Assessment of fibroblast growth factor 19 as a non-invasive serum marker for hepatocellular carcinoma
2022-04-02GhadaAbdelrahmanMohamedEhabHasanNashaatHadeerMohamedFawzyAhmedMohamedElGhandour
Ghada Abdelrahman Mohamed,Ehab Hasan Nashaat,Hadeer Mohamed Fawzy,Ahmed Mohamed ElGhandour
Ghada Abdelrahman Mohamed,Ehab Hasan Nashaat,Hadeer Mohamed Fawzy,Ahmed Mohamed ElGhandour,Department of Internal Medicine,Gastroenterology and Hepatology Unit,Faculty of Medicine,Ain Shams University,Cairo 11591,Egypt
Abstract BACKGROUND Fibroblast growth factor 19(FGF-19)is one of the founding members of the endocrine FGF subfamily.Recently,it has been the subject of much interest owing to its role in various physiological processes affecting glucose and lipid metabolism and the regulation of bile acid secretion as well as cell proliferation,differentiation,and motility.Additionally,FGF-19 secretion in an autocrine style has reportedly contributed to cancer progression in various types of malignancies including hepatocellular carcinoma(HCC).AIM To estimate the serum FGF-19 concentrations in HCC cases and assess its diagnostic performance for the detection of HCC.METHODS We recruited 90 adult participants and divided them into three equal groups:Healthy controls,cirrhosis patients,and HCC patients.Serum FGF-19 concentrations were measured using the Human FGF-19 ELISA kit.RESULTS We detected a high statistically significant difference in serum FGF-19 levels among the three groups.The highest level was observed in the HCC group,followed by the cirrhosis and control groups(236.44 ± 40.94 vs 125.63 ± 31.54 vs 69.60 ± 20.90 pg/mL,respectively,P ≤ 0.001).FGF-19 was positively correlated with alpha fetoprotein(AFP;r =0.383,P =0.003)and international normalised ratio(r =0.357,P =0.005),while it was negatively correlated with albumin(r =-0.500,P ≤ 0.001).For the detection of HCC,receiver operating characteristic curve analysis showed that the best cut-off point of AFP was > 8.2 ng/mL with an area under the curve(AUC)of 0.78,sensitivity of 63.33%,specificity of 83.33%,positive predictive value(PPV)of 79.2%,negative predictive value(NPV)of 69.4%,and total accuracy of 78%.However,FGF-19 at a cut-off point > 180 pg/mL had an AUC of 0.98,sensitivity of 100%,specificity of 90.0%,PPV of 90.0%,NPV of 100%,and total accuracy of 98%.CONCLUSION FGF-19 represents a possible novel non-invasive marker for HCC.It may improve the prognosis of HCC patients due to its utility in several aspects of HCC detection and management.
Key Words:Fibroblast growth factor 19;FGF-19;Fibroblast growth factors;Tumour biomarkers;Hepatocellular carcinoma;Detection;Cirrhosis
lNTRODUCTlON
Fibroblast growth factor 19(FGF-19)is one of the founding members of the endocrine FGF subfamily[1].Recently,it has been the subject of much interest owing to its role in various physiological processes affecting glucose and lipid metabolism and bile acid secretion as well as cell proliferation,differentiation,and motility[2-4].Additionally,FGF-19 secretion in an autocrine style has reportedly contributed to cancer progression in various types of malignancies including hepatocellular carcinoma(HCC)[5-9].
FGF-19 has a restricted pattern of expression.It is mostly expressed in the terminal ileum in response to the bile-acid-stimulated intestinal Farnesoid X receptor(FXR)[10],and then,through the portal circulation to the liver,it attaches to its receptor,fibroblast growth factor receptor 4(FGFR4),and a cofactor known as β-klotho.This action initiates the transcription of various genes that negatively regulate bile acid synthesis through the downregulation of CYP7A1[11].
Although FGF-19 is formed principally in the ileum and FGF-19 expression is almost absent in the human liver under normal conditions,current studies propose that FGF-19 may be autocrined by human hepatocytes under cholestatic conditions,peritumoral tissue cirrhosis,and HCC.The secretion of FGF-19 in these conditions demonstrates the protective negative feedback of FGF-19 in order to guard hepatocytes from the cytotoxicity of bile acids[12-14]and the promotion of the development and progression of HCC by bile acids through mTOR dependent mechanisms[15].This beneficial effect of the FGF-19 pathway has also been proposed in other studies inFXR-/-knock out mice that developed hepatic malignancies,which were inhibited by the expression of anFXRtransgene in the intestine[16].This effect indicates the protective aspect of Fgf15(the mouse homolog of human FGF-19)in relation to hepatic malignancies.Additionally,Fgf15/FGF19 mediated hepatic regeneration in mice in other studies[17,18].
However,the higher expression of FGF-19 in HCC patients has been found to promote tumour cell survival and has antiapoptotic impacts that are applied through the FGFR4-glycogen synthase kinase(GSK)3β-Nrf2 signalling pathway[19].Moreover,Kanget al[20]showed that a distinctive molecular subtype of FGF-19 is correlated with a poor prognosis in HCC patients.In addition,Cuiet al[21]and Zhaoet al[22]reported that Fgf15 and FGF-19,respectively,promoted the progression of HCC by stimulating epithelial-mesenchymal transition and Wnt/β-catenin cascade,which is linked to tumour aggression and mortality.Furthermore,previous data has pointed to FGF-19 as a promoter of liver stem cells in HCC patients,as noted in the robust association between FGF-19 and EpCAM,which is a moderator of cell adhesion and signalling and a special biomarker for liver cancer stem cells[23,24].Additionally,confirmation of the role of FGF-19 signalling in HCC progression arises from the tumourpreventing effect of the selective FGFR4 inhibitor BLU9931 in a mouse HCC model with implanted FGF-19-producing,FGFR4-expressing hepatic cells[25].These results suggest that FGF-19 may be implicated in tumour development in HCC cases.
Since FGF-19 is a serum protein secreted by HCC cells in an autocrine loop style,and systemic concentrations of FGF-19 have been found to reflect its portal concentrations[14,26],we aimed to estimate the serum FGF-19 concentrations in HCC cases and assess the diagnostic performance of FGF-19 for the detection of HCC.
MATERlALS AND METHODS
This observational study was conducted at Ain Shams University Hospitals in Cairo,Egypt from March 2021 to September 2021.This study was performed in accordance with the ethics principles of the Declaration of Helsinki and was authorised by the ethics board of the Faculty of Medicine,Ain Shams University(No.FMASU MS 66/2021).Written informed approval was obtained from all the participants before they were enrolled in the study.
We consecutively recruited 90 adult participants and divided them into three equal groups:Healthy controls,cirrhosis patients,and HCC patients.Patients with any malignant disease other than HCC were excluded.None of the HCC cases had either neoadjuvant chemotherapy or radiotherapy.
Diagnosis of cirrhosis and HCC
Cirrhosis was diagnosed according to laboratory parameters,clinical manifestations,and/or histological criteria[27].HCC was identified through contrast-enhanced imaging studies and/or histological criteria as per the practice guidelines[28].
Measurement of serum FGF-19 concentrations
The serum FGF-19 concentrations were measured using the Human FGF-19 ELISA kit(SunRed Biological Technology Co.Ltd.,Shanghai,China,Catalogue # 201-12-2199)with a sensitivity of 2.032 pg/mL,assay range of 2.5-700 pg/mL,intra-assay coefficient of variability(CV)< 10%,and inter-assay CV < 12%.
Statistical methods
Data were analysed using the Statistical Package for Social Science(IBM SPSS Statistics for Windows,Version 20.0.Armonk,NY:IBM Corp).The qualitative variables are shown as numbers and percentages,while the quantitative variables are shown as the mean,standard deviation,or median and interquartile range,as appropriate.The differences among the groups were calculated using the Chisquare test,Fisher exact test,independentt-test,one-way ANOVA test,or Kruskal-Wallis test,as appropriate.A receiver operating characteristic(ROC)curve analysis was applied to assess the diagnostic performance of FGF-19 and alpha fetoprotein(AFP)for HCC detection.APvalue of less than 0.05 was considered statistically significant.
RESULTS
This study included 90 participants divided into control,cirrhosis,and HCC groups.The HCC group was comprised of 19 males(63.3%)and 11 females(36.7%),with a mean age of 57.37 years.In the cirrhotic group,there were 20 males(66.7%)and 10(33.3%)females,with a mean age of 53.57 years.The control group included 18 males(60%)and 12 females(40%),with a mean age of 51.07 years(Table 1).According to the Child-Pugh class,14 of the HCC cases(46.7%)belonged to Class C,while 18(60%)of the cirrhotic cases belonged to Class A(P=0.002,Table 1).There were statistically significant differences among the three groups concerning AFP,haemoglobin,platelets,alanine aminotransferase,aspartate aminotransferase(AST),albumin,international normalised ratio(INR),fasting blood glucose,and bilirubin(Table 1).
We detected a high statistically significant difference in the FGF-19 levels of the three groups.The highest level occurred in the HCC group,followed by the cirrhosis and control groups(236.44 ± 40.94vs125.63 ± 31.54vs69.60 ± 20.90 pg/mL,respectively,P≤ 0.001;Table 1,Figure 1).There were seven HCC patients with negative AFP;however,they had elevated FGF-19 levels(> 180 pg/mL).Serum FGF-19 levels were not significantly different according to the Child-Pugh class in the cirrhosis and HCC groups(Table 2).
The tumour characteristics of the HCC cases are shown in Table 3.Serum FGF-19 levels were higher in relation to the size of the tumour,the presence of portal vein thrombosis,jaundice,lower limb oedema,and weight loss;however,these differences did not reach statistical significance(Table 4).FGF-19 was positively correlated with AFP(r=0.383,P=0.003)and INR(r=0.357,P=0.005),while it was negatively correlated with albumin(r=-0.500,P≤ 0.001;Table 5,Figure 2).

Table 1 Characteristics of all participants

HBV:Hepatitis B virus;HCC:Hepatocellular carcinoma;HCV:Hepatitis C virus;INR:International normalised ratio.

Table 2 Serum fibroblast growth factor 19 levels in the cirrhosis and hepatocellular carcinoma groups according to Child-Pugh score
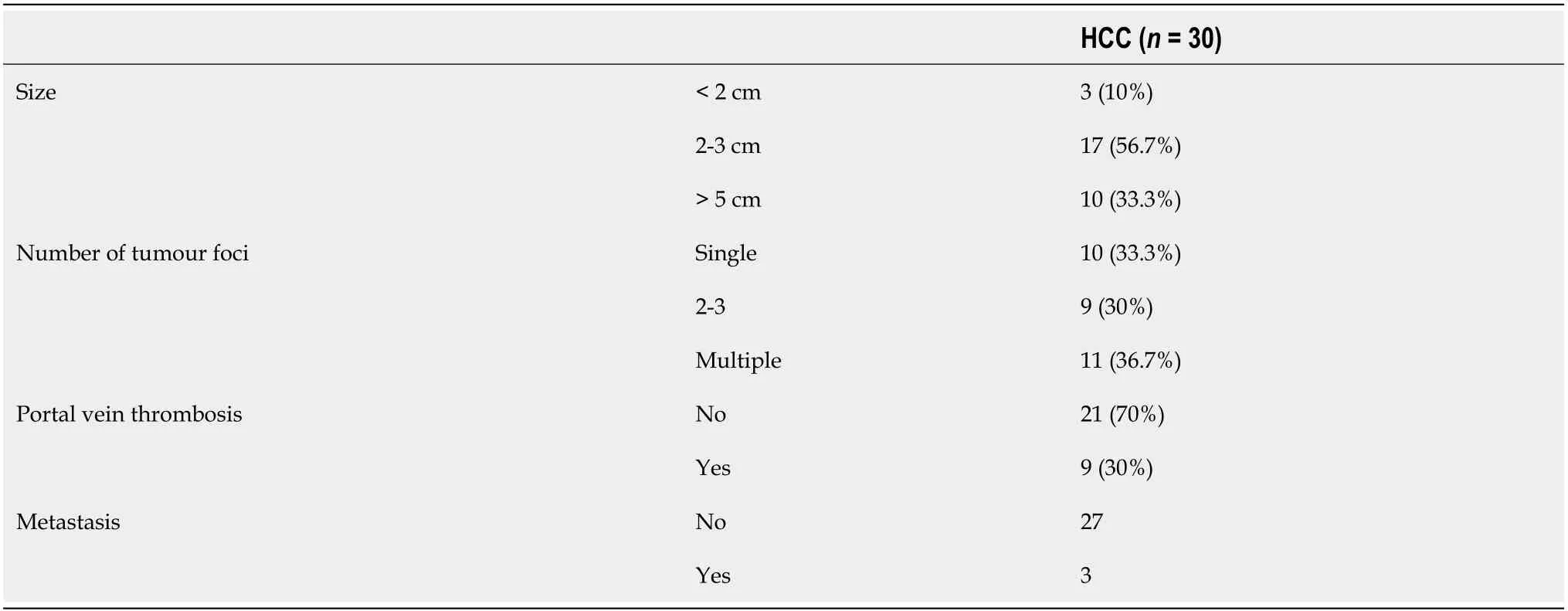
Table 3 Tumour characteristics of hepatocellular carcinoma cases
For the detection of HCC,the ROC curve analysis showed that the best cut-off point of AFP was > 8.2 ng/mL with an area under the curve(AUC)of 0.78,sensitivity of 63.33%,specificity of 83.33%,positive predictive value(PPV)of 79.2%,negative predictive value(NPV)of 69.4%,and total accuracy of 78%.However,FGF-19 at a cut-off point > 180 pg/mL had an AUC of 0.98,sensitivity of 100%,specificity of 90.0%,PPV of 90.0%,NPV of 100%,and total accuracy of 98%(Table 6,Figure 3).
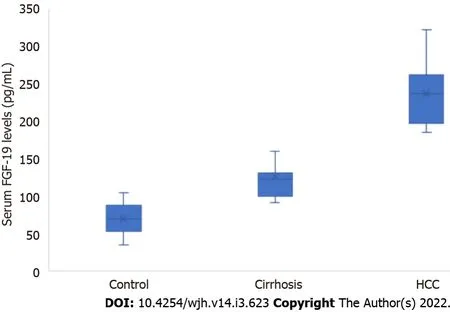
Figure 1 Serum fibroblast growth factor 19 levels in the control,cirrhosis,and hepatocellular carcinoma groups.FGF-19:Fibroblast growth factor 19;HCC:Hepatocellular carcinoma.
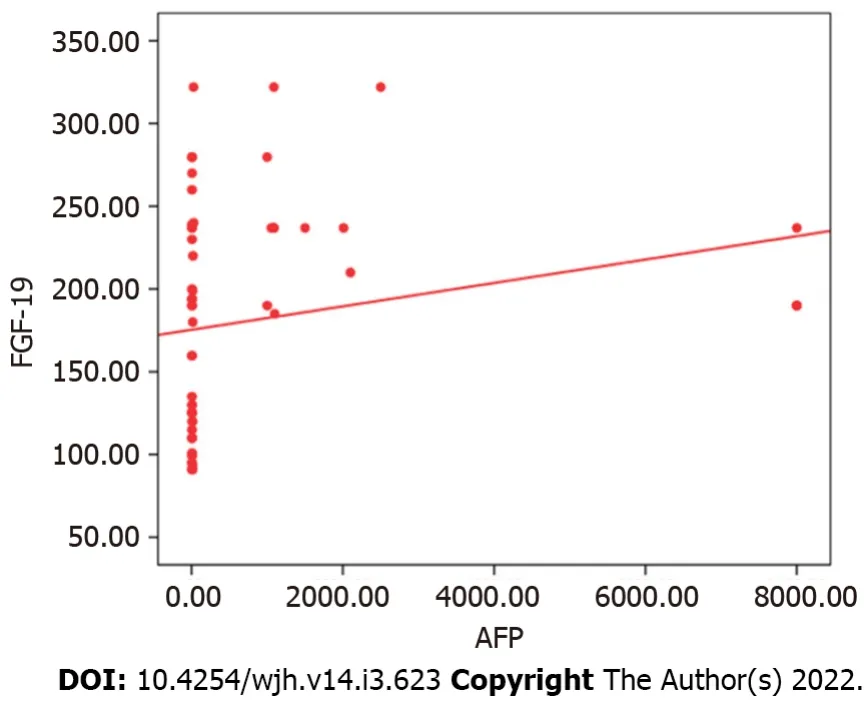
Figure 2 Correlation between serum fibroblast growth factor 19 and alpha fetoprotein.AFP:Alpha fetoprotein;FGF-19:Fibroblast growth factor 19.
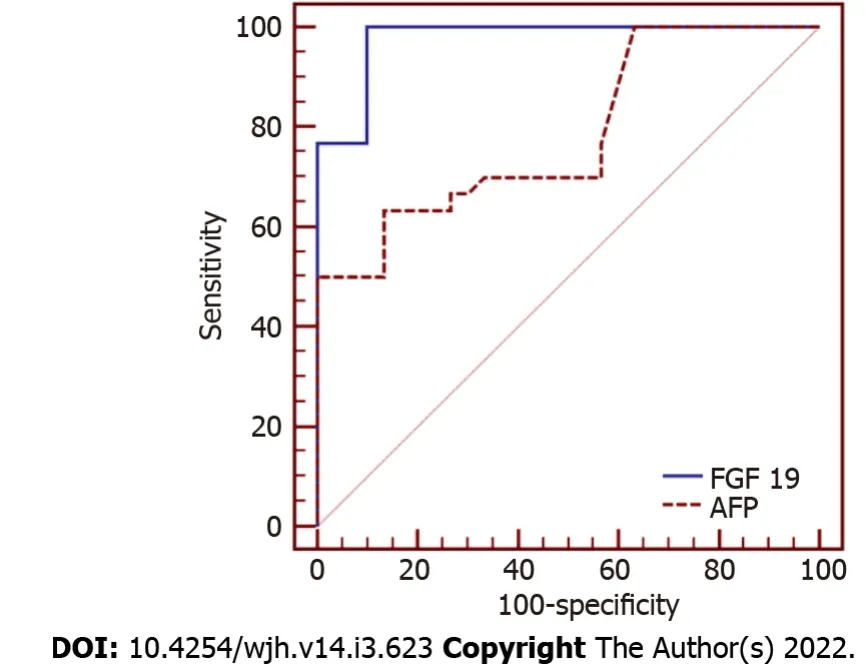
Figure 3 Receiver operating characteristic curves for assessing the diagnostic performance of FGF-19 and alpha fetoprotein for the differentiation of HCC cases.AFP:Alpha fetoprotein;FGF-19:Fibroblast growth factor 19.
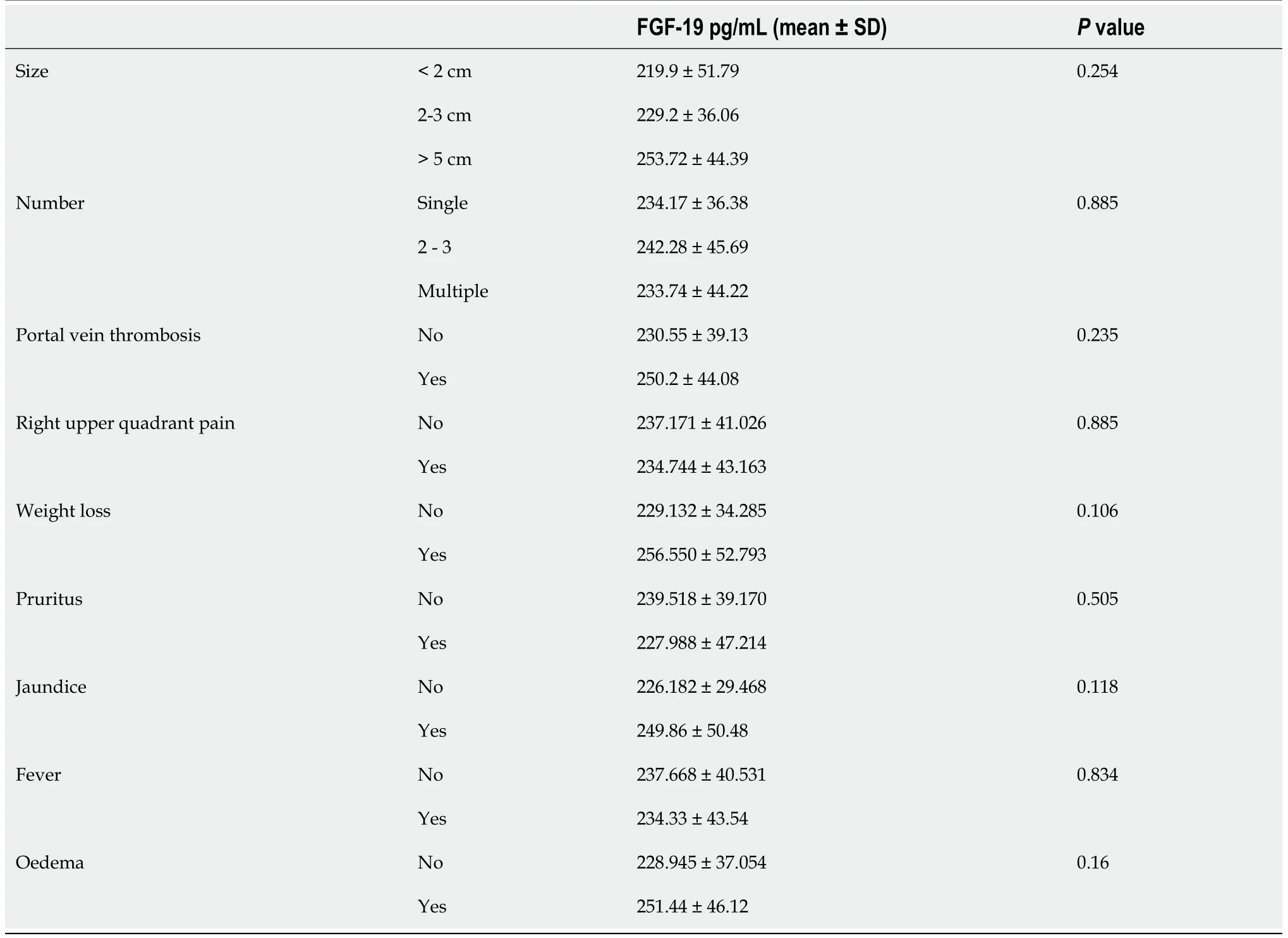
Table 4 Serum fibroblast growth factor 19 levels according to variables in the hepatocellular carcinoma group

Table 5 Correlation between fibroblast growth factor 19 and alpha fetoprotein with patients’ laboratory data

Table 6 Diagnostic performance of fibroblast growth factor 19 and alpha fetoprotein for differentiation of hepatocellular carcinoma cases
DlSCUSSlON
HCC is the third highest cause of tumour death globally,with a 5-year survival rate of approximately 20% despite the developments in imaging technologies and therapeutic methodologies[29].Unfortunately,the majority of HCC patients are diagnosed at an advanced stage of disease;therefore,early recognition of the disease is crucial to improving the prognosis and overall survival of patients[24].
Tumour markers have commonly been utilised for numerous objectives,such as diagnosis,follow-up care after treatment,optimisation of therapeutic effectiveness,and prediction of prognosis.Earlier studies have identified various serum markers for HCC which can be applied as diagnostic and prognostic markers for HCC.Although the assessment of these biomarkers is not essential for establishing a conclusive diagnosis of HCC as per the guidelines,these biomarkers play a key role in HCC diagnosis and monitoring[28,30,31].However,it has been found that AFP,which is the most studied marker,may remain in the normal range not only in the early stages,but also in the advanced stages of HCC[32].Moreover,an increase of AFP is occasionally detected in cirrhotic patients.Considering these two facts,alternative serum markers with high levels of sensitivity and specificity are needed.
It has previously been reported that FGF-19 may be associated with the pathogenesis and clinical characteristics of HCC[12,24].Thus,we aimed to investigate the diagnostic utility of FGF-19 in HCC cases.We observed significantly higher serum FGF-19 levels in the HCC group compared to the control and cirrhosis groups.Serum FGF-19 levels were also higher in relation to the size of the tumour and presence of portal vein thrombosis;however,these differences did not reach statistical significance owing to the small sample size.
In accordance with our results,Maedaet al[12]detected higher serum levels of FGF-19 in their HCC group(214.5 pg/mL)compared to the cirrhosis group(100.1 pg/mL,P< 0.001)and the control group(78.8 pg/mL,P=0.002).However,no statistically significant difference was detected between the cirrhotic cases and controls in their study.
Similar to the current results,Liet al[24]detected significantly higher serum FGF-19 levels in the HCC group compared to the control group(145.57 ± 118.72vs90.18 ± 13.88 pg/mL,P=0.044).They also reported that FGF-19 levels were significantly raised in the HCC tissues(57.80 ± 4.39 pg/10 mg total protein)in comparison to both healthy control tissues(33.29 ± 1.53 pg/10 mg total protein,P< 0.001)and paired peritumoral tissues(46.33 ± 2.53 pg/10 mg total protein,P=0.032).Additionally,FGF-19mRNA expression was significantly raised in the HCC tissues in comparison to paired peritumoral tissues(3.30 ± 1.82vs2.25 ± 0.82,respectively,P=0.025).Moreover,FGF-19 expression increased significantly with a strong positive correlation(r=0.968)consistent with the histological severity of hepatic disease,showing a trend in samples with steatosis(224.13 ± 115.68,P=0.087),steatohepatitis(413.99 ± 159.55,P=0.002),cirrhosis(613.35 ± 157.29,P< 0.001),and HCC(2507.28 ± 831.10,P=0.001)in comparison to the paired peritumoral tissues(142.96 ± 41.32).
Our results are also consistent with those of Sunet al[33],who detected higher FGF-19 levels in the HCC and diabetes-HCC groups than in the control and diabetes groups(220.5,185.1,115.8,and 70.4 pg/mL,respectively,P< 0.001).All these results indicate that FGF-19 may have a role in the pathogenesis of HCC.
In line with the results of the current research,Sunet al[33]detected a positive association between FGF-19 and AFP in HCC patients(P< 0.05).However,Maedaet al[12]found no significant association between serum FGF-19 concentrations and AFP.Moreover,in partial agreement with the present study,Wunschet al[34]observed that serum and hepatic concentrations of FGF-19 were associated with the severity of hepatic disease,as measured by laboratory parameters including albumin(r=-0.408,P=0.007),haemoglobin(r=-0.394,P=0.01),AST(r=0.328,P=0.03),and total bilirubin(r=0.577,P<0.001).
For HCC detection,in the study by Maedaet al[12],the ROC curve analysis determined a cut-off point of FGF-19 of 200 pg/mL,which had an AUC of 0.795,sensitivity of 53.2%,specificity of 95.1%,PPV of 95.9%,and NPV of 48.7%.This result was comparable to those of AFP(AUC=0.827).However,in the current study,FGF-19 had a better diagnostic performance at a cut-off > 180 pg/mL with an AUC of 0.98,sensitivity of 100%,specificity of 90%,PPV of 90%,and NPV of 100%.
The current study was limited by a small sample size and a high ratio of patients with advanced HCC.Further studies are needed to investigate the clinical applications of the current results.FGF-19 could serve as a predictor of prognosis and a marker for follow-up after HCC treatment.Additionally,the FGF-19 pathway has received increased interest as a possible therapeutic target in chronic liver diseases[5,35-37].In fact,anti-FGF-19 antibody therapy has been described as inhibiting HCC evolution in FGF-19 transgenic mice[38].
CONCLUSlON
FGF-19 could be a possible novel non-invasive marker for HCC.It may improve the prognosis of HCC patients due to its utility in several aspects of HCC detection and management.
ARTlCLE HlGHLlGHTS
Research background
Fibroblast growth factor 19(FGF-19)is one of the founding members of the endocrine FGF subfamily.Recently,it has been the subject of much interest owing to its role in various physiological processes affecting glucose and lipid metabolism and bile acid secretion as well as cell proliferation,differentiation,and motility.Additionally,FGF-19 secretion in an autocrine style has reportedly contributed to cancer progression in various types of malignancies including hepatocellular carcinoma(HCC).
Research motivation
Tumour markers for HCC with a high sensitivity and specificity are necessary.
Research objectives
We aimed to estimate the serum FGF-19 concentrations in HCC cases and assess the diagnostic performance of FGF-19 for the detection of HCC.
Research methods
We recruited 90 adult participants and divided them into three equal groups:Healthy controls,cirrhosis patients,and HCC patients.Serum FGF-19 concentrations were measured using the Human FGF-19 ELISA kit.
Research results
We detected a high statistically significant difference in the FGF-19 levels between the three groups,with the highest level occurring in the HCC group,followed by the cirrhosis and control groups(236.44± 40.94vs125.63 ± 31.54vs69.60 ± 20.90 pg/mL,respectively,P ≤ 0.001).For the detection of HCC,ROC curve analysis showed that FGF-19 produced a better diagnostic performance than alpha fetoprotein with an AUC of 0.98vs0.78.
Research conclusions
FGF-19 may be a possible novel non-invasive marker for HCC.
Research perspectives
FGF-19 could serve as a predictor of prognosis and a marker for follow-up after HCC treatment.Furthermore,the FGF-19 pathway may be a therapeutic target for the management of HCC.
FOOTNOTES
Author contributions:Mohamed GA,Nashaat EH,and ElGhandour AM designed the study;Fawzy HM participated in the acquisition of the data;Mohamed GA,Nashaat EH,Fawzy HM,and ElGhandour AM participated in the analysis and interpretation of the data;Mohamed GA,Nashaat EH,Fawzy HM,and ElGhandour AM revised the article critically for important intellectual content;Mohamed GA wrote the manuscript.
lnstitutional review board statement:The study was reviewed and approved by the institutional review board of Faculty of Medicine,Ain Shams University,Cairo,Egypt.
lnformed consent statement:Informed consent was obtained from every participant before the enrolment into the study.
Conflict-of-interest statement:All authors have nothing to disclose.
Data sharing statement:The statistical code and dataset are available from the corresponding author at ghadaabdelrahman@med.asu.edu.eg.The participants gave informed consent for the data sharing.
STROBE statement:The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared and revised according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Egypt
ORClD number:Ghada Abdelrahman Mohamed 0000-0003-0320-1011;Ehab Hasan Nashaat 0000-0002-7686-6463;Hadeer Mohamed Fawzy 0000-0001-7941-0931;Ahmed Mohamed ElGhandour 0000-0002-6106-4636.
S-Editor:Ma YJ
L-Editor:Wang TQ
P-Editor:Ma YJ
杂志排行

World Journal of Hepatology的其它文章
- Hepatitis E in immunocompromised individuals
- Small duct primary sclerosing cholangitis:A discrete variant or a bridge to large duct disease,a practical review
- New progress in understanding roles of nitric oxide during hepatic ischemia-reperfusion injury
- Renal manifestations of hepatitis E among immunocompetent and solid organ transplant recipients
- Safety of direct acting antiviral treatment for hepatitis C in oncologic setting:A clinical experience and a literature review
- Fertaric acid amends bisphenol A-induced toxicity,DNA breakdown,and histopathological changes in the liver,kidney,and testis