Ilizarov bone transport combined with the Masquelet technique for bone defects of various etiologies(preliminary results)
2022-04-06DmitryBorzunovSergeyKolchinDenisMokhovikovTatianaMalkova
INTRODUCTION
The challenges of long-bone defect management have increased in contemporary orthopedic practice due to the severity of high-energy trauma and its complications[1].These defects can lead to a multistage,long and costly treatment.The Ilizarov method of bone transport(IBT)and the Masquelet induced membrane technique(IMT)have been used in a great variety of challenging clinical situations including post-traumatic bone loss,infected nonunion,tumor resection,and congenital deficiency,such as congenital pseudarthrosis of the tibia(CPT)[2-4].Both techniques have specific merits and shortcomings,but numerous studies have shown their efficacy in the management of extensive longbone defects of various etiologies,including congenital defects[2-5].
The troll then showed him the three bushels of money which he had earned during the past year; they stood beside the other three, and all the six now belonged to him
The IBT has been praised for high union rates and its biological aspect of growing authentic bone tissue to close bone defects[5-7].Its followers believe that it is an ideal type of non-free bone grafting by which a vascularized autologous osteotomized bone fragment is transported gradually in the interfragmental gap within the soft tissue envelope to grow the missing bone part of a required length and shape[2,6-8].The Ilizarov system has been criticized due to complications such as pin-tract infection,pain,possible joint contractures,risk of ischemic regeneration in compromised soft-tissues around a large defect and impaired quality of life due to the long time needed to provide treatment tasks and new bone remodeling[9].The IMT is also based on the biological tissues of the induced membrane(IM)and autologous bone grafting,and utilizes internal or external fixation[10,11].It is not devoid of characteristic complications either,being a staged treatment that takes months to complete bone remodeling.However,it provides a better quality of life,especially if pathology is located in the upper limb and femur[3,10].
Recent available studies have reported mostly good final outcomes of both procedures[6,7,10,11].A study that compared the IBT(37 sources)and the IMT(41 sources)did not find statistical differences and reliable advantages between them in regard to consolidation,infection risks and failures that ended with amputation[12].However,the study found that IBT patients had a higher rate of refractures.This may be associated with the fact that bone regeneration in large defects requires a longer time for remodeling and needs supportive internal fixation[8].Nevertheless,several reviews and clinical studies doubt the superiority of IMT over IBT for long-bone defects in the lower extremity and point out that bone consolidation time may be unpredictable while non-weight bearing is prolonged in IMT[13,14].High rates of infection and even amputation were reported for tibial defects after open fractures treated with IMT[14].On the contrary,IBT allows weight-bearing from the first days.It is primarily used in patients with an infected tibia and rarely results in amputation[2,5].In pediatrics,IMT has been frequently used for cancer surgery reconstructions[4].Congenital anomalies,including СPT,may be treated with both options[4,15,16].
The combination of IMT and IBT may provide good outcomes in post-traumatic tibial defects after previous treatment failures,although the external fixation is longer due to spacer retention time.This combination might also be used for severe types of CPT despite possible refractures.
MATERIALS AND METHODS
We retrospectively studied the treatment course and outcomes in a case series that included seven PTD patients(subgroup A)and nine CPT cases(subgroup B)managed using the combination of IMT and IBT.The patients were treated at the same specialized department in our orthopedic center by one team of surgeons in 2014–2019.
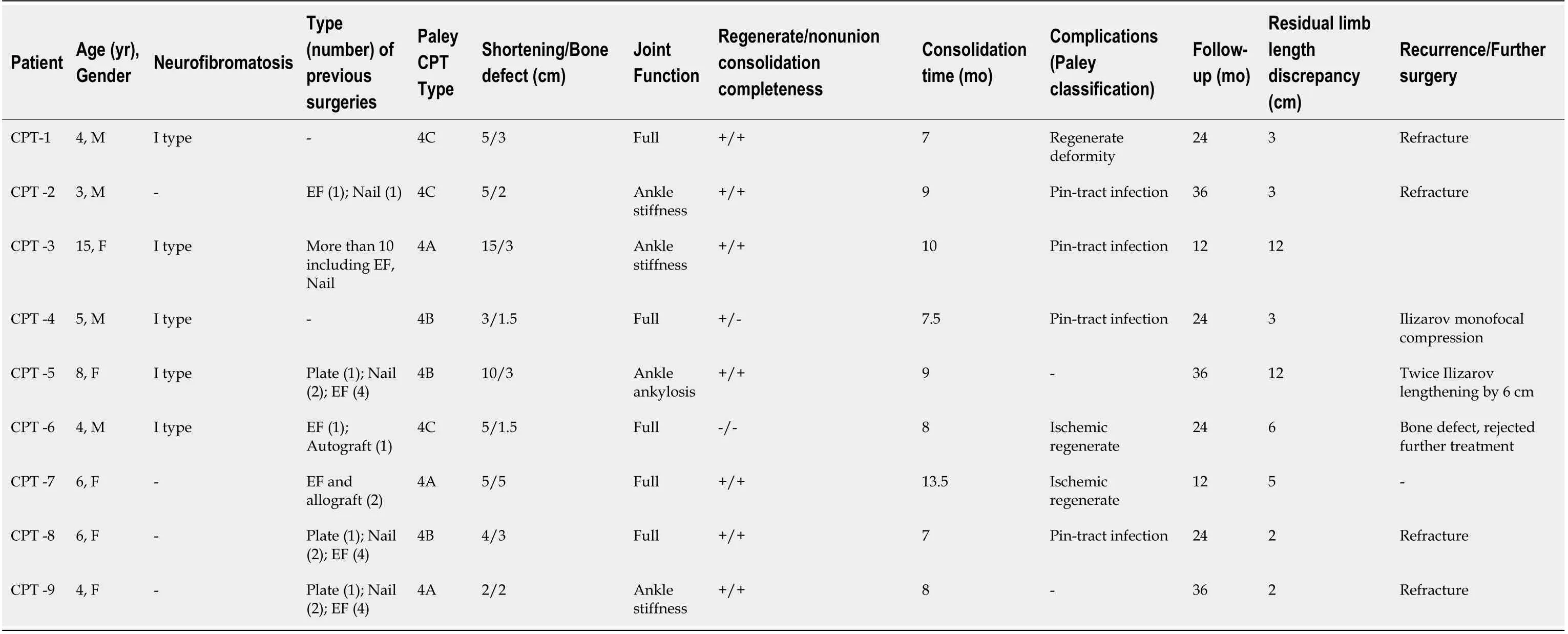
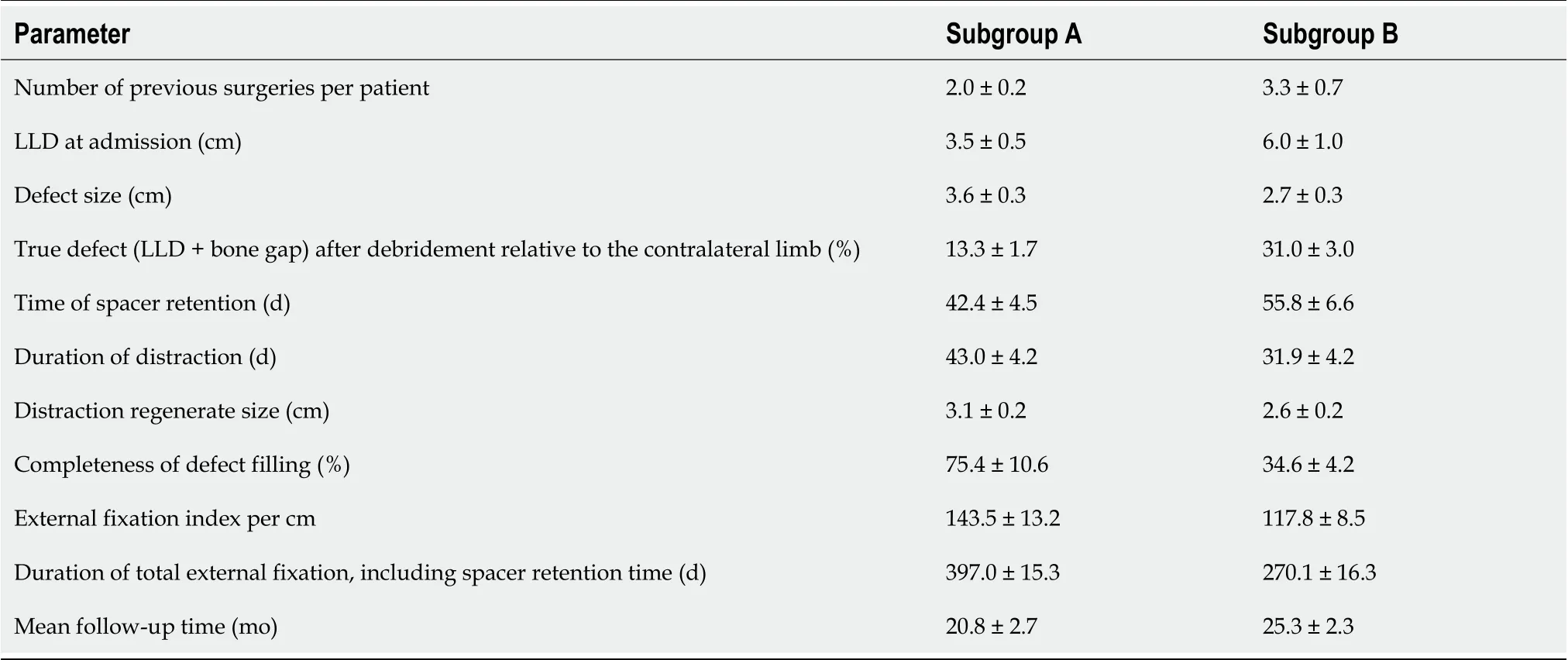
Tibial defects in subgroup A were caused by falls from a height,injuries at production sites and traffic accidents(Table 1).Time since injury was from one to 12 years(mean,3.7 ± 0.9 years)and all subjects were adults(six males and one female with a mean age of 38.5 ± 4.1 years).Six cases had a history of infection and one had delayed wound healing.Patients’ inclusion criteria in subgroup A were bone defects of post-traumatic origin after several failed previous treatments,with a disease history of one year or more,and non-viable types of nonunion(hypotrophic,torsion-wedge,defect-pseudarthrosis).Patients with active infection or hematogenous osteomyelitis were excluded.Subgroup B included nine children with a mean age of 6.1 ± 0.9 years and severe CPT types(Paley types 4 a-c)[15],mostly due to neurofibromatosis type I,who had had numerous failed interventions to unite pseudarthrosis and had no active infection(Table 2).Mean preoperative data of both subgroups are given in Table 3.
Osteotomy for bone fragment transport.The spacer was accessed through the previous incision.Careful handling was required to maximize preservation of the induced membrane.Upon removal of the spacer,the induced membrane that enveloped it remained in the interfragmental gap and the wound was sutured.In the frame being unchanged,a mainly proximal osteotomy for bone transport was performed.The distal fragment was osteotomized in PTD-case 5(Table 1);osteotomy wasperformed at two levels in CPT-case 7(Table 2).Distraction was initiated from day 5 to 7 at a rate of 1 mm/d produced with 4 increments.Condition of the regeneration was checked radiographically every ten days.In low optical density of the regenerate or its deformity,the rate of distraction was adjusted or reduced to 2 or 3 increments,a quarter of a mm each.The transported bone fragment ran in the membrane without technical problems.Distraction was carried out until close docking of the fragments.Upon docking,supportive compression of 1 mm was provided once every two weeks in the consolidation phase.Autologous grafting was not added.
Surgical protocol
Ilizarov frame mounting + spacer implantation.The Ilizarov frame was constructed of three ring supports with three wires in the proximal and distal rings and two wires in the middle ring at the level of the tibial diaphysis.Fibular osteotomy was performed in order to eliminate segment deformities.For pseudarthrosis resection,an anterior approach to the tibia was used.In subgroup A,the resection started from the level of the endplate and extended to the margin with the bleeding bone.The "blood dew" sign indicated an adequate level of resection.In subgroup B,the pseudarthrosis zone along with the surrounding pathologically altered periosteum was resected.After resection,the limb was fixed with the Ilizarov frame in a neutral position according to the tension of soft tissues with the correct anatomical axis of the segment.Next,the defect size was measured.A pre-shaped spacer was prepared from methyl methacrylate cement by molding in a syringe.Its diameter corresponded to the bone diameter of the specific patient,coinciding with the level of the cortical plates,or going beyond the cortices by 2-3 mm.The spacer was placed into the defect gap after being hardened and was fixed in the gap by applying compression with the Ilizarov frame.One dose of vancomycin was added to the spacer material for infection prevention in subgroup A.Wounds were closed in the regular manner.We used only the first phase of the IMT procedure.
There he sat, lighted up by the flames from the burning house opposite, both hands holding tightly12 on his red cap, in which lay the treasure; and now he knew what his heart really valued most--to whom he really belonged
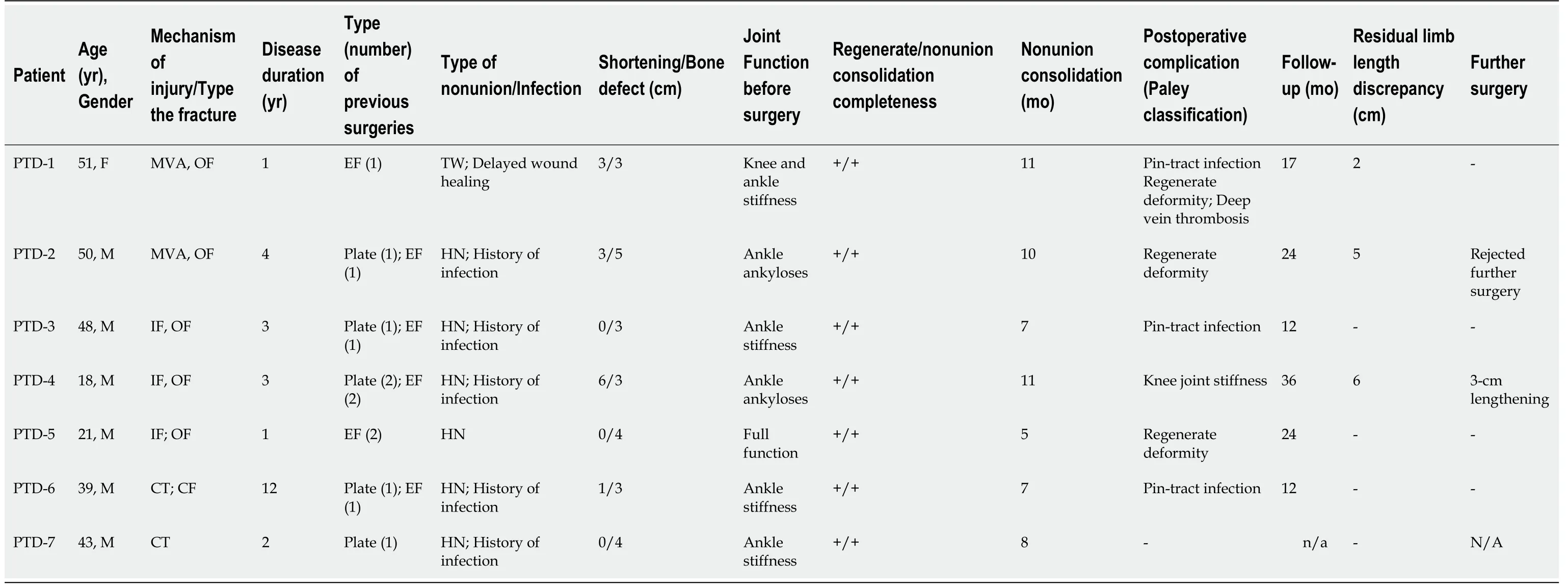
Postoperative care and radiographic checks followed the standards of the Ilizarov method.Radiographic evidence of bony union,external fixation time,defect filling rate and complications were assessed.The primary outcome measure was radiographic bone union.Secondary outcomes were correction of limb length discrepancy and deformities.
Thin fragments of the biomembrane formed around the cement spacer were harvested prior to bone transport for histological examination in all patients.The material was collected intraoperatively at step 2.
We also promoted osteogenesis at bone fragments docking.As the role of the periosteum in CPT pathogenesis has already been proven,we expected that the neoperiosteum-like nature of the induced membrane would have an effect on bone union and regeneration in the CPT subgroup.The induced membrane was supposed to supply blood to the area with a new vascular network,thereby excluding osteolysis.However,the results in subgroup B were similar to other current techniques used for this pathology[15].
All adult patients and the children’s parents gave informed consent for surgical treatment and inclusion in the study.The study was approved by the ethics board of our institution.
The subgroups had different etiologies of the defects and belonged to different age groups.Thus,we did not aim to compare them.The statistical method included calculation of mean values and their deviations using Microsoft Excel 2019.Moreover,the sample size of subgroups was small;therefore,only descriptive statistics were used.
RESULTS
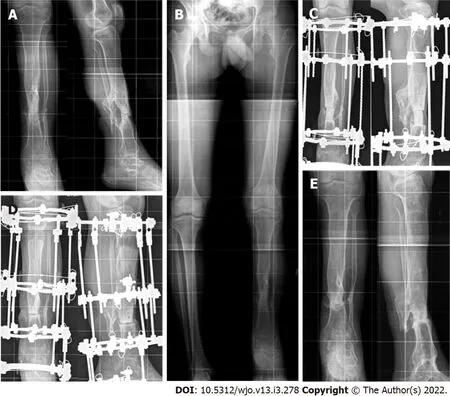
Table 1 and Table 2 present the main preoperative and treatment parameters along with outcomes of the combined technique of IMT + IBT in all patients.The mean values of the main measures are shown in Table 3.Bone union was achieved in all patients of subgroup A(Figure 1)and in seven patients of subgroup B(Figure 2).Total duration of external fixation was 397.0 ± 15.3 and 270.1 ± 16.3 d,including spacer retention time of 42.4 ± 4.5 and 55.8 ± 6.6 d,in subgroups A and B,respectively.One non-united CPT case was further treated with the Ilizarov compression method only and achieved union.Another failed CPT case was lost.After a follow-up period of one to three years,there were no refractures in subgroup A.Refractures occurred in four cases of CPT due to severe disease(mostly Paley CPT type 4 C)and multiple previous treatments.Cases CPT-8 and CPT-9 had seven previous surgeries each.

Bone transport in the membrane ran smoothly.Postoperative complications included several cases of pin-tract infection and regenerate deformity in both subgroups.Insufficient ischemic regeneration was observed in two cases of subgroup B.Bone regenerate deformity and pin-tract infection were resolved during the course of treatment.The regenerate zone was perforated with wires and supportive compression was performed with the same frame in ischemic hourglass-shaped regeneration for its stimulation.We prefer delayed lengthening to finally correct the length in non-viable nonunion,after bone consolidation has been secured.Thus,we subsequently performed this in two patients of subgroup A who applied for length compensation.Further treatment reduced limb length discrepancy from 12 to 6 cm in CPT-case 5 with two procedures.
We aimed to conduct clinical studies on the use of a new technological solution that integrates the IMT and IBT techniques for treating non-viable tibial defects of post-traumatic(PTD)etiology and CPT to improve bone regeneration at the docking site,bone consolidation and reduce refracture rate.
DISCUSSION
Several surgeries are often required to manage extensive segmental bone loss after multiple failures or severe congenital deficiency.They may result in prolonged recovery times,poor outcomes,and even amputation as a complex of mechanical issues and biological factors should be utilized for reconstruction[1,2].IBT has established itself as an efficient tool for long bone defect management,including patients with infections,especially in the tibia[5-9].It is able to resolve the problematic triad of bone loss,soft-tissue compromise and bone infection.The IMT has recently been used for extensive defects in any long-bone segment[3,4,18].According to several authors,the advantage of IMT over IBT lies in the fact that the consolidation time does not depend on the bone defect size as it is filled with autologous graft material[3,11].Nevertheless,extensive defects need a lot of bone graft substance,especially in the lower extremities[18].Alternately,the distraction procedure,being a part of IBT,is able to supply new regenerated bone substance[2].
We assumed that defect filling would provide a particularly favorable environment for bone regeneration and the reparative process with the combined use of IMT and IBT.After extraction of a spacer there is a tunnel in the interfragmental gap the walls of which are formed by the induced membrane which was found to be a type of neoperiosteum[16,19].Apart from a favorable mechanical effect,the combined conditions could provide a biological effect of the induced membrane on osteogenesis.It was shown that multiple microvessels of the biomembrane penetrate into the regenerate zone and promote the inflow of low differentiated pluripotent cells[16].The cells of the membrane basal layer and perivascular osteopontin-positive cells that possess osteogenic differentiation ability contribute to the formation of a low mineralized bone matrix on the surface of the spacer.This could cause an osteoinductive effect on the pluripotent cells in the region of the compression regenerate formed at the docking site.According to the reported findings,the osteoinductive membrane is adequately vascularized and produces growth factors(vascular endothelial growth factor,transforming growth factor-beta 1)and bone morphogenetic protein-2 that play a role in regeneration and may prevent lysis[19].It is also assumed that the biomembrane features antimicrobial activity related to the synthesis of antioxidants which are secreted locally along with growth factors[20].Another mechanism of the supposed bacteriostatic effect is the presence of local peptides in the membrane which are able to inhibit secretion of the bacterial biofilm[16].There were no foci of infection in the biomembrane fragments harvested at step 2 of our procedure in all cases.In addition,none of the patients developed infection.
But the host went around as if he didn t notice anything, though Grandfather always insisted that he detected a little twinkle in the rich man s eyes as he shook hands with all his fellow parishioners and wished them good night.
The results of the subgroups in our series could not be compared due to different etiologies and the pathogenesis of nonunion.For this reason,the outcomes were presented separately.Despite the absence of active infection,we chose the primary task to achieve radical debridement in order to prevent possible infection.In subgroup A,the spacer’s role was also to sanitize the site of previous infection.The absence of infection recurrence is attributed equally to the impact of radical debridement and that of the vascularized membrane.The interval between the first operation and the osteotomy was a period of infection control that was based on the results of bacteriological tests for selection of antibiotic therapy.The spacer maintained the shape of the defect gap to exclude soft tissues invagination into the defect.
The next day when I came to work Harry was behind the counter of Tony s magazine stand. He looked at me rather sheepishly and said, Well, I had to get a job somewhere, didn t I?
When they were wandering in this manner through the forest the hare carelessly raised his hatchet in passing, and cut down some thick boughs28 that were hanging over the path, but at length, after cutting down a good big tree, which cost him many hard blows, he declared that it was too heavy for him to carry home, and he must just leave it where it was
She stole into the garden, took a flower from the flower-beds of each of her sisters, kissed her hand a thousand times towards the palace, and then rose up through the dark blue waters
The removal of the spacer presupposes repeated trauma to the skin and soft tissues in the pseudarthrosis zone.However,if we draw a parallel,classical bone transport involves an open coaptation for fragments docking.According to the protocol for our combined technique,docking was performed in a closed way by compression at the junction of the fragments without grafting.The known approach to create the maximum "bone mass" in the area of pseudoarthrosis was implemented by the technique[15].Therefore,to add autologous bone grafting or internal fixation to the described combination seemed to us extremely invasive.However,open docking and a graft were used in an earlier study of infected tibial defects treated with a similar technology[21].Thus,there could be options to synergistically widen the integrated approach.
The nurse went, and was struck with amazement at the sun-like radiance of his face; she salaamed and said: O youth! welcome! the lady of the garden calls you; come! He went with her and into a palace which was like a house in Paradise, and saw seated on the royal carpets of the throne a girl whose brilliance93 shamed the shining sun
Consolidation of nonunion was achieved in all the defects of post-traumatic etiology but it should be noted that the IM effect was not strong enough for CPT consolidation and did not help to eliminate refractures in the long term.The refracture rate was comparable with the literature data on the use of other methods,including the Ilizarov method used separately[15].
The management of СPT has been much discussed recently and there is plenty of clinical research with variable results[15,22-30].The superiority of one of the techniques for reconstruction in CPT has not yet been confirmed.The latest clinical studies predominantly describe patients where the Ilizarov method is the main component of CPT management in conjunction with intramedullary nailing and bone grafting[22-25].The combined technique of the Ilizarov external fixation,stabilization with an intramedullary rod and corticocancellous bone autograft yields a statistically significant reduction in the number of refractures compared with standalone fixation methods.It was stated that the four methods of CPT treatment might achieve primary union of about 50% without refracture and this was attributed to the biological nature of CPT[15].Improved union rates in IMT assisted by the Ilizarov external fixator and grafting for previously failed CPT treatment were reported[26].
However,regardless of the primary bone fusion rates,most of the authors state that the probability of long-term bone union retention remains unpredictable due to biological factors of the disease characterized by low osteogenic potential.Therefore,methods to enhance this potential have been identified such as wrapping,grafting,crossunion of the tibia and fibula,and application of several biological agents to promote osteogenesis[27-30].Our technology might also be used.
The combination of technologies to treat orthopedic pathology is largely associated with the need to obtain a faster and a more efficient result in the most severe cases.Apart from our previous study[16],we found only three case reports that used the combined principles of IMT and IBT with satisfactory outcomes,although not quite the same as our technology[21,31,32].The limitation of our series is the small sample of patients with two different etiologies of defects and various clinical situations,but all severe cases.Our preliminary results suggest that the etiological factor plays a significant role in the use of this combined technique.Both subgroups had impaired bone regeneration potential due to multiple previous failures and a worsened condition of the tibia,but undoubtedly this was greater in subgroup B.
We retrospectively studied the treatment course and outcomes in a case series that included seven PTD patients(subgroup A)and nine CPT cases(subgroup B)managed by the combined technology of IMT and IBT.Adult patients in subgroup A had bone defects of post-traumatic origin after several previous treatments failed and non-viable types of nonunion(hypotrophic,torsion-wedge,defectpseudarthrosis).Subgroup B included nine children with a mean age of 6.1 ± 0.9 years with severe CPT types who had numerous failed interventions to unite pseudarthrosis.Step 1 included Ilizarov frame placement and spacer introduction into the resected defect to generate the induced membrane which remained in the interfragmental gap after spacer removal.Step 2 was an osteotomy and bone transport of the fragment through the tunnel in the induced membrane,its compression and closed docking for consolidation without grafting.Upon docking,supportive compression of 1 mm was provided once every two weeks in the consolidation phase.Postoperative care and radiographic checks followed the standards of the Ilizarov method.Radiographic evidence of bony union,external fixation time,defect filling rate and complications were assessed.The primary outcome measure was radiographic bone union.Secondary outcomes were correction of limb length discrepancy and deformities.The outcomes were retrospectively studied after a mean follow-up period of 20.8 ± 2.7 mo in subgroup A and 25.3 ± 2.3 mo in subgroup B.
CONCLUSION
The importance of improving bone regeneration in the management of large bone defects and CPT is a very relevant issue due to treatment failures that diminish bone potential for regeneration.Management of CPT may take years in a growing child due to frequent recurrences and has a negative impact on the child’s development.Therefore,a combination of the biological merits of IBT and IMT seemed to us a promising strategy in the management of cases with a history of failed attempts and impaired regeneration potential.Following use of the combined technique in an experimental canine model[17],we aimed to conduct clinical studies on the use of this new technological solution that integrates the IMT and IBT techniques for treating non-viable tibial defects of post-traumatic(PTD)etiology and CPT to improve bone regeneration at the docking site,bone consolidation and reduce the refracture rate.
ARTICLE HIGHLIGHTS
Research background
The challenges of long-bone defect management have increased in contemporary orthopedic practice due to the severity of high-energy trauma and its complications.They lead to a multi-stage,long and costly treatment.The Ilizarov method of bone transport(IBT)and the Masquelet induced membrane technique(IMT)have been used in a great variety of challenging clinical situations including posttraumatic bone loss,infected nonunion,tumor resection,and congenital pseudarthrosis of the tibia(CPT).
Research motivation
The importance of improving bone regeneration in the management of large bone defects and CPT is a very relevant issue due to treatment failures that diminish bone potential for regeneration.Therefore,a combination of the biological merits of IBT and IMT seemed a promising strategy for the management of cases with a history of failed attempts and impaired regeneration potential.
It is also important to note that since their earthly father has abandoned them, the Grimms have the children turn to God the Father to save them (Zipes 1997). Return to place in story.
Research objectives
Subgroup A patients could walk with crutches after frame removal gradually increasing weightbearing.Subgroup B patients were recommended to use crutches for one month and then leg braces for one year.
Research methods
We did not complete limb length compensation in our patients due to the severity of their tibial defects and pseudarthrosis.The primary goal was bone union.Of course,residual limb length discrepancy is the factor affecting the final result in post-traumatic cases.We recommend IBT for defects less than 12 cm,and free vascularized fibula or transverse Ilizarov transport of the fibular fragment for bigger defects[2].Due to the fact that IBT is able to realize the potential of human bone regeneration for anatomical and functional restoration in large long-bone defects with minimal trauma,it is extensively used after the failure of other established methods of treatment or infection.The arguments against it as a primary treatment option are the complexity of the Ilizarov apparatus mounting and its size,the number of adjustments,pin-tract infection,multi-stage and long treatment course that needs a lot of compliance both from the patient and the surgeon.Although IMT seems simple,it is not so easy to complete successfully in severe cases[33].Finally,it is worth noting the significant disadvantage of the combined approach which is an increase in the duration of total external fixation[21].Due to these facts,the integration is a more complex procedure.Its effects,modification or failures should be studied further.
Research results
Upon completion of treatment,defects were filled by 75.4 ± 10.6% and 34.6 ± 4.2%,in subgroups A and B,respectively.Total duration of external fixation was 397 ± 9.2 and 270.1 ± 16.3 d,including spacer retention time of 42.4 ± 4.5 and 55.8 ± 6.6 d,respectively.Bone infection was not observed.Postoperative complications included several cases of pin-tract infection and regenerate deformity in both subgroups.Ischemic regeneration was observed in two cases of subgroup B.Complications were corrected during the course of treatment.Bone union was achieved in all patients of subgroup A and in seven patients of subgroup B.One non-united CPT case was further treated with the Ilizarov compression method only and achieved union.After a follow-up period of two to three years,refractures occurred in four cases of united CPT.
Research conclusions
The combination of IMT and IBT may provide good outcomes in post-traumatic tibial defects after previous treatment failures,although the external fixation is longer due to spacer retention time.This combination might also be used for severe types of CPT,despite the fact that refractures may occur.
Research perspectives
There are ways to further investigate the adjuncts to our protocol such as grafting at the docking site and intramedullary nailing,especially in severe CPT.
I ve been in love with you for years, she said, since the first time I saw you from the Addisons living room window. Yes-it was me they wanted you to meet. But you wouldn t let anyone introduce us. You wouldn t let the Addisons set us up; you wouldn t take Karen s word for it that we would like each other. I thought I was never going to meet you.
FOOTNOTES
All authors contributed to the conception and design,drafting of the manuscript,analysis and interpretation of data,and critical revision of the manuscript;Malkova TA and Kolchin SN contributed to the acquisition of literature data;Kolchin SN performed statistical analysis.Borzunov DY,Kolchin SN,Mokhovikov DS performed the interventions in the cases included into this study.
The study was approved by the ethical committee at the Ilizarov Center.
All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
The authors have no conflict of interests.
No additional data are available.
As the train pulled away, I sat down on a bench in the station. What I had wanted to do with muscle had been accomplished32 with kind words. I had just seen Aikido in action, and the essence of it was love. I would have to practice the art with an entirely33 different approach and speak about the resolutions of conflict.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Russia
Dmitry Y Borzunov 0000-0003-3720-5467;Sergey N Kolchin 0000-0003-1606-4749;Denis S Mokhovikov
0000 -0001-8728-8948;Tatiana A Malkova 0000-0002-4301-9161.
Afterwards the teacher decided to do a class project to see what kind of impact recognition would have on a community. She gave each of the students three I more ribbons and instructed them to go out and spread this acknowledgment ceremony. Then they were to follow up on the results, see who honored whom and report back to the class in about a week.
Wang JL
Webster J
Marshmallows, I said, as though I d said it every summer. Last night Daddy and I walked down toward the lake and it looks as though they re just about ready to pick. It s a good thing we re here now. They only come out one day a year.
Wang JL
杂志排行
World Journal of Orthopedics的其它文章
- Impact of enhanced recovery pathways on safety and efficacy of hip and knee arthroplasty:A systematic review and meta-analysis
- Surgical treatment of femoral deformities in polyostotic fibrous dysplasia and McCune-Albright syndrome:A literature review
- Plate vs reverse shoulder arthroplasty for proximal humeral fractures:The psychological health influence the choice of device?
- Diagnostic role of Xpert-MTB RIF assay in osteoarticular tuberculosis:A retrospective study
- Comparative study of intertrochanteric fracture fixation using proximal femoral nail with and without distal interlocking screws
- Accuracy of shoulder joint injections with ultrasound guidance:Confirmed by magnetic resonance arthrography