Impact of vaccination on SARS-CoV-2 infection: Experience from a tertiary care hospital
2022-04-22NupurPalDebalinaNagJayeetaHalderAritraBiswasRajaRayAvijitHazraChitritaChatterjee
Nupur Pal, Debalina Nag, Jayeeta Halder, Aritra Biswas, Raja Ray, Avijit Hazra, Chitrita Chatterjee
1Department of Microbiology, Institute of Post-Graduate Medical Education & Research, Kolkata, India
2Department of Pharmacology, Institute of Post-Graduate Medical Education & Research, Kolkata, India
Ever since the world has been engulfed by the COVID-19 pandemic, caused by SARS-CoV-2 virus, humanity has gone through untold miseries. There has been a widespread impact on health, including substantial mortality and morbidity, especially among older adults and those with pre-existing health conditions[1,2],in addition to serious repercussions for the global economy, and social wellbeing. Despite this devastating spread of the virus, a large number of the population remains non-immune to SARS-CoV-2[3].With no approved cure in sight, hopes are pinned on safe and effective vaccines and their equitable distribution and acceptance for reigning in the pandemic. The vaccination campaign for COVID-19 in India was started on 16th January, 2021 using two vaccines, first with Covishield (AstraZeneca and Serum Institute of India) and later along with Covaxin (BBV152, Bharat Biotech and ICMR). Initially,health care workers and other front line workers were prioritized for vaccination, and then vaccinations for COVID-19 were started for all adults in India. We intended to find out the number of breakthrough COVID-19 infections after vaccination in a tertiary care hospital,Kolkata, India.
Data were collected retrospectively from 1st April 2021 to 8th July 2021 of all samples sent for testing of SARS-CoV-2 infection by RT-PCR in the Department of Microbiology of the study hospital.The timing was synchronous with the second and highest COVID-19 pandemic wave that emerged in India and attained its peak in the last week of April 2021, with reports of an average of 400 000 daily cases. We recorded all data regarding vaccination status, types and doses of vaccine received, duration between vaccination and onset of symptoms of COVID-19 to assess the effectiveness of vaccines.All data were verified twice and telephonic communications were conducted with infected individuals aimed to estimate the number of breakthrough COVID-19 infections in the vaccinated population using RT-PCR and evaluate the effectiveness of Covishield and Covaxin in respect to the incidence of infection, doses and time since vaccination to infection. We also took into account the demographical factors and impact of vaccination on health in a tertiary care hospital. GraphPad Prism software version 5 was employed for statistical analysis using Fisher’s exact test, Chi-square test, odds ratio (OR) and 95% confidence interval (CI). This study was approved by local ethics review board (IPGME&R/IEC/2021 I 575R Date:18.11.2021).
Out of total of 1 546 vaccinated persons who had received either single or double dose, 67 (4.33%) persons tested positive for COVID-19 which was much lower as compared to the nonvaccinated individuals where the positivity rate was 15.61% during the 2nd wave of this pandemic. This data is statistically significant (P<0.001) and odds ratio (OR) for RT-PCR positive non-vaccinated compared to vaccinated population was 4.08(95% CI 3.19-5.21) (Table1). Among 1 546 vaccinated population,735 were fully vaccinated and 811 received single-dose vaccine.Seventeen from fully vaccinated and 50 from partially vaccinated individuals became RT-PCR positive in the post-vaccination period.Comparison between non-vaccinated and fully vaccinated revealed significant results and non-vaccinated populations had 8 times more risk for contracting the virus than fully vaccinated persons(95% CI 4.94-12.94). As compared to partially vaccinated persons(1st dose), fully vaccinated persons (2nd dose) were also safer (OR 2.67, 95% CI 1.52-4.66). Among 1 546 vaccinated persons, 126 persons had received Covaxin (8%), 1 420 had received Covishield(92%). Out of 67 positive vaccinated people, 61 received Covishield(4.29%) while 6 received Covaxin (4.76%). Regarding age group and sex distribution among vaccinated positive persons, the olderage group (>60 year) was most susceptible (21/197, 10.65%) even after vaccination and the younger age group (18-44 year) were least susceptible (20/822, 2.43%) (P<0.001, OR 5.43, 95% CI 2.88-10.27).Comparison between sequential age bands by using the Chi-square test for trend showed a significant linear trend (P<0.001). This indicates increasing age increases the risk of getting infected. Female(30/476, 6.30%) were more susceptible than male (37/1047, 3.53%)after receiving vaccination (P<0.021). Out of total 67 positive, 17(17/67, 25.37%) had completed two doses of vaccination, among them, 10 were healthcare workers (10/17, 58.82%). Breakthrough infection occurred after 1 month of receiving the 2nd dose in 8 patients, after 2 months in 4 patients, after 3 months in 3 patients,and after 4 months in 2 patients. Out of the 50 persons (44 Covishield & 6 Covaxin) who had received only one dose of vaccine,24 tested positive within 4 weeks of vaccination, 14 tested positive after 1 month and 6 were positive after 2 months in the Covishield group, while all 6 people were positive within 4 weeks of the single dose vaccine in the Covaxin group. The median cycle threshold (CT)value among vaccinated RT-PCR positive people was 23. Among 67 vaccinated positive persons 17 (25.37%) were symptomatic and only 4 were hospitalized which was 5.9% of all vaccinated and 23.5% of all symptomatic RT-PCR positive people. Unfortunately, one death was recorded among all vaccinated positive individuals, who had received only a single dose of Covaxin and were diagnosed RT-PCR positive after 4 weeks of vaccination.
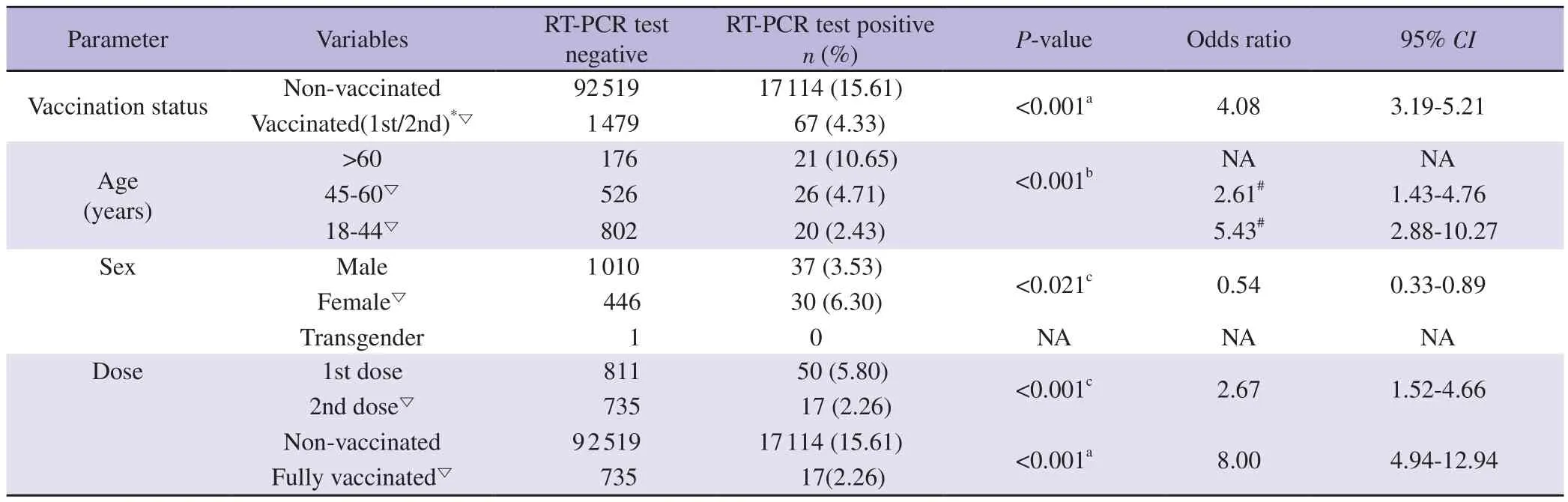
Table1. Comparison of COVID-19 positivity status between demographic and vaccination subgroups.
It is a matter of significant concern that vaccination may not be offering full protection from infection, hospitalization and death.A lot of people having both doses of Covishield and Covaxin were hospitalized after breakthrough infection, and few of them even died as per anecdotal reports but there is no actual published data so far.Our study aimed to assess the effectiveness of the Covishield and Covaxin in the general population as well as health care workers.Covishield vaccine was developed at Oxford University and consists of a replication-deficient chimpanzee adenoviral vector ChAdOx1,containing the SARS-CoV-2 structural surface glycoprotein antigen(spike protein; nCoV-19) gene. Covaxin is an inactivated whole virus vaccine, containing SARS-CoV-2 particles that have been chemically deactivated[4,5]. According to clinical trial reports both vaccines have effectiveness in decreasing the risk of getting COVID-19 infections by 70%-90%, and also vaccine efficacy against COVID-19 requiring hospital admission from three weeks after the first dose was 100%[4,5].
From our study, it can be concluded that the vaccinated population is safer compared to non-vaccinated individuals. The risk of contracting the virus is minimum in a fully vaccinated population as compared to partially vaccinated and non-vaccinated individuals which is quite similar to other studies[6-8]. Though Covishield is a more widely used vaccine in India, both Covishield and Covaxin vaccines are almost equally effective in preventing SARS-COV-2 infection. The average duration of post-vaccination RT-PCR positivity is 4 weeks after1st dose vaccination, it may be due to delayed activation of the primary immune response. Two thirds of our study population have an asymptomatic or mild infection,around 5.9% required hospitalization and one death was reported.It is possible that breakthrough infection could be attributed to COVID-19 variants bypassing the vaccine-induced immunity[7,8].
Our study showed significant difference between female and male.One study from Kerala, India also showed female preponderance over male[7]. The reason behind this gender difference is not known which needs further future research. Older age groups and healthcare workers formed the bulk of the population that tested positive inspite of complete vaccination which corroborates with other studies[7,9].Our study also showed that increasing age also increases the chance of getting infected. It is crucial to determine whether the effect of vaccines is influenced either by host factors such as age, sex, prior COVID-19 infection, other co-morbidities, or by vaccine factors such as type of vaccine, number of doses and interval of doses.There have also been concerns that these vaccines may be less effective against the B1617 variant of SARS-CoV-2, the strain that was identified as the main driver of the second wave of the pandemic in India[8,10]. These areas need to be investigated in further research.At the same time, continuous compliance with increased public awareness is essential to achieve optimum vaccination impact to mitigate the pandemic.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Authors’ contributions
NP prepared the final draft along with conceptualization,methodology and editing. DN collected data and wrote the first draft.RR and CC supervised and reviewed the manuscript. AH conducted all statistical analysis. JH and AB conducted the investigations and prepared methodology.
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- Vaccine equity: The need of the hour in the face of emerging SARS-CoV-2 variants
- World’s first malaria vaccine and its significance to malaria control in Africa
- Alternative mix-and-match COVID-19 vaccine administration versus standard vaccination for prevention of severe COVID-19: A specific cost utility analysis
- Furuncular myiasis by Wohlfahrtia magnifica (Diptera: Sarcophagidae) in a healthy child
- Evaluation of Cuban Bacillus thuringiensis (Berliner, 1911) (Bacillales: Bacillacea)isolates with larvicidal activity against Aedes aegypti (Linnaeus, 1762) (Diptera:Culicidae)
- Ultrastructural and enzymatic alterations in the ovary of Rhodnius prolixus infected with Trypanosoma rangeli