Renal manifestations of hepatitis E among immunocompetent and solid organ transplant recipients
2022-04-02KarthikKovvuruNicholasCarbajalAbhinandanReddyPakanatiCharatThongprayoonPanupongHansrivijitBoonphiphopBoonphengPattharawinPattharanitimaVoravechNissaisorakarnWisitCheungpasitpornSwethaKanduri
Karthik Kovvuru,Nicholas Carbajal,Abhinandan Reddy Pakanati,Charat Thongprayoon,Panupong Hansrivijit,Boonphiphop Boonpheng,Pattharawin Pattharanitima,Voravech Nissaisorakarn,Wisit Cheungpasitporn,Swetha R Kanduri
Karthik Kovvuru,Nicholas Carbajal,Swetha R Kanduri,Department of Medicine,Ochsner Clinic Foundation,New Orleans,LA 70121,United States
Abhinandan Reddy Pakanati,Department of Medicine,The Kidney Clinic LLC,Snellville,GA 30078,United States
Charat Thongprayoon,Department of Nephrology and Hypertension,Mayo Clinic,Rochester,MN 55905,United States
Panupong Hansrivijit,Department of Internal Medicine,UPMC Pinnacle,Harrisburg,PA 17104,United States
Boonphiphop Boonpheng,Department of Nephrology,David Geffen School of Medicine,University of California,Los Angeles,CA 90095,United States
Pattharawin Pattharanitima,Department of Internal Medicine,Faculty of Medicine,Thammasat University,Pathum Thani 12121,Thailand
Voravech Nissaisorakarn,Department of Internal Medicine,MetroWest Medical Center,Tufts University School of Medicine,Boston,MA 01760,United States
Wisit Cheungpasitporn,Department of Medicine,Mayo Clinic,Rochester,MN 55905,United States
Abstract Hepatitis E virus(HEV)infections are generally self-limited.Rare cases of hepatitis E induced fulminant liver failure requiring liver transplantation are reported in the literature.Even though HEV infection is generally encountered among developing countries,a recent uptrend is reported in developed countries.Consumption of unprocessed meat and zoonosis are considered to be the likely transmission modalities in developed countries.Renal involvement of HEV generally holds a benign and self-limited course.Although rare cases of cryoglobulinemia are reported in immunocompetent patients,glomerular manifestations of HEV infection are frequently encountered in immunocompromised and solid organ transplant recipients.The spectrum of renal manifestations of HEV infection include prerenal failure,glomerular disorders,tubular and interstitial injury.Kidney biopsy is the gold standard diagnostic test that confirms the pattern of injury.Management predominantly includes conservative approach.Reduction of immunosuppressive medications and ribavirin(for 3-6 mo)is considered among patients with solid organ transplants.Here we review the clinical course,pathogenesis,renal manifestations,and management of HEV among immunocompetent and solid organ transplant recipients.
Key Words:Hepatitis E;Acute kidney injury;Glomerular disorders;Kidney biopsy;Solid organ transplant;Kidney transplant
lNTRODUCTlON
Hepatitis E virus(HEV)has a pronounced worldwide distribution.It is a spherical,single-strand RNA virus consisting of three partially overlapping open reading frames(ORF)ORF1,ORF2,and ORF3[1].HEV belongs to hepeviridae family,and eight genotypes of HEV(HEV1 to HEV 8)have been identified[2,3].Genotypes HEV1 and HEV2 are routinely encountered in developing countries and are transmitted through fecal-oral route.HEV3 and HEV4 are associated with sporadic autochthonous infection among western countries and are predominantly transmitted through animal reservoirs and ingestion of uncooked meat[4-6].Additionally,HEV genome 3 related infection is associated with solid organ transplant recipients and immunocompromised patients.Other uncommon modalities of transmission could occur through blood products and solid organ transplants[7,8].Transfusion-related transmission is not common in the United States,but is reported in countries like China and Japan[9,10].Lastly,vertical transmission of HEV infection from mother to fetus could be up to 100%,as reported by Kumaret al[11]and is associated with fatal outcomes.
CLlNlCAL COURSE
HEV infection commonly holds a benign,self-limiting course,and the case-fatality rate in developing countries is estimated to be 0.5%-4%[12,13].Clinical presentation of HEV infection is similar to that of hepatitis A.Majority of the infected patients sustain mild and asymptomatic course.Acute HEV infection is accompanied by jaundice,icteric eyes,malaise,anorexia,and abdominal discomfort.Severe infection is usually reported among patients with underlying chronic liver disease and is associated with increased mortality[14].Additionally,solid organ transplant recipients encounter a more sustained course[15].Among such patients,HEV antibody production could be delayed,often leading to sustained viremia with progression to chronic hepatitis and cirrhosis[16,17].
Pregnant women can suffer a complicated course with fulminant HEV infection and sustain higher mortality rates compared to non-pregnant cohorts.It is estimated that fatality rates reach 10%-40%among pregnant women[11,18].Both obstetric and non-obstetric complications are encountered.Nonobstetric complications include fulminant hepatic failure,acute liver failure,acute cerebral edema and obstetric complications include pre-term delivery,antepartum hemorrhage,intrauterine fetal demise[19-21].
RENAL MANlFESTATlONS OF HEV lNFECTlON
Non-glomerular manifestations
Renal manifestations of hepatitis B and hepatitis C(HBV,HCV)infection are well described.The association between HEV infection and kidney is established as the HEV particles are isolated from the urine of infected patients[22,23].Additionally,when urine of infected monkeys was induced into healthy animals,the development of HEV infection was well appreciated and confirmed the infectious nature of the viral particles shed in the urine[23].HEV-associated renal manifestations include prerenal or intrinsic renal disorders.Among intrinsic renal conditions,glomeruli and tubules are the affected sites[24,25].
HEV infection is less commonly associated with the progression of kidney disease in immunocompetent patients.Chronic HEV infection and subsequent development of decompensated liver cirrhosis are frequently encountered among solid organ transplant recipients.Hepatorenal physiology secondary to increased circulating vasoactive agents like nitric oxide is often noted.Similar to other cirrhotic patients,HEV-associated liver dysfunction patients could have increased vasodilatory mediators released secondary to shear stress on the portal vasculature,leading to splanchnic vasodilatation,portosystemic shunting,and bacterial translocation.Additionally,reduction in effective arterial blood volume perpetuates decrease in renal perfusions that ultimately leads to renal vasoconstriction[26].Urine sodium levels remain low,indicating prerenal failure.However,prolongation of renal hypoperfusion contributes to ischemic injury of the proximal tubule with manifestations of acute tubular necrosis[13].
Bile cast nephropathy,also called cholemic nephrosis,is typically encountered among patients with cholestasis secondary to advanced cirrhosis or acute liver failure.Nayaket al[27]reported a case of cholemic nephrosis secondary to acute HEV infection.Historically,the diagnosis is made by kidney biopsy with the presence of bile cast obstructing distal tubules.The pathogenesis of cholemic nephrosis is not completely understood,however,it is hypothesized secondary to intraluminal obstruction of the bile cast along with direct tubular toxicity[28,29].
Cases of hemolysis and subsequent renal failure are reported with HEV infection.Karkiet al[30]reported a case of massive hemolysis in a patient with glucose-6-phosphate dehydrogenase(G6PD)deficiency,heme pigment causing direct proximal tubular toxicity.Development of hemoglobin cast further leads to intratubular obstruction and subsequent development of acute kidney injury.It is hypothesized that the liver dysfunction secondary to acute HEV leads to accumulation of toxins along with the depletion of antioxidants like glutathione.Additionally,if patients have underlying G6PD deficiency,massive hemolysis,and acute kidney injury are encountered[31](Figure 1).
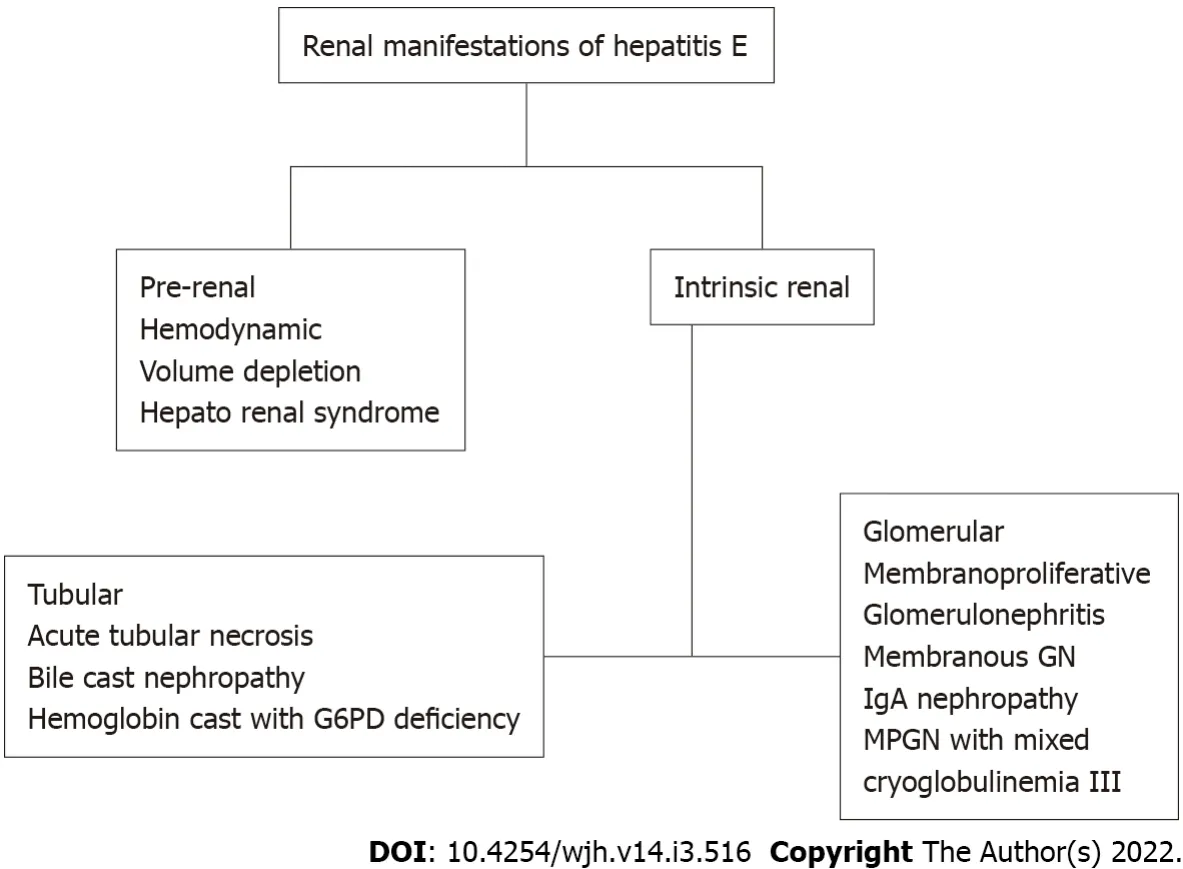
Figure 1 Causes of acute kidney injury in acute hepatitis E virus-infected patients.
Glomerular manifestation
Glomerular manifestations of HEV infection are reported among solid organ transplant recipients associated with HEV genotype 3.However,it is unclear if renal manifestations and presentation differ among various organ transplant recipients.While glomerular manifestations are commonly noted among immunocompromised patients[32,33],autochthonous HEV-induced membranoproliferative glomerular pattern was reported in an immunocompetent individual[33].
Study by Kamaret al[34]evaluated the renal function of patients with HEV infection in solid organ transplants recipients.Out of total 51 cases of genotype 3 HEV infections,43.2% were cleared of the virus spontaneously within 6 mo of infection,whereas 56.8% progressed to chronic hepatitis.Among 36 kidney and kidney-pancreas-transplant patients,glomerular filtration rate(GFR)significantly decreased from baseline of 52.9 ± 17.7 mL/min at four-month median before HEV infection to 48.8 ± 18.7 mL/min during acute HEV infection(P=0.04).Acute rejection episode,infection,modification in immunosuppressant type or dose,and functional renal insufficiency were ruled out,and the GFR decline is attributed to acute HEV infection.Proteinuria levels significantly increased in four kidney-transplant patients at HEV diagnosis,which subsequently improved with improvement in renal functions and HEV clearances.
Kidney biopsy performed during acute phase revealed patterns of membranoproliferative glomerulonephritis,cryoglobulinemia II and III types,and IgA nephropathy[34].Additionally,among patients who developed chronic hepatitis,12 patients who received anti-viral therapy with ribavirin for three months had clearances of HEV with subsequent improvement in GFR at 6 mo follow up.Interestingly,In the subgroup who received anti- viral therapy,cryoglobulinemia was detected in 70% of patients before therap,eventually became undetectable in all patients after viral clearance.Renal manifestations of the reported cases of HEV infection among immunocompetent and solid organ recipients are summarized in Table 1.

Table 1 Renal manifestations of the reported cases of hepatitis E virus infection among immunocompetent and solid organ recipients
PATHOPHYSlOLOGY OF HEV-lNDUCED RENAL lNJURY
Pathophysiology of HEV-induced kidney injury is not completely known.HEV-mediated renal manifestations were thought to be a result of direct cytopathic injury due to the viral infection per se or related to immune-mediated mechanisms.Similar to HBV and HCV,it is hypothesized that HEV plays a role in precipitating glomerular injury through immune complex-mediated mechanisms[35].The study by El- Mokhtaret al[36]assessed the role of immune-mediated mechanisms in HEV-induced renal dysfunction.CD10 and CD13 positive proximal tubular epithelial cells were isolated and challengedin vitrowith HEV inoculum.HEV infection minimally upregulated inflammatory markers in the absence of peripheral blood mononuclear cells,and no measurable changes were noted in lactate dehydrogenase(LDH)levels,kidney injury molecules,or transcription of chemokines.However,when the HEV infected proximal tubular cells were inoculated with peripheral blood mononuclear cells,there was upregulation of inflammatory molecules,kidney injury markers,and LDH levels,indicating that HEV infection per se might not be completely responsible for glomerular injury.Thus,it is the intersection between immune cells,HEV infection,and proximal tubular epithelial cells that contribute to renal injury[36].
MANAGEMENT OF RENAL MANlFESTATlONS OF HEV lNFECTlON
Diagnostics
Over the recent years,HEV laboratory testing has been refined drastically.Two main methods for testing HEV currently are indirect and direct serological tests.With regards to indirect studies,there are commercially available kits for serological testing for the presence of anti-HEV IgM and anti-HEV IgG that relies on the presence of antibodies in the serum to detect infection[37].In addition,indirect studies rely heavily on patient’s immune response to HEV infection,decreasing sensitivity in immunocompromised patients to some degree[38].Direct testing predominately uses more advanced nucleic acid testing,that worksviadetecting the presence of viral genetic material in the form of nucleic acid sequences(HEV RNA)to determine the presence or absence of infection along with detection of viral capsid antigens[39,40].
In Immunocompetent patients,it is advised to check anti-HEV IgM initially for suspected HEV infection[41].A negative test rules out the disease,however,if the test is positive,HEV RNA analysis is needed.On the other hand,among immunocompromised patients,it is recommended to test HEV-RNA even with negative anti-HEV IgM in blood and in stool before ruling out HEV infection[37].Urine studies and electrolytes give subtle clues in identifying various causes of AKI.Urine microscopy adds an additional advantage to diagnose patients with acute tubular necrosis in the presence of muddy brown granular cast.Kidney biopsy remains the gold standard diagnostic testing for glomerular disorders and tubular obstructions,including bile cast nephropathy,while evaluating renal manifestations of HEV.Patients with acute or chronic hepatitis with new-onset proteinuria should be considered for kidney biopsy[42].
Treatment
Management of HEV-associated renal manifestations depends on the clinical presentation.Treatment is predominantly based on a conservative approach given benign course of the disease.Acute infection with HEV usually does not require anti-viral therapy.In patients with severe acute infection or acute on chronic liver disease,ribavirin therapy is considered[42].For patients with acute kidney injury secondary to acute tubular necrosis or bile cast nephropathy,routine care to maintain mean arterial pressures,avoid nephrotoxic agents,and further insults are recommended.Indications for initiation of renal replacement therapy are similar to routine indications of dialysis initiation.Management of HEVassociated glomerular disorders should be based on underlying pathology.Guinaultet al[33]reported a case of HEV-induced cryoglobulinemic glomerulonephritis in an immunocompetent patient with serum monoclonal IgG k light chain type II cryoglobulin.Renal biopsy results were consistent with lobular membranoproliferative exudative glomerulonephritis with fibrinoid necrosis and cellular crescents with a ruptured Bowman capsule.The patient was subsequently treated with seven sessions of plasma exchange along with pulse steroids with improvement in HEV RNA titers and cryoglobulinemic levels.Occasionally acute HEV infection follows a fulminant course as reported in pregnant individuals and could manifest as acute cerebral edema,seizures,acute fatty liver and are associated with increased mortality[43].
While managing patients with solid organ transplants,benefits of treatment need to be weighed against risks of rejection.Reduction of immunosuppression is considered the first-line approach[44],allowing HEV clearance in about one-third of patients.Ribavirin,an anti-viral agent,is considered in patients with severe acute or acute on chronic liver failure[45,46].It has also been postulated that ribavirin acts by inhibiting HEV viral replication and increases the expression of interferon stimulating genes leading to immune modulation[47].In a study done by Kamaret al[34],patients who received anti-viral therapy with ribavirin,cryoglobulinemia was detected in 70% of patients before therapy and became undetectable in all patients after viral clearance.Ribavirin is also used successfully to treat HEVassociated membranoproliferative glomerulonephritis in a solid organ transplant recipient[32](Figure 2).

Figure 2 Management of acute kidney injury in acute hepatitis E infected patients.
In a multicenter retrospective study by Karmeret al,solid-organ transplant recipients were treated with ribavirin at a median dose of 600(range,29-1200)mg/d for three months.Similar virological remission was observed in patients who received ribavirin for three months as compared to those who were treated for more than three months.In patients with detectable HEV RNA in the serum and/or in the stool,at the end of three months,ribavirin monotherapy can be continued for an additional three months[48]Hence it is indicated to treat with ribavirin initially for three months and evaluate the response.With non-sustained virological remission,ribavirin is recommended to be continued for a total of 6 mo.Among liver transplant recipients,interferon(IFN)α has shown to achieve sustained virological remission among patients with HEV after liver transplant.However,the use of IFNα is not recommended among other solid organ transplant recipients due to the risk of graft rejection(Table 1).
Sofosbuvir,a nucleotide analog,is evaluated along with ribavirin in patients who failed ribavirin monotherapy.Wezelet al[49]evaluated two solid organ transplant recipients who failed ribavirin monotherapy and observed that sofosbuvir showed variable antiviral activity in chronic HEV patients.Sofosbuvir was ineffective in achieving sustained virological response.Pegylated IFNα has shown efficacy in achieving a sustained virological response in patients with hemodialysis and liver transplants[50].However,given the concern of interference with graft and risk of acute rejection,interferon α is contraindicated in patients with other solid organ transplants[47].
CONCLUSlON
HEV infection is a global health concern and is uncommonly associated with mortality and morbidity.HEV infection is restricted not only to developing countries,but is increasingly identified among developed countries.Renal manifestations of HEV range from prerenal failure,acute tubular necrosis,glomerular disorders,and intratubular obstruction form bile cast nephropathy.Similar to HBV and HCV infections,immune-mediated mechanisms are hypothesized in development of HEV-associated glomerular diseases.Conservative approach is routinely employed in cases of renal involvement from acute hepatitis in immunocompetent patients.Among solid organ transplant recipients,ribavirin is considered in patients with chronic HEV infection for a duration of 3-6 mo along with reduction of immunosuppression.IFNα has shown to achieve sustained virological remission among patients with HEV after liver transplant.However,the use of IFNα is not recommended among other solid organ transplant recipients secondary to the risk of graft rejection.In patients who failed monotherapy with ribavirin,sofosbuvir has been evaluated in conjunction with ribavirin with variable anti-viral effects.Plasma exchange,in addition to pulse steroids is occasionally used in management of crescentic glomerular nephritis associated with HEV infection.
FOOTNOTES
Author contributions:Kovvuru K,Carbajal N,Pakanati AR,Thongprayoon C,Hansrivijit P,Boonpheng B,Pattharanitima P,Nissaisorakarn V and Kanduri SR contributed to acquisition of data,drafting the article;Cheungpasitporn W contributed to overall supervision and final approval.
Conflict-of-interest statement:The authors declared no potential conflicts of interest.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:United States
ORClD number:Karthik Kovvuru 0000-0003-2640-724X;Nicholas Carbajal 0000-0002-8034-9223;Abhinandan Reddy Pakanati 0000-0002-3370-0471;Charat Thongprayoon 0000-0002-8313-3604;Panupong Hansrivijit 0000-0002-5041-4290;Boonphiphop Boonpheng 0000-0002-3022-8861;Pattharawin Pattharanitima 0000-0002-6010-0033;Voravech Nissaisorakarn 0000-0002-9389-073X;Wisit Cheungpasitporn 0000-0001-9954-9711;Swetha R Kanduri 0000-0002-7190-6665.
S-Editor:Zhang H
L-Editor:A
P-Editor:Zhang H
杂志排行

World Journal of Hepatology的其它文章
- Hepatitis E in immunocompromised individuals
- Small duct primary sclerosing cholangitis:A discrete variant or a bridge to large duct disease,a practical review
- New progress in understanding roles of nitric oxide during hepatic ischemia-reperfusion injury
- Safety of direct acting antiviral treatment for hepatitis C in oncologic setting:A clinical experience and a literature review
- Fertaric acid amends bisphenol A-induced toxicity,DNA breakdown,and histopathological changes in the liver,kidney,and testis
- Prevalence of hypothyroidism and effect of thyroid hormone replacement therapy in patients with non-alcoholic fatty liver disease:A population-based study