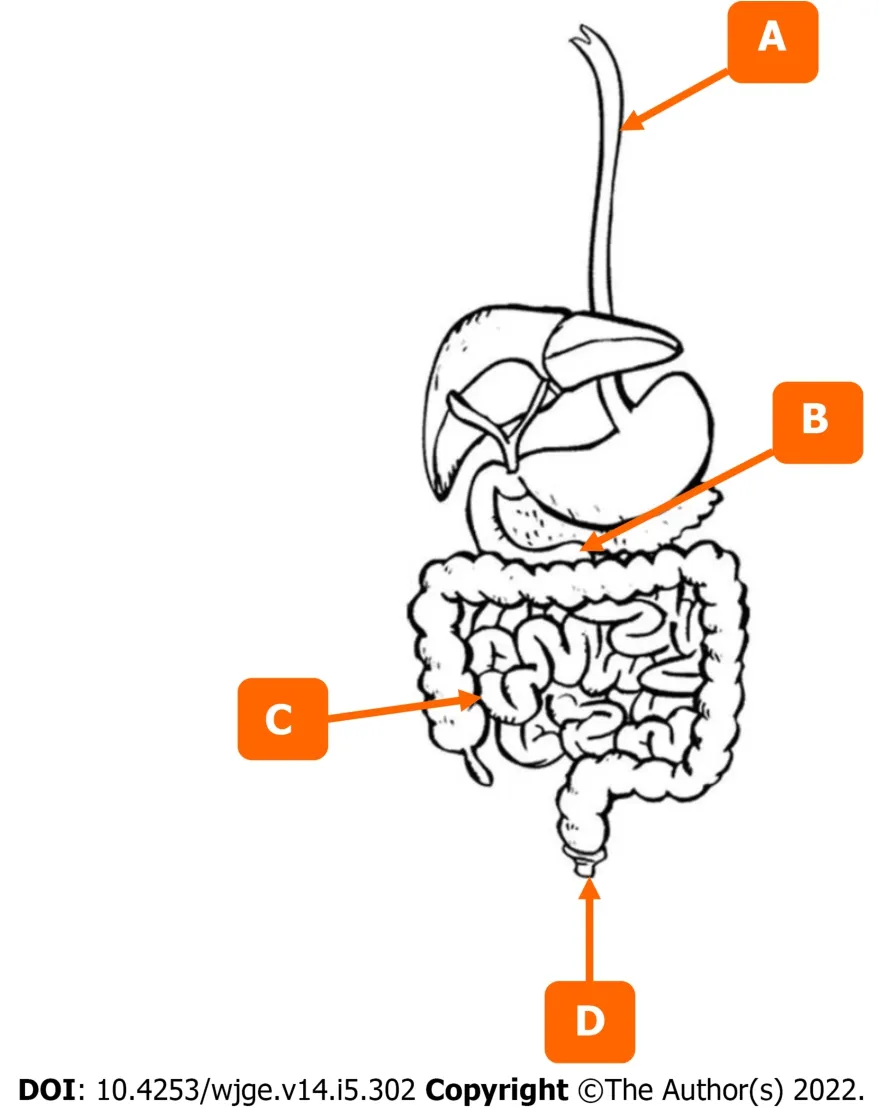
The first patient was a 72-year-old male who presented with symptoms of dysphagia.The initial EGD was unrevealing.It was only after the second EGD that a flat squamous cell carcinoma was appreciated 2 cm below the upper esophageal sphincter (UES) (Figure 1A,Figure 2A).The lesion was missed on the initial scope insertion and was likely missed because of a rapid scope withdrawal.
Case 2
The second patient was a 40-year-old female with iron deficiency anemia requiring multiple blood transfusions.The patient had undergone multiple upper and lower endoscopies and a capsule study,all of which were unrevealing.It was only after the 4
portion of the duodenum was examined that a malignant gastrointestinal stromal tumor was identified,diagnosed,and resected (Figures 1B and 2B).
It was the first hour of her awakening, full of anguish andhorror. Superstition made her alternately shudder with cold or burnwith the heat of fever. Many things, of which she had feared even tospeak, came into her mind. Silently, as the cloud-shadows in themoonshine, a spectral apparition flitted by her; she had heard of itbefore. Close by her galloped four snorting steeds, with fire flashingfrom their eyes and nostrils. They dragged a burning coach, and within it sat the wicked lord of the manor, who had ruled there a hundred years before. The legend says that every night, at twelve o clock, he drove into his castleyard and out again. He was not as pale as dead men are, but black as a coal. He nodded, and pointed to Anne Lisbeth, crying out, Hold fast! hold fast! and then you may ride again in a nobleman s carriage, and forget your child.
Case 3
As we learn more about common pitfalls and shortcomings of endoscopy,training fellows to recognize them becomes the next key step.It is important to standardize best practices and shed light on the areas commonly missed in colonoscopy training[33].One of the studies even suggested that pre-fellowship exposure to best practices of endoscopy,can improve the learning period and procedural skill of fellows[34].
Case 4
Our last patient was a 68-year-old with a history of cirrhosis and recurrent bright red blood per rectum.She had 2 colonoscopies done to find the bleeding source,both were unrevealing.It was months later that the patient had a 2 cm anal growth examined and diagnosed on careful retroflexion.The anal lesion was then seen on a reinspection of the anal area.(Figures 1D and 2D).
DISCUSSION
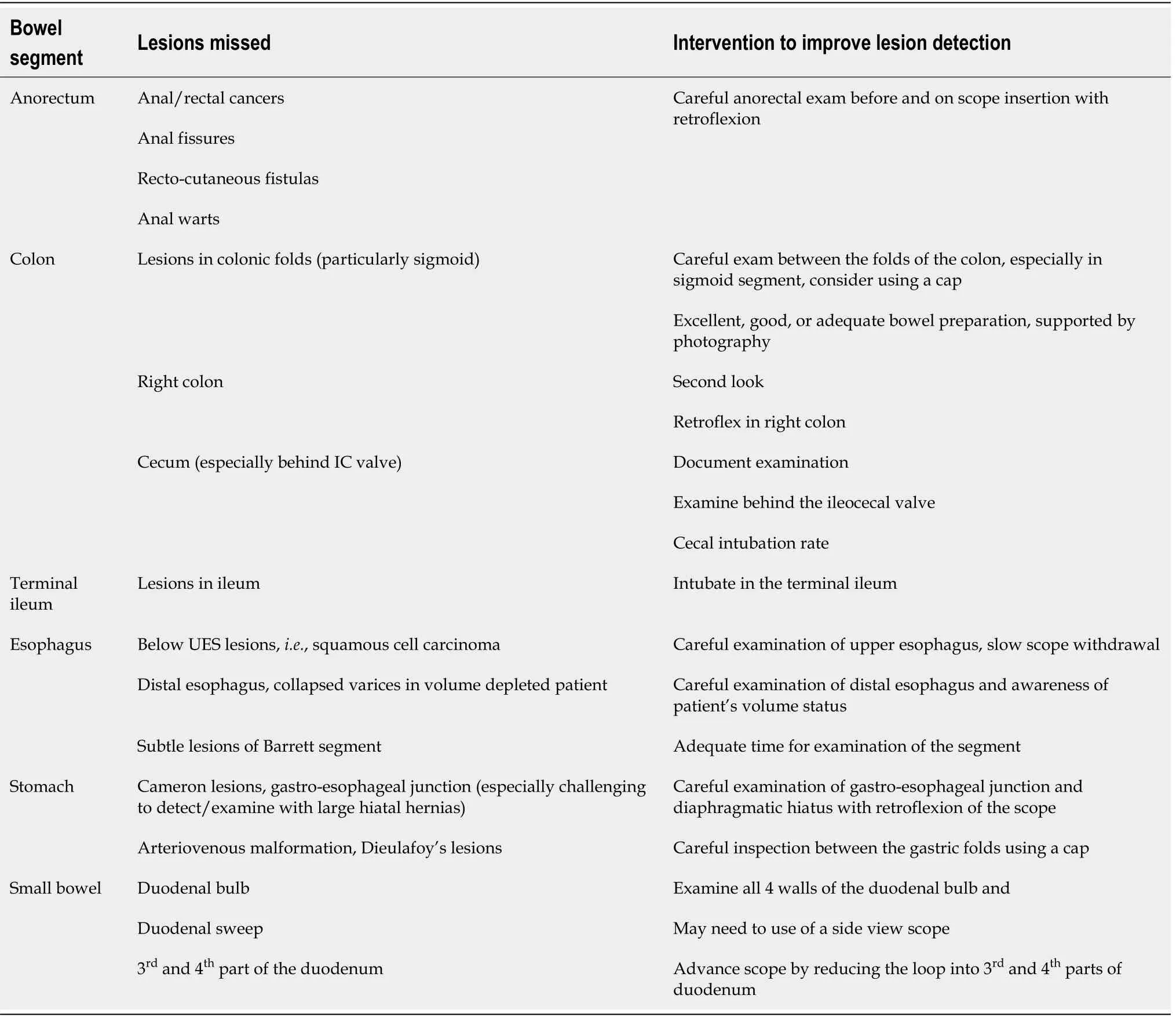
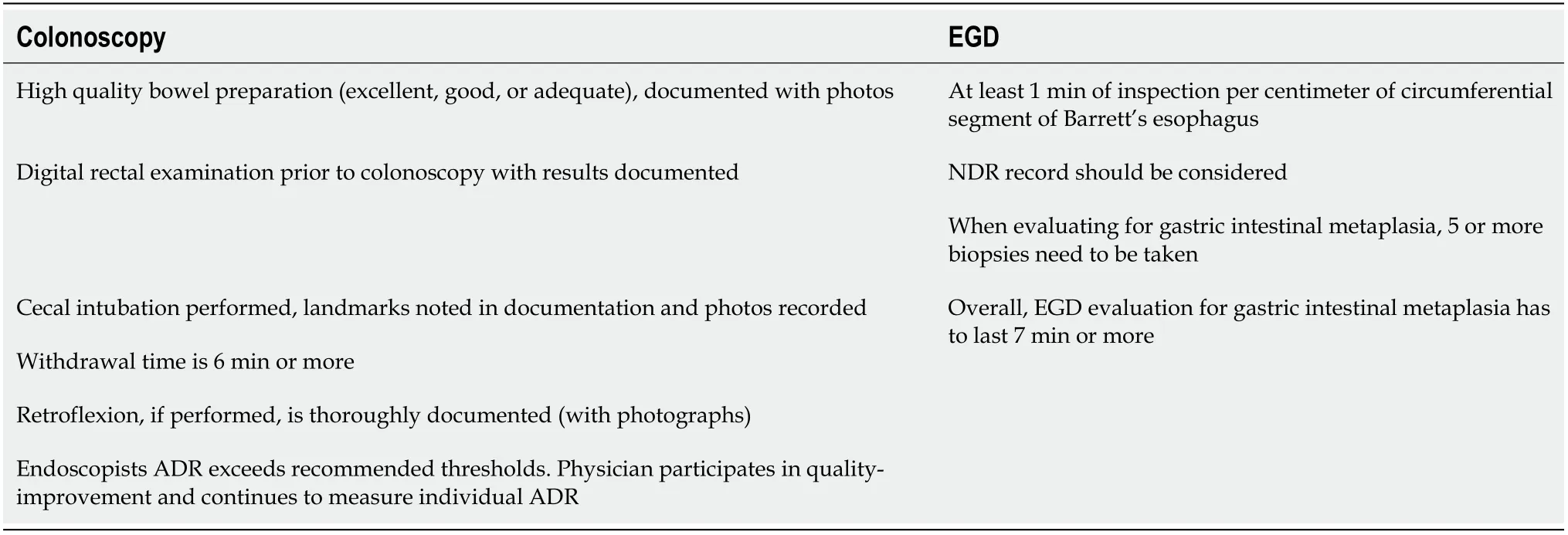
Increasing awareness of the bowel segments at risk for being missed on endoscopy is important.Similarly,it is important to incorporate technical maneuvers that could help identify these challenging lesions into fellowship training and post-graduate courses to help practicing endoscopists (Tables 1 and 2)[10].Lastly,following the most recent endoscopy quality metrics will help improve the detection of challenging lesions.
Colonoscopy
A complete colonoscopy should include a thorough exam of the endoscope’s entry point (anal canal),all segments of the colon,and,if possible,the distal ileum.We are going to discuss distal to proximal bowel segments as visualized on colonoscopy and use it as a framework to go over commonly missed lesions for each segment along with maneuvers and techniques that can help detect them.
Some of the common gastric lesions missed on EGD are Cameron lesions,lesions around gastro-esophageal (GE) junction (especially with large hiatal hernias),arteriovenous malformations,Dieulafoy lesions (Table 1).Some interventions that can be done are careful inspection of GE and diaphragmatic hiatus with retroflexion of the scope,inspection between gastric folds using the previously discussed cap-assisted endoscopy (Table 1)[23].One of the EGD quality metrics that is important to remember is adequate number of gastric biopsies,which should be greater or equal to 5[24].Timing is another important quality metric.Examination time during EGD when looking for intestinal metaplasia should be longer than 7 min,because longer inspection implies a more careful exam and results in a higher rate of neoplasia detection[25].Park
[25] observed that slow endoscopists (defined as withdrawal time of more than 3 min) were better at detecting neoplastic lesions (0.28%) compared to fast endoscopists (0.20%).As a result,they proposed that examination time could be a surrogate measure for the procedure quality[25].Another study identified that endoscopist who takes more than 7 min to complete exams is more likely to detect a high-risk gastric lesion when compared to a fast endoscopist[26].Given heterogeneity of data between the two studies,it is difficult to draw conclusions regarding the optimal examination time.This is further complicated by the fact that longer endoscopic times are associated with cardiac arrythmias,esophageal tears,aspiration,and bacterial translocation[27].
Captain Rondon took us into parts of the South Bronx that make Harlem look like Beverly Hills. When we arrived, we went into a store where we bought a lot of food and some baskets. We packed enough for seven families for thirty days. Then we went out to start feeding people. We went to buildings where there were half a dozen people living in one room: squatters with no electricity and no heat in the dead of winter surrounded by rats, cockroaches5 and the smell of urine. It was both an astonishing realization6 that people lived this way and a truly fulfilling experience to make even a small difference.
The astonished Prince stepped into the boat, and, holding the wolf s tail in his hand, he steered31 boldly out into the open sea, where the sun was gilding32 the blue waves with its golden rays
Second look examination of the right side of the colon can help reduce the rate of cecal lesions missed[16].Retroflexion in the right colon is another maneuver that can enhance visualization of right-sided lesions and improve ADR[14,16].It entails bending of the scope in a
-turn such that viewing lens is facing backwards[14].
Cecum intubation is a very important skill and a quality measure that can enhance visualization of the cecum and identify lesions that are oftentimes missed.Additionally,endoscopists should pay particular attention to the mucosa behind the IC valve.Documentation of cecal landmarks is crucial.
My first Thanksgiving in prison, I refused to eat. My first birthday I spent alternating between rage and feeling more sorry for myself than ever before. On Christmas, I wouldn t even get out of bed. I stayed under the covers to hide the tears I cried all day.
Some of the most commonly missed esophageal lesions are immediately below the UES and lesions in the distal esophagus (such as collapsed varices in a volume depleted patient or subtle changes of Barrett’s segment) (Table 1)[10].Some possible interventions to facilitate detection of challenging lesions are careful examination of the full length esophagus paying particular attention to upper and lower most segments,being aware of patient’s volume status,and allotting adequate time for examination of the segment (Table 1).Quality metrics for Barrett’s segment inspection time call for 1 minute inspection time per cm of circumferential length[21].Longer inspection time results in a more careful visualization of the mucosa and subsequently increase chances of detecting pathology[21].Another quality metric that is being proposed when examining esophagus is neoplasia detection rate (NDR)[22].Like ADR for colonoscopy,it is important to keep track of NDR for EGD when examining for Barrett’s segment,because it reflects the quality of inspection[22].
The optimal withdrawal time for colonoscopy remains an important topic.A 6-minute withdrawal time was accepted,but a recent meta-analysis by Bhurwal
[17] of 69551 patients compared withdrawal time of 6
9 min in its ability to detect adenomas.They found that odds ratio for ADR was significantly higher at 1.54 for colonoscopies with withdrawal time of 9 min or more[17].
Incidence of gastric pathology varies in different countries.There is higher prevalence of gastric cancer in Eastern countries.Consequently,this led to increased awareness of gastric lesions and a more robust screening protocols in countries like Japan[28].In Japan,it is recommended to undergo annual upper endoscopy for anybody over the age 40.As a result,there are more early-stage gastric lesions (53%) identified when compared to United States (27%)[29,30].This shows that increased awareness and adequate training can improve subtle lesion detection.
Upper endoscopy
A complete EGD should entail a thorough exam of the esophagus,including the UES,point of entry into the stomach,other poorly visualized areas of the stomach,along with all segments of the duodenum.We are going to discuss distal to proximal bowel segments as visualized on EGD and use it as a framework to go over commonly missed lesions for each segment along with maneuvers and techniques to help detect them.
Some of the commonly missed lesion of colonic segment include lesions found inside the colonic folds (especially in sigmoid colon),right-sided colon,cecum [especially behind the ileocecal (IC) valve],and distal ileum (Table 1).There are a few techniques that can be implemented to facilitate detection of these challenging lesions (Table 1).Endoscopists should do a thorough examination between the haustral folds to avoid missing even large polyps that can hide inside the folds.Cap-assisted colonoscopy is another acceptable option as it involves a transparent attachment at the end of the scope that can improve adenoma detection rate (ADR) by flattening of the haustral folds and improving visualization of mucosa,especially on scope withdrawal[15].
All maneuvers discussed need to be thoroughly photographed and documented in the procedure description per the colonoscopy quality metrics (Table 2).Quality metrics further require bowel preparation to be excellent,good,or adequate and supported by photography and withdrawal time should be noted in documentation and exceed 6 minutes[11].It is also encouraged that practicing endoscopist’s adenoma detection rate (ADR) exceeds recommended thresholds.Physicians should routinely measure their ADR and participate in quality improvement programs[11].
Some of the commonly missed lesions in anorectum are anal and rectal cancer,anal fissures,recto cutaneous fistulas,anal warts (Table 1)[10].This is likely because of the scopes entry point being overlooked or not property visualized at the beginning of the procedure.The importance of anal examination by a skilled endoscopist if further emphasized by the fact that anorectal lesions can have a non-specific presentation and may go undiagnosed by patient’s primary care physician.Chiu
[12] found that only 54% of patients have a rectal examination by their primary care provider when they present with a non-specific anal complaint.Another study indicated that only 23% of patients presenting with anal complaint were diagnosed correctly by their primary care provider;the remaining patients were erroneously diagnosed with hemorrhoids[13].As a result,this leads to delay in diagnosis and management of anal and rectal cancers.As proposed by quality metrics,digital rectal exam needs to be performed and thoroughly documented prior to colonoscopy (Table 2)[11].Another maneuver that could be used to enhance detection of challenging lesions in anorectum is retroflexion.It allows for a better visualization of distal rectum and distal anus (Table 1)[14].Retroflexion needs to be photographed and documented[11].
Lesions can be missed in terminal ileum as many colonoscopies do not investigate this bowel segment.It is important to note that the ileum is the most common site for development of carcinoid tumors (57%) and that even primary ileal tumors are missed on computer tomography (CT) scans in 64% of cases[18-20].This emphasizes the importance of a thorough and complete endoscopic exam that may detect primary ileal tumors early and allow for timely intervention[20].Endoscopists should try to intubate the terminal ileum whenever feasible.
Duodenum
Some of the commonly missed segments of the small bowel are duodenal bulb,duodenal sweep,and 3
and 4
parts of the duodenum (Table 1).Some of the maneuvers that can help detect these challenging lesions are careful examination of all 4 walls of the duodenal bulb,use of a side view scope for the duodenal sweep,advancement of the scope by reducing the loop into the 3
and 4
parts of duodenum (Table 1).Many upper endoscopies do not go past the 2
part of the duodenum.Lesions in more distal segments of the duodenum (3
and 4
) are usually more challenging to visualize and require an extralog fiber optic scope and a trained endoscopist[31].Interestingly,60% of benign duodenal lesions and 50% of malignant duodenal lesions are only diagnosed on autopsy and missed on the endoscopic exam[32].
TRAINING
The third patient was a 50-year-old female who presented with ongoing diarrhea.Stool studies revealed cryptosporidium.Fortunately,the patient’s colonoscopy included examination of the terminal ileum and was able to detect a small submucosal carcinoid tumor (Figures 1C and 2C).It was successfully resected with metastatic disease noted in only one lymph node.
The Cat s master did not build very much upon what he said. He had often seen him play a great many cunning tricks to catch rats and mice,15 as when he used to hang by the heels, or hide himself in the meal, and make as if he were dead; so that he did not altogether despair of his affording him some help in his miserable condition. When the Cat had what he asked for he booted himself very gallantly, and putting his bag about his neck, he held the strings of it in his two forepaws and went into a warren16 where was great abundance of rabbits. He put bran and sow-thistle into his bag, and stretching out at length, as if he had been dead, he waited for some young rabbits, not yet acquainted with the deceits of the world, to come and rummage his bag for what he had put into it.
ARTIFICIAL INTELLIGENT in ENDOSCOPY
Endoscopy continues to be an operator dependent procedure.As such,it presents a growing opportunity for development of machine learning technology and computer algorithms to assist endoscopists with lesion detection.Artificial intelligent (AI) has a promise to improve accuracy of endoscopic procedures,reduce inter-operator variability,and compensate for human error and factors contributing to it such as fatigue or limited experience[35].Thus far,computer-aided detection algorithms of AI have been trained to detect lesions both macroscopically and by optical biopsy/ microscopically[36].Recent studies demonstrated that AI performed better than endoscopists in esophageal cancer and neoplasm detection in pooled sensitivity 94%
82%,respectively[37].The specificity of AI-based endoscopy had specificity of 85% for esophageal cancer and neoplasms[37].AIbased endoscopy provided a 26.5% increase in sensitivity for detection of early gastric cancer when compared to endoscopists (sensitivity of 95%)[38].The specificity of AI-based endoscopy had specificity of 87.3% for early gastric cancer[38].AI algorithms have also been targeted towards colorectal cancer detection.Recent reports suggest that AI-assisted colonoscopy has sensitivity of 94% [39,40].While some reports suggest that AI may not show significant improvement in larger polyp detection rate (38.8%
26.2%),AI-based colonoscopy showed significant improvement in detection of small and flat polyps that are easily missed (76.0%
68.8% and 5.9%
3.3%,respectively)[41].
CONCLUSION
Endoscopy has developed into a sophisticated diagnostic tool that provides great accuracy in lesion detection,but it is not perfect and remains operator dependent.The cases we presented expose weaknesses and shortcomings of endoscopic examination for both the upper and lower gastrointestinal tract,providing an opportunity for improvement.Commonly missed areas and the reason for why they were missed need to be communicated to currently practicing gastroenterologists.Additionally,educating fellows during their training on the possible shortcomings and weaknesses of endoscopy may help improve the quality of procedures in the future.
Turshudzhyan A wrote the letter,Rezaizadeh H and Tadros M critically revised the manuscript.
Okay, he said, helping10 me down the stairs and to the curb11, I m going to stay here and keep an ear out for the babies. I ll tell you when it s safe to cross. You go over to the coke machine, get your coke and come back out. Wait for me to tell you when it s safe to cross back.
So the first thing he did was to search the house for materials to make an ointment23, which he sprinkled plentifully24 with pepper and then put in his pocket
Rezaizadeh H has financial interest associated with AstraZeneca and research funding/interest associated with Celgene/Bristol Meyers Squibb.
I have a daughter, 7 said the old woman, who is so beautiful that she has not her equal in the world,8 and is well fitted to be your wife; if you will make her lady-queen9 I will show you the way out of the wood.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
United States
Alla Turshudzhyan 0000-0001-6867-7569;Houman Rezaizadeh 0000-0002-1066-5394;Micheal Tadros 0000-0003-3118-3893.
Xing YX
A
He lived very merrily; he went every night to the theatre, made paper kites out of five-pound notes, and played ducks and drakes with sovereigns instead of stones
Xing YX
1 Peery AF,Dellon ES,Lund J,Crockett SD,McGowan CE,Bulsiewicz WJ,Gangarosa LM,Thiny MT,Stizenberg K,Morgan DR,Ringel Y,Kim HP,DiBonaventura MD,Carroll CF,Allen JK,Cook SF,Sandler RS,Kappelman MD,Shaheen NJ.Burden of gastrointestinal disease in the United States:2012 update.
2012;143:1179-1187.e3 [PMID:22885331 DOI:10.1053/j.gastro.2012.08.002]
2 Januszewicz W,Kaminski MF.Quality indicators in diagnostic upper gastrointestinal endoscopy.
2020;13:1756284820916693 [PMID:32477426 DOI:10.1177/1756284820916693]
3 Beg S,Ragunath K,Wyman A,Banks M,Trudgill N,Pritchard DM,Riley S,Anderson J,Griffiths H,Bhandari P,Kaye P,Veitch A.Quality standards in upper gastrointestinal endoscopy:a position statement of the British Society of Gastroenterology (BSG) and Association of Upper Gastrointestinal Surgeons of Great Britain and Ireland (AUGIS).
2017;66:1886-1899 [PMID:28821598 DOI:10.1136/gutjnl-2017-314109]
4 Bisschops R,Areia M,Coron E,Dobru D,Kaskas B,Kuvaev R,Pech O,Ragunath K,Weusten B,Familiari P,Domagk D,Valori R,Kaminski MF,Spada C,Bretthauer M,Bennett C,Senore C,Dinis-Ribeiro M,Rutter MD.Performance measures for upper gastrointestinal endoscopy:a European Society of Gastrointestinal Endoscopy (ESGE) Quality Improvement Initiative.
2016;48:843-864 [PMID:27548885 DOI:10.1055/s-0042-113128]
5 Park WG,Shaheen NJ,Cohen J,Pike IM,Adler DG,Inadomi JM,Laine LA,Lieb JG 2nd,Rizk MK,Sawhney MS,Wani S.Quality indicators for EGD.
2015;110:60-71 [PMID:25448872 DOI:10.1038/ajg.2014.384]
6 ASGE Endoscopy Unit Quality Indicator Taskforce,Day LW,Cohen J,Greenwald D,Petersen BT,Schlossberg NS,Vicari JJ,Calderwood AH,Chapman FJ,Cohen LB,Eisen G,Gerstenberger PD,Hambrick RD 3rd,Inadomi JM,MacIntosh D,Sewell JL,Valori R.Quality indicators for gastrointestinal endoscopy units.
2017;2:119-140 [PMID:29905282 DOI:10.1016/j.vgie.2017.02.007]
7 Rex DK,Schoenfeld PS,Cohen J,Pike IM,Adler DG,Fennerty MB,Lieb JG 2nd,Park WG,Rizk MK,Sawhney MS,Shaheen NJ,Wani S,Weinberg DS.Quality indicators for colonoscopy.
2015;81:31-53 [PMID:25480100 DOI:10.1016/j.gie.2014.07.058]
8 Menon S,Trudgill N.How commonly is upper gastrointestinal cancer missed at endoscopy?
2014;2:E46-E50 [PMID:26135259 DOI:10.1055/s-0034-1365524]
9 Bressler B,Paszat LF,Chen Z,Rothwell DM,Vinden C,Rabeneck L.Rates of new or missed colorectal cancers after colonoscopy and their risk factors:a population-based analysis.
2007;132:96-102 [PMID:17241863 DOI:10.1053/j.gastro.2006.10.027]
10 Tadros M,Wu GY.Management of occult gi bleeding a clinical guide.Cham:Springer International Publishing;2021
11 Rex DK.Avoiding and defending malpractice suits for postcolonoscopy cancer:advice from an expert witness.
2013;11:768-773 [PMID:23376796 DOI:10.1016/j.cgh.2013.01.027]
12 Chiu S,Joseph K,Ghosh S,Cornand RM,Schiller D.Reasons for delays in diagnosis of anal cancer and the effect on patient satisfaction.
2015;61:e509-e516 [PMID:26889506]
13 Edwards AT,Morus LC,Foster ME,Griffith GH.Anal cancer:the case for earlier diagnosis.
1991;84:395-397 [PMID:1865443]
14 Rex DK,Vemulapalli KC.Retroflexion in colonoscopy:why?
2013;144:882-883 [PMID:23499952 DOI:10.1053/j.gastro.2013.01.077]
15 Pohl H,Bensen SP,Toor A,Gordon SR,Levy LC,Berk B,Anderson PB,Anderson JC,Rothstein RI,MacKenzie TA,Robertson DJ.Cap-assisted colonoscopy and detection of Adenomatous Polyps (CAP) study:a randomized trial.
2015;47:891-897 [PMID:26126162 DOI:10.1055/s-0034-1392261]
16 Ai X,Qiao W,Han Z,Tan W,Bai Y,Liu S,Zhi F.Results of a second examination of the right side of the colon in screening and surveillance colonoscopy:a systematic review and meta-analysis.
2018;30:181-186 [PMID:29232250 DOI:10.1097/MEG.0000000000001009]
17 Bhurwal A,Rattan P,Sarkar A,Patel A,Haroon S,Gjeorgjievski M,Bansal V,Mutneja H.A comparison of 9-min colonoscopy withdrawal time and 6-min colonoscopy withdrawal time:A systematic review and meta-analysis.
2021;36:3260-3267 [PMID:34617312 DOI:10.1111/jgh.15701]
18 Baxi AJ,Chintapalli K,Katkar A,Restrepo CS,Betancourt SL,Sunnapwar A.Multimodality Imaging Findings in Carcinoid Tumors:A Head-to-Toe Spectrum.
2017;37:516-536 [PMID:28287937 DOI:10.1148/rg.2017160113]
19 Modlin IM,Lye KD,Kidd M.A 5-decade analysis of 13,715 carcinoid tumors.
2003;97:934-959 [PMID:12569593 DOI:10.1002/cncr.11105]
20 Gupta A,Lubner MG,Wertz RM,Foley E,Loeffler A,Pickhardt PJ.CT detection of primary and metastatic ileal carcinoid tumor:rates of missed findings and associated delay in clinical diagnosis.
2019;44:2721-2728 [PMID:31016344 DOI:10.1007/s00261-019-01945-0]
21 Gupta N,Gaddam S,Wani SB,Bansal A,Rastogi A,Sharma P.Longer inspection time is associated with increased detection of high-grade dysplasia and esophageal adenocarcinoma in Barrett's esophagus.
2012;76:531-538 [PMID:22732877 DOI:10.1016/j.gie.2012.04.470]
22 Parasa S,Desai M,Vittal A,Chandrasekar VT,Pervez A,Kennedy KF,Gupta N,Shaheen NJ,Sharma P.Estimating neoplasia detection rate (NDR) in patients with Barrett's oesophagus based on index endoscopy:a systematic review and meta-analysis.
2019;68:2122-2128 [PMID:30872393 DOI:10.1136/gutjnl-2018-317800]
23 Karaca C,Daglilar ES,Soyer OM,Gulluoglu M,Brugge WR.Endoscopic submucosal resection of gastric subepithelial lesions smaller than 20 mm:a comparison of saline solution-assisted snare and cap band mucosectomy techniques.
2017;85:956-962 [PMID:27663715 DOI:10.1016/j.gie.2016.09.016]
24 Dinis-Ribeiro M,Areia M,de Vries AC,Marcos-Pinto R,Monteiro-Soares M,O'Connor A,Pereira C,Pimentel-Nunes P,Correia R,Ensari A,Dumonceau JM,Machado JC,Macedo G,Malfertheiner P,Matysiak-Budnik T,Megraud F,Miki K,O'Morain C,Peek RM,Ponchon T,Ristimaki A,Rembacken B,Carneiro F,Kuipers EJ;European Society of Gastrointestinal Endoscopy;European Helicobacter Study Group;European Society of Pathology;Sociedade Portuguesa de Endoscopia Digestiva.Management of precancerous conditions and lesions in the stomach (MAPS):guideline from the European Society of Gastrointestinal Endoscopy (ESGE),European Helicobacter Study Group (EHSG),European Society of Pathology (ESP),and the Sociedade Portuguesa de Endoscopia Digestiva (SPED).
2012;44:74-94 [PMID:22198778 DOI:10.1055/s-0031-1291491]
25 Park JM,Huo SM,Lee HH,Lee BI,Song HJ,Choi MG.Longer Observation Time Increases Proportion of Neoplasms Detected by Esophagogastroduodenoscopy.
2017;153:460-469.e1 [PMID:28501581 DOI:10.1053/j.gastro.2017.05.009]
26 Teh JL,Tan JR,Lau LJ,Saxena N,Salim A,Tay A,Shabbir A,Chung S,Hartman M,So JB.Longer examination time improves detection of gastric cancer during diagnostic upper gastrointestinal endoscopy.
2015;13 :480-487.e2 [PMID:25117772 DOI:10.1016/j.cgh.2014.07.059]
27 Kavic SM,Basson MD.Complications of endoscopy.
2001;181:319-332 [PMID:11438266 DOI:10.1016/s0002-9610(01)00589-x]
28 Hanazaki K,Sodeyama H,Wakabayashi M,Miyazawa M,Yokoyama S,Sode Y,Kawamura N,Miyazaki T,Ohtsuka M.Surgical treatment of gastric cancer detected by mass screening.
1997;44:1126-1132 [PMID:9261611]
29 Theuer CP.Asian gastric cancer patients at a southern California comprehensive cancer center are diagnosed with less advanced disease and have superior stage-stratified survival.
2000;66:821-826 [PMID:10993608]
30 Theuer CP,Kurosaki T,Ziogas A,Butler J,Anton-Culver H.Asian patients with gastric carcinoma in the United States exhibit unique clinical features and superior overall and cancer specific survival rates.
2000;89:1883-1892 [PMID:11064344 DOI:10.1002/1097-0142(20001101)89:9<1883::aid-cncr3>3.3.co;2-8]
31 Markogiannakis H,Theodorou D,Toutouzas KG,Gloustianou G,Katsaragakis S,Bramis I.Adenocarcinoma of the third and fourth portion of the duodenum:a case report and review of the literature.
2008;1:98 [PMID:18706123 DOI:10.1186/1757-1626-1-98]
32 Kaminski N,Shaham D,Eliakim R.Primary tumours of the duodenum.
1993;69:136-138 [PMID:8506195 DOI:10.1136/pgmj.69.808.136]
33 Kumar NL,Smith BN,Lee LS,Sewell JL.Best Practices in Teaching Endoscopy Based on a Delphi Survey of Gastroenterology Program Directors and Experts in Endoscopy Education.
2020;18:574-579.e1 [PMID:31125782 DOI:10.1016/j.cgh.2019.05.023]
34 Kim DH,Park SJ,Cheon JH,Kim TI,Kim WH,Hong SP.Does a Pre-Training Program Influence Colonoscopy Proficiency during Fellowship?
2016;11:e0164360 [PMID:27764144 DOI:10.1371/journal.pone.0164360]
35 El Hajjar A,Rey JF.Artificial intelligence in gastrointestinal endoscopy:general overview.
2020;133:326-334 [PMID:31929362 DOI:10.1097/CM9.0000000000000623]
36 Li H,Hou X,Lin R,Fan M,Pang S,Jiang L,Liu Q,Fu L.Advanced endoscopic methods in gastrointestinal diseases:a systematic review.
2019;9:905-920 [PMID:31281783 DOI:10.21037/qims.2019.05.16]
37 Zhang SM,Wang YJ,Zhang ST.Accuracy of artificial intelligence-assisted detection of esophageal cancer and neoplasms on endoscopic images:A systematic review and meta-analysis.
2021;22:318-328 [PMID:33871932 DOI:10.1111/1751-2980.12992]
38 Ikenoyama Y,Hirasawa T,Ishioka M,Namikawa K,Yoshimizu S,Horiuchi Y,Ishiyama A,Yoshio T,Tsuchida T,Takeuchi Y,Shichijo S,Katayama N,Fujisaki J,Tada T.Detecting early gastric cancer:Comparison between the diagnostic ability of convolutional neural networks and endoscopists.
2021;33:141-150 [PMID:32282110 DOI:10.1111/den.13688]
39 Kominami Y,Yoshida S,Tanaka S,Sanomura Y,Hirakawa T,Raytchev B,Tamaki T,Koide T,Kaneda K,Chayama K.Computer-aided diagnosis of colorectal polyp histology by using a real-time image recognition system and narrow-band imaging magnifying colonoscopy.
2016;83:643-649 [PMID:26264431 DOI:10.1016/j.gie.2015.08.004]
40 Byrne MF,Chapados N,Soudan F,Oertel C,Linares Pérez M,Kelly R,Iqbal N,Chandelier F,Rex DK.Real-time differentiation of adenomatous and hyperplastic diminutive colorectal polyps during analysis of unaltered videos of standard colonoscopy using a deep learning model.
2019;68:94-100 [PMID:29066576 DOI:10.1136/gutjnl-2017-314547]
41 Xu L,He X,Zhou J,Zhang J,Mao X,Ye G,Chen Q,Xu F,Sang J,Wang J,Ding Y,Li Y,Yu C.Artificial intelligenceassisted colonoscopy:A prospective,multicenter,randomized controlled trial of polyp detection.
2021;10:7184-7193 [PMID:34477306 DOI:10.1002/cam4.4261]
杂志排行
World Journal of Gastrointestinal Endoscopy的其它文章
- Acute upper gastrointestinal bleeding:A stitch on time saves nine
- Intraoperative endoscopic retrograde cholangiopancreatography for traumatic pancreatic ductal injuries:Two case reports
- Why is endosonography insufficient for residual diagnosis after neoadjuvant therapy for esophageal cancer? Solutions using muscle layer evaluation
- Endoscopic ultrasonography drainage and debridement of an infected subcapsular hepatic hematoma:A case report
- Recognition of esophagitis in endoscopic images using transfer learning
- Endobiliary biopsy