Effect of synoviectomy combined with postoperative radiotherapy on pigmented villonodular synovitis in knee: A meta-analysis
2022-04-07QiZhongLaiTianYeLinPengYangBingLangXiongQiZhaoZouKaiShenCaiZiQiLiWeiHeQingWenZhang
Qi-Zhong Lai, Tian-Ye Lin, Peng Yang, Bing-Lang Xiong, Qi-Zhao Zou, Kai-Shen Cai,Zi-Qi Li, Wei He, Qing-Wen Zhang✉
1. The First Clinical College of Guangzhou University of Chinese Medicine, Guangzhou 510080, China
2. The First Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou 510080, China
Keywords:Pigmented villonodular synovitis Knee Arthroscopy Open surgery Synovectomy Radiotherapy Metaanalysis
ABSTRACT Objective: Surgical resection of the diseased synovium is the main method for the treatment of pigmented villonodular synovitis in knee. Postoperative radiotherapy is an adjuvant therapy to reduce recurrence. However, whether it should be combined with radiotherapy is controversial. The study is designed to evaluate the efficacy of synovectomy combined with postoperative radiotherapy in the treatment of pigmented villonodular synovitis compared with only synovectomy in knee. Methods: The related references were searched from SinoMed, CNKI, Wanfang, VIP, PubMed, Embase, Cochrane Library and Web of Science from inception to October 2020, and the studies of synovectomy combined with postoperative radiotherapy were screened. According to the type of research, the corresponding evaluation methods were selected for quality evaluation of the literature. RevMan 5.3 software was used for meta-analysis. The primary outcome was recurrence, and the secondary outcome included complications, excellent and good rate of function of knee, range of motion of knee, Lysholm score and IKDC score of knee etcetera. Results: A total of 11 articles were included in meta-analysis, with 510 cases, 280 in the combined group and 230 in the control group. The results of meta-analysis showed that: (1) The recurrence rate in the combination group was significantly lower than that in the control group, OR=0.33 [95%CI (0.20,0.55)],p < 0.0001. (2) The complications in the combined group were higher than that in the control group, OR=2.70 [95%CI (1.16,6.31)], p=0.02. (3) The excellent and good rate of the combined group was significantly better than that of the control group, OR=2.86 [95%CI (1.23,6.64)],p=0.01, and it also may be the result of different evaluation criteria of each study. (4)There was no significant difference range of motion[MD=2.96,95%CI(-0.54,6.47),p=0.10],Lysholm score[MD=3.22,95%CI(-0.51,6.96),p=0.09] and IKDC score[MD=2.88,95%CI(-1.07,6.82),p=0.15] in knee between the two groups. Conclusions: The meta-analysis shows that synovectomy combined with radiotherapy can reduce the recurrence rate of pigmented villonodular synovitis in knee, but compared with only operation, there are higher complications. However, the above conclusions need to be verified by long-term follow-up of more high-quality clinical studies.
1. Introduction
Pigmented villonodular synovitis (PVNS) is a benign proliferative disease of synovium, synovial sac and tendon sheath, characterized by nodular hyperplasia of synovial villi and massive hemosiderin deposition[1]. The cause of the disease is not clear, there are trauma, tumor, inflammation and other theories, and the disease includes localized type and diffuse type[2, 3]. The age of onset of the disease is mostly 20-40 years old, mainly invading the large joints, the most common is the knee[4]. Surgery is the most common method for the treatment of the disease[5], including synovectomy (open or arthroscopic surgery), joint replacement, etc., but there is a risk of postoperative recurrence, especially the diffuse type[2].According to the literature[6], the average follow-up of 25 months in 214 cases of PVNS in knee, the postoperative recurrence rate of localized type was 8.6%, and that of diffuse type was 47.6%.Due to the high recurrence rate of PVNS, reoperation is needed after recurrence, and the operation may not completely relieve the pain, which brings emotional, psychological and economic burden to the patients, and seriously affects the quality of life of the patients[7, 8]. In recent years, adjuvant therapy has played a more and more important role in reducing recurrence rate and relieve pain, and postoperative combined radiotherapy is one of them[5].Some studies[9-11] reported that synovectomy combined with radiotherapy can reduce the recurrence rate and obtain good joint function. However, it has also been reported that the combination of radiotherapy after synovectomy can not reduce the recurrence rate[12], and even will have related complications and increased the risk of carcinogenesis[13-15].
There is no clear consensus on the treatment of PVNS in knee,and there are doubts about the combination of radiotherapy after synovectomy[1, 16]. Therefore, searching for the latest studies from domestic and overseas, we explore the efficacy of synovectomy combined with radiotherapy in the treatment of PVNS in knee.
2. Data and methods
2.1 Literature search
According to the combination of subject words and free words, four English databases of PubMed, Embase, Cochrane Library and Web of Science and four Chinese databases of SinoMed, CNKI, Wanfang and VIP were searched by computer. The retrieval period was from the time of building the database to October 2020. The Chinese key words were knee joint, pigmented villonodular synovitis,postoperative, radiotherapy, etc., while the English key words were knee, pigmented villonodular synovitis, synovectomy, radiotherapy,etc.
2.2 literature selection
2.2.1 Inclusion criteria
(1) types of study: randomized controlled trials, cohort studies,case-control studies; (2) subjects: patients diagnosed with PVNS in knee[3, 17]; (3) intervention: open or arthroscopic synovectomy was used in the combined group, adjuvant radiotherapy after operation,and only open or arthroscopic synovectomy was used in the control group. (4) outcomes: recurrence, complications, excellent and good rate of function of knee, range of motion of knee, Lysholm score and IKDC score of knee etcetera.
(1) descriptive research; (2) conference reports, case reports,experience introductions and reviews; (3) repeatedly published literature; (5) full-text literature that cannot be downloaded; (6)incomplete outcome data; (7) non-Chinese or non-English literature.
2.2.3 Outcomes
(1) main outcome: recurrence, (2) secondary outcomes:complications, excellent and good rate of function of knee, range of motion of knee, Lysholm score and IKDC score of knee etcetera.
2.3 Literature screening and data extraction
The retrieved literatures were removed the repetition and saved the remained, and then established a database by Note Express.According to the inclusion and exclusion criteria, two researchers independently read the titles and abstracts of the literature retrieved,and screened out the possible included literature. For the selected literature, read the full text carefully and marked the included literature. The two researchers cross-checked the included literature,and if there were differences in the included literature, the group discussed the solution and reached a consensus, which was taken as the final result standard. Two researchers used Microsoft Excel 2019 to extract the information from the included literature, including the first author, time of publication, type of study, number of cases,follow-up time, intervention, recurrence, complications, excellent and good rate of function of knee, range of motion of knee, Lysholm score and IKDC score of knee and other related information in the combined group and control group. After extracting the information,the two researchers checked it carefully, and finally saved the data.
2.4 Quality evaluation of the included literature
The quality evaluation of the included literature, cohort study or case-control study was evaluated according to the Newcastle-Ottawa scale (NOS) [18]. The scale has three columns, including:the study population chooses (selection), the comparable between groups(comparability), outcome, and its full score is 9. The randomized controlled trial was evaluated with the Jadad scale[19],which have three columns: random, blind, loss of follow-up and withdrawal, with a full score of 5.
2.5 Statistical analysis
RevMan 5.3 software was used for statistical analysis. The ratio ratio (OR) was used as the effect scale for the counting data,and the weighted mean difference (MD) or the standard mean difference (SMD) was used as the effect scale for the measurement data according to the similarities and differences of measurement methods. The heterogeneity test was evaluated by Q test and I test.When P > 0.1 and I2< 50%, heterogeneity was considered to be not statistically significant, and fixed effect model was used. When P <0.1 or I2> 50%, heterogeneity was considered to exist, and random effect model was used. When heterogeneity was high, found out the source of heterogeneity and then conducted sensitivity analysis or subgroup analysis. Funnel plot was used to analyze potential publication bias. The confidence interval was 95%, and statistically significant was p < 0.05.
3. Results
3.1 Process and results of literature retrieval
A total of 382 related references were obtained, including 219 in Chinese, 163 in English and 193 remained after removing repetitive literature. According to the inclusion and exclusion criteria, 11 references were included after reading the title, abstract and full text of the literature[12, 20-29]. There were 510 patients, including 280 patients in the combined group and 230 patients in the control group.The process and results of literature retrieval are shown in figure 1.
It is true that she never said so positively, but she certainly allowed the Princess to believe it, because she thought a little disappointment would be good for her
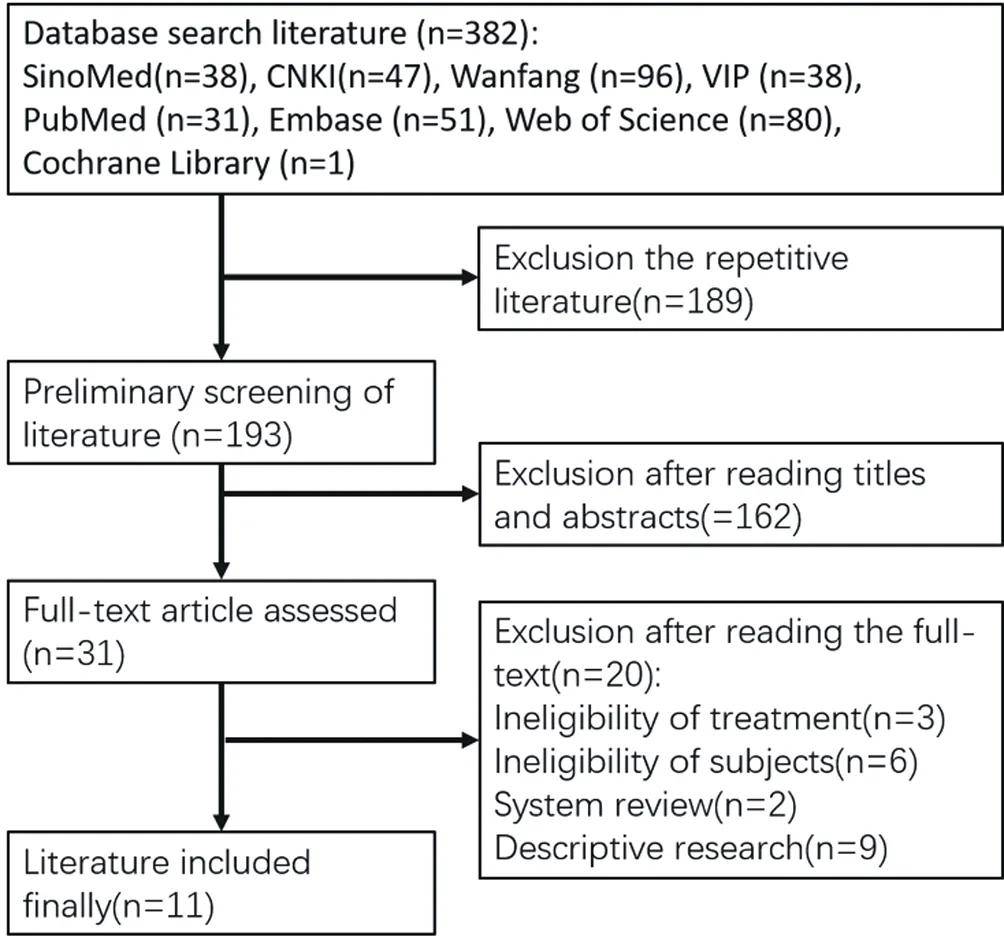
Figure 1 Flow chart of literature screening
3.2 Basic characteristics and quality evaluation of the included literature
The basic characteristics included of the included study are shown in Table 1-2. In the cohort study, the Newcastle-Ottawa scale was used to evaluate the quality of the literature, and the Jadad scale was used in the randomized controlled trial. 9 of the 10 cohort studies were scored ≥ 7, 1 was scored as 5, and 1 randomized controlled trial was scored as 2.
3.3 Results
3.3.1 RecurrenceAll the included literature[12, 20-29] reported the recurrence, and one[21] was divided into three subgroups according to the different lesions, so the three subgroups were analyzed independently to reduce the heterogeneity (marked as①②③respectively). There was no significant heterogeneity (P=0.54, I2=0%), and the fixed effect model was used for meta-analysis. The results showed that the recurrence rate of the combined group was significantly lower than that of the control group, OR=0.33 [95%CI (0.20,0.55)], and there was significant difference in the recurrence rate between the two groups (p < 0.0001). The quality of 2 articles[24, 28] was low, so metaanalysis was performed again after excluding these two references.The result showed OR=0.41 [95%CI (0.24,0.70)], and there was significant difference in recurrence rate between the two groups (p=0.001). According to the mode of radiotherapy, subgroup analysis was carried out. External radiotherapy, there are 7 articles[21-24, 26-28], there is no significant heterogeneity (P=0.97, I2=0%). The fixed effect model was used, and the result was OR=0.16 [95%CI (0.07,0.38), p<0.0001), indicating that the recurrence rate of combined external radiotherapy after synovectomy was significantly lower than that of only operation group. For in vivo radiotherapy, 3 references[12, 25, 29] were analyzed, OR=0.54 [95%CI (0.25, 1.14),p=0. 10. There was no significant difference in the recurrence rate between postoperative combined intrabody radiotherapy and simple operation. See figure 2-5.

Table 1 Basic characteristics of the included studies
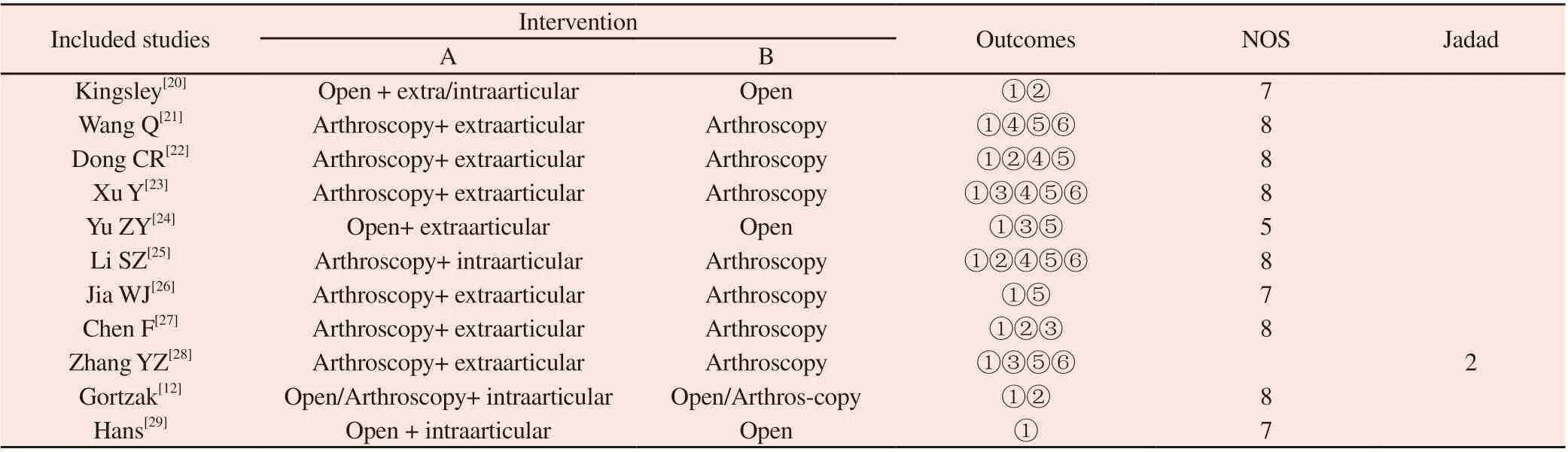
Table 2 Basic characteristics of the included studies
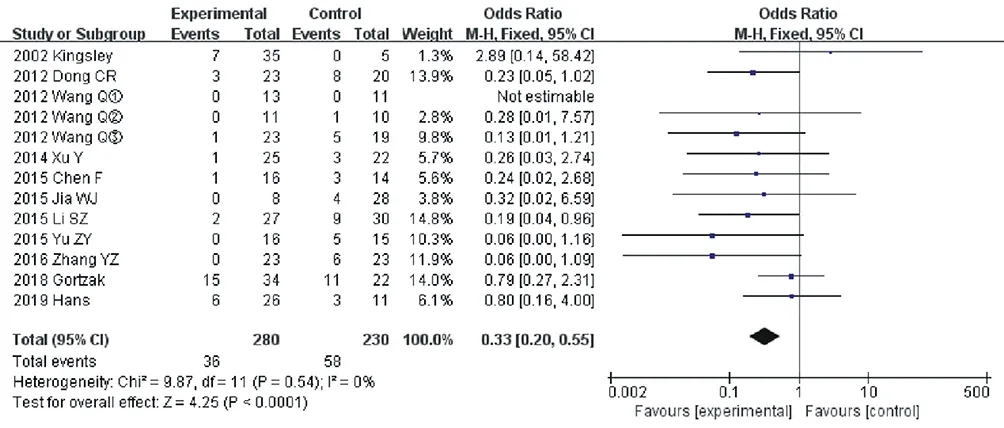
Figure 2 Forest diagram for comparison of postoperative recurrence rates between the two groups
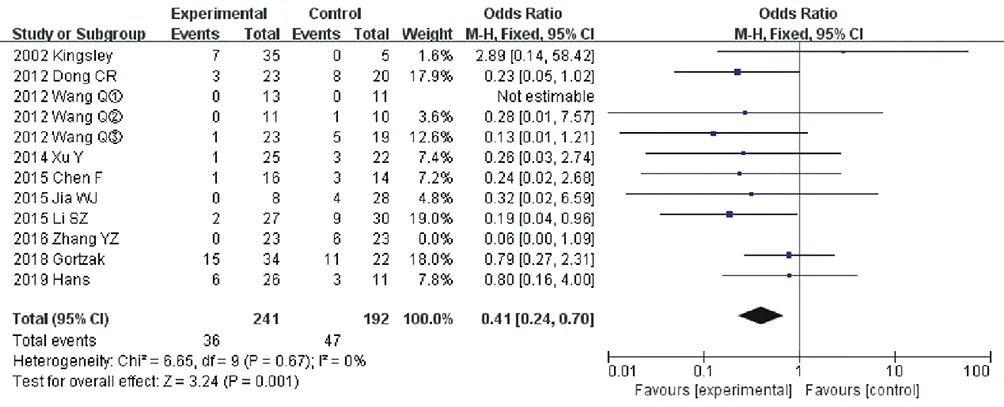
Figure 3 Forest diagram for comparison of postoperative recurrence rates between the two groups after the exclusion of the two references

Figure 4 Forest diagram for comparison of postoperative recurrence rates between the two groups of extraarticular radiotherapy

Figure 5 Forest diagram for comparison of postoperative recurrence rates between the two groups of intraarticular radiotherapy
3.3.2 Complications
Five articles[12, 20, 22, 25, 27] recorded the complications after treatment, and one of them[20] did not specify which group of complications, so 4 articles were analyzed by meta-analysis. The fixed effect model was used for meta-analysis (P=0.37, I2=4%). The results showed that there was a significant difference in the incidence of complications between the two groups, OR=2.70[95%CI(1.16,6.31)], p=0.02. See figure 6.

Figure 6 Forest diagram for comparison of postoperative complications between the two groups
3.3.3 Excellent and good rate
Four articles[23, 24, 27, 28] reported the excellent and good rate, of which one[24] only had data of the combined group, but no data of the control group. Therefore, 3 articles were analyzed. It is worth noting that the criteria for judging the excellent and good rate of the three articles are not the same. The fixed effect model was used for meta-analysis (P=0.72, I2=0%), and the result showed that there was a significant difference in the excellent and good rate between the two groups, OR=2.86[95%CI (1.23,6.64)], p=0.01. See figure 7.
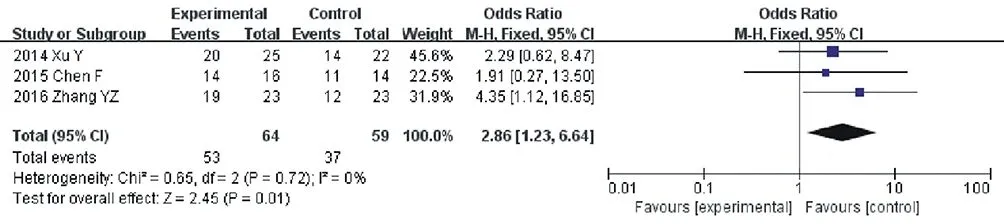
Figure 7 Forest diagram for comparison of the excellent and good rate postoperative between the two groups
3.3.4 Range of motion of kneeThere were 4 references[21-23, 25] that recorded the complete range of motion of the knee that could be used for analysis. Heterogeneity analysis showed that there was no significant heterogeneity between the two groups (P=0.21, I2=30%). The fixed effect model was used to analyze. There was no significant difference in the range of motion of the knee between the two groups (MD=2.96,95%CI (-0.54, 6.47), p=0.10. See figure 8.

Figure 8 Forest diagram for comparison of range of motion of knee postoperative between the two groups
3.3.5 Lysholm score of knee
Five studies[21-23, 25, 28] recorded complete knee Lysholm scores that can be used for analysis, and the included studies had heterogeneity (P<0.00001, I2=85%). The dates were analyzed by random effect model, and the results were MD=3.22,95%CI (-0.51,6.96), p=0.09, indicating that there was no significant difference Lysholm scores of between the two groups. See figure 9.

Figure 9 Forest diagram for comparison of Lysholm score postoperative between the two groups
3.3.6 IKDC score of knee
Four articles[21, 23, 25, 28] recorded the complete knee IKDC score for analysis. Heterogeneity analysis showed that the random effect model was used for meta-analysis, (P=0.0005, I2=78%). The results were MD=2.88,95%CI (- 1.07), p=0.15, indicating that there was no significant difference in knee IKDC score between the two groups.See figure 10.

Figure 10 Forest diagram for comparison of IKDC score postoperative between the two groups
3.4 Sensitivity analysis
High heterogeneity was found in Lysholm score and IKDC score of knee, and one reference[28] was found after eliminating one by one.After excluding the reference, the final conclusion did not change.The heterogeneity may come from the subjectivity of Lysholm score and IKDC score of knee. See figure 11-12.
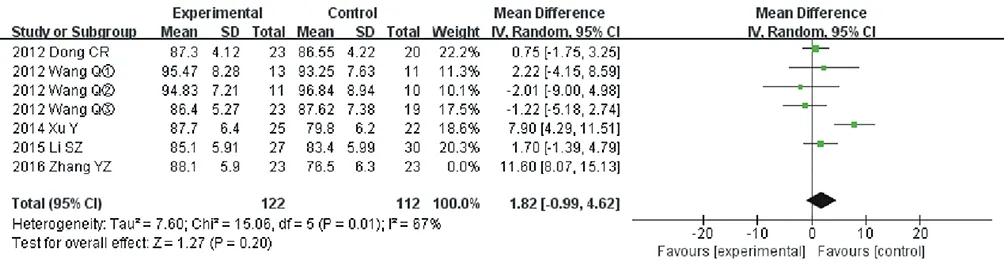
Figure 11 Sensitivity analysis of Lysholm score of knee

Figure 12 Sensitivity analysis of IKDC score of knee
3.5 Publication bias analysis
The recurrence of PVNS in knee treated by synovectomy combined with postoperative radiotherapy was analyzed by funnel plot. A total of 11 literature were included[12, 20-29]. As shown in figure 13,there was asymmetry in scatter points, suggesting publication bias,which may be caused by small sample size and unpublished negative results.
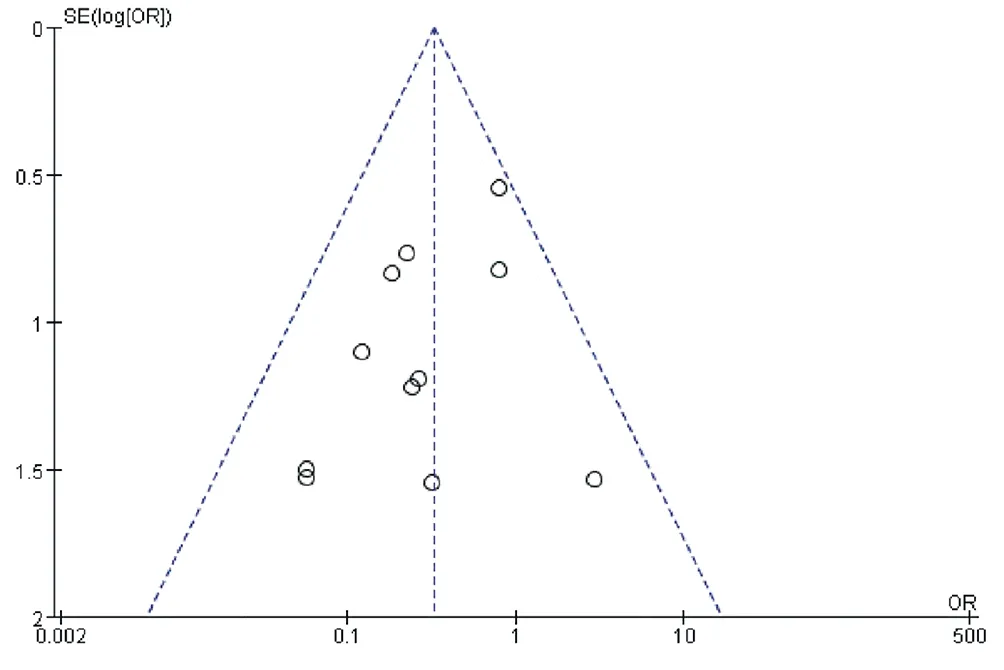
Figure13 Funnel plot of recurrence
4. Discussion
Synovial tissue of PVNS lesion of knee is invasive and can destroy bone. Early surgical resection of diseased synovial tissue is of great significance. At present, synovectomy mainly includes open surgery and arthroscopic surgery. No matter what kind of operation, there is the possibility of recurrence. The recurrence rate of PVNS in knee is related to the follow-up time[30]. The longer the follow-up time is,the greater the recurrence may be. The recurrence rate varies with different types of lesions. Palmerini et al[31] had did a retrospective analysis of 294 PVNS patients, 28% reported local recurrence, 14%in localized type, 36% in diffuse type (p=0.002). The median time of recurrence was 16 months, the average follow-up time was 4.4 years, and 66% had no recurrence in 5 years. Patel et al[6] reported that, with the average follow-up of 25 months (1.5-168 months) of 214 PVNS patients in knee, the recurrence rate of localized type was 8.6%, while that of diffuse type was 47.6%. For localized type,there is no significant difference in recurrence rate between open surgery and arthroscopic surgery[6], but arthroscopic surgery has fewer complications, so arthroscopic surgery is more recommended for localized PVNS. For the diffuse type, Gu et al[32] reported that multi-directional arthroscopic surgery is superior to open surgery in the recovery of function of knee and can shorten hospital stay and reduce the amount of bleeding. However, some studies[6, 33, 34]suggested open surgery for the treatment of diffuse PVNS in knee,which believed that diffuse type and arthroscopy are closely related to recurrence. The high recurrence rate of arthroscopic treatment of diffuse PVNS may be related to the fact that the range of exposure is too small to remove the lesion of synovial tissue thoroughly. For those cases, open surgical resection may be an ideal surgical method.In addition, some studies [35, 36] reported that arthroscopic surgery combined with open surgery for the treatment of PVNS of knee can get better. In the literature included in this study, 10 were diffuse lesions, 1 did not explain what kind of lesions, with a total of 510 patients, including 94 cases of recurrence.
For diffuse type, total synovectomy may be difficult to achieve[37],which is an important cause of postoperative recurrence, and postoperative radiotherapy plays an auxiliary role in resecting the residual small lesions[20]. Radiotherapy includes intra-articular and extra-articular radiotherapy, which can reduce the recurrence for patients with high risk of recurrence. Some studies[9-11] reported that combined radiotherapy after synovectomy can effectively reduce recurrence. Oztemur et al[38] reported that arthroscopic surgery or open surgery combined with radiotherapy is effective in the treatment of PVNS of knee, but there is no difference between the two methods. However, in the study of Gortzak et al[12], 56 patients with PVNS of knee were included, 34 patients in the combined group received intra-articular injection of yttrium-90 from 6 to 8 weeks after synovectomy, and 22 patients in the control group only underwent synovectomy. The average follow-up was 7.3 years (2.5-25.5 years). There were 15 cases of recurrence in the combined group and 11 cases in the control group (p<0.363). Postoperative combined with intra-articular radiotherapy did not reduce the recurrence rate. In this study, meta-analysis of 11 articles showed that postoperative combined radiotherapy was better than simple operation in controlling the recurrence rate, with an OR of 0.33[95%CI (0.20,0.55)], p<0.0001. The result is similar to an individual data meta-analysis in 2015[39]. However, most of the literature included in that meta-analysis were descriptive studies, and there was no control group, the research time was relatively long, and has not been included in the relevant domestic literature. When analyzed the different modes of radiotherapy, it indicates that the recurrence rate of combined external radiotherapy after synovectomy is significantly lower than that of simple operation group OR=0.16 [95%CI(0.07,0.38)], p<0.0001. For extra-articular radiotherapy, OR=0.54[95%CI (0.25,1.14)], p=0. 10, there was no significant difference.The results showed that it was feasible to reduce the recurrence rate by combined extraarticular radiotherapy, but no significant evidence was found in intra-articular radiotherapy. It is worth mentioning that there are 7 articles in the former and only 3 in the latter, which may also be the result of publication bias or too little literature. Some studies[40] have found that the preoperative neutrophil-lymphocyte ratio is a simple and economical predictor for recurrence of PVNS of knee after arthroscopic surgery combined with local radiotherapy,which is of far-reaching significance in guiding clinical work.
In terms of complications, postoperative combined radiotherapy was significantly higher than that of simple operation, OR=2.70[95%CI (1.16,6.31)], p=0.02. Radiotherapy can remove the residual lesions after surgery, but it is also a kind of injury to the tissue around the knee, so radiotherapy may be accompanied by complications[11, 13-15, 41], including short-term, such as joint swelling, transient myelosuppression, etc., as well as long-term,such as skin pigmentation, and what is more serious is bone ischemic necrosis and canceration. Based on this consideration,Stephan et al[1] did not recommend radiotherapy for the treatment of PVNS of knee. If postoperative combined radiotherapy is needed, it should be performed by an experienced doctor to reduce related complications[42]. In terms of excellent and good rate, the combination group is significantly better than the control group,which may be due to the different criteria for the evaluation of each study, leading to such a result. In terms of the function of knee, there was no significant difference in knee range of motion, Lysholm score and IKDC score between the two groups.
The limitations of this studies are as follows: (1) Only one randomized controlled trial is included, and the quality of the RCT is not high, and the rest are mainly cohort studies, and the conclusions are easily affected by the low level of evidence; (2) The total number of cases included in the study is limited, and the bias can not be eliminated thoroughly, and some outcome indicators are included in a small number of literatures. At the same time, there are few foreign studies that meet the included criteria, which will inevitably affect the conclusion. (3) The follow-up time of each study is different, so it can not judge the long-term effect well, and there is a high heterogeneity. (4) There are many specific ways of postoperative combined radiotherapy. Due to the limited number of literatures, the curative effect of each method can not be analyzed one by one. Combined analysis may lead to bias. Therefore, we should be cautious about the conclusions of the meta-analysis.Generally speaking, the quantity and quality of the studies included in this paper still need to be improved. Therefore, the conclusions of this paper need to be verified by more large-sample multicenter prospective clinical studies fully.
In conclusion, the meta-analysis of the included literature shows that, in the treatment of PVNS of knee, synovectomy combined with radiotherapy can reduce the recurrence rate, but compared with only surgery, there are higher complications. This conclusion requires more prospective, large sample, multicenter, randomized clinical trials to provide more reliable evidence.
The author's contribution to this article:
Lai Qizhong, first author, design executor, participated in literature screening, data analysis and first draft writing. Zhang Qingwen,corresponding author, design scheme and article content revision.The second author participated in the correction of the first draft.The third author gave support in terms of statistical software. The fourth author participated in literature retrieval and screening. The fifth author participated in literature review and data extraction. The sixth author participated in literature review and data extraction. The Seventh and eighth author, the article's revised and so on.
杂志排行

Journal of Hainan Medical College的其它文章
- Study on prescription and medication rules of Hua Baojin for treatment of colorectal cancer based on data mining
- Molecular mechanism of treatment of pneumonia in children with Mori cortex - Lycii cortex based on network pharmacology
- Analysis of risk factors and establishment of predictive model for elevated ALT in adult patients with nonalcoholic fatty liver disease
- Mechanism of Resveratrol on autophagy mediated by Mst1/Sirt3 signaling pathway in diabetic cardiomyopathy
- A systematic review and meta-analysis for platelet-rich plasma in treatment of knee osteoarthritis
- Identification and analysis of core target genes of miR-29b-3p in glioma