Predictors of Mortality at 28-days in lnfection associated Acute Kidney lnjury in Cirrhosis
2022-04-02TaranaGuptaNaveenRangaSandeepKumarGoyal
Tarana Gupta,Naveen Ranga,Sandeep Kumar Goyal
Tarana Gupta,Naveen Ranga,Department of Medicine,Pandit Bhagwat Dayal Sharma Post Graduate Institute of Medical Sciences,Rohtak 124001,Haryana,India
Sandeep Kumar Goyal,Independent Researcher,Kangra 176056,Himachal Pradesh,India
Abstract BACKGROUND Acute kidney injury(AKI)in cirrhosis is important complication with poor outcomes.And infections are common cause for acute decompensation.Infections in cirrhosis lead to acute deterioration of hemodynamics leading to precipitation of AKI.AIM To study predictors of mortality in patients with infection-associated AKI in cirrhosis.METHODS This was a prospective,observational study conducted at Tertiary care centre from January 2018 till April 2019.Total 119 participants with cirrhosis of liver presenting with AKI were included into the study.AKI was defined as per international club of Ascites-AKI criteria 2015.Patients were grouped into infection AKI and non-infection AKI.Non-infection AKI included patients with diuretic induced AKI and pre-renal AKI.Logistic regression analysis was used to determine predictors of mortality at 28-d.RESULTS Out of 119 patients,alcohol(n =104)was most common etiology of cirrhosis.The infection AKI included 67(56%)patients and non-infection AKI(n =52)included pre-renal AKI in 36(30%)and diuretic-induced AKI in 16(14%)patients.Infection AKI had significantly higher bilirubin,higher international normalized ratio(INR),low serum sodium,higher total leukocyte count(TLC)and higher prevalence of hepatic encephalopathy(HE)as compared to non-infection AKI.Infection AKI had higher progression of AKI(19/67 vs 2/52;P =0.01)and 28-d mortality(38/67 vs 4/5;P ≤ 0.01)as compared to non-infection AKI.At 28-d,nonsurvivors(n =42)had significantly higher bilirubin,higher INR,low serum sodium,higher TLC and higher prevalence of HE as compared to survivors(n =77).On subgroup analysis of Infection AKI group,on multivariate analysis,serum bilirubin as well as presence of HE were independent predictors of 28-d mortality.There was no significant difference of mortality at 90-d between two groups.CONCLUSION Infection AKI in cirrhosis has a dismal prognosis with higher 28-d mortality as compared to noninfection AKI.Serum bilirubin and presence of HE predict 28-d mortality in infection AKI.
Key Words:Infection;Acute kidney injury;Mortality;Cirrhosis;Bilirubin;Hepatic encephalopathy
lNTRODUCTlON
The onset of jaundice,ascites,hepatic encephalopathy(HE),or gastrointestinal(GI)bleed marks the decompensation of a well-compensated chronic liver disease.The occurrence of ascites is an important benchmark in history of cirrhosis as it tilts the balance[1].It signifies the presence of clinically significant portal hypertension,liver cell dysfunction,hypoalbuminemia,alteration in hemodynamics due to imbalance of vasoconstrictors and vasodilators in the splanchnic and systemic circulation.The splanchnic pooling of blood and systemic vasodilation leads to reduced effective arterial blood volume over a period of time resulting in refractory ascites.Ascites predisposes a patient with cirrhosis to increased incidence of spontaneous bacterial peritonitis(SBP)and acute kidney injury(AKI).In 25-year inception cohort study of patients with cirrhosis by D’Amicoet al[2],it was shown that as stages of cirrhosis progress from 1 to 6,there is decreased 5-year survival.On competing risk analysis,they showed 0.50-0.97 risk of death within 1-year of onset of infections,renal failure or acute-on-chronic liver failure(ACLF)in decompensated cirrhosis[3,4].
The unique structural organization and dual blood supply of the liver plays important role in its immune function.Cirrhosis is associated with immune dysfunction.There is associated impaired Kupffer cell function,sinusoidal capillarization with continuous basement membrane formation leading to impaired exchange of cargo between sinusoidal blood and hepatocytes[5].The gut dysbiosis in cirrhosis leads to increased portal blood endotoxemia,increased lipopolysaccharide levels which due to portosystemic shunting bypasses the liver and reaches directly in systemic circulation.This increases the risk of acquiring bacterial infections in cirrhosis.In addition,there is reduced neutrophil count due to splenic sequestration,associated neutrophil dysfunction with reduced chemotaxis,reduced monocyte and macrophage function with and impaired phagocytosis,impaired natural killer cell function.The CD4 and CD8 T cell function is also reduced[6-8].Liver dysfunction leads to reduced complement proteins and hypoalbuminemia.All these factors predispose patients with cirrhosis towards acquiring infection.Sepsis,on the other hand is a precursor to multiorgan dysfunction.Therefore,we aimed to compare infection associated AKI with non-infection AKI in patients with cirrhosis of liver.We also determined the predictors of mortality in patients with infection AKI.
MATERlALS AND METHODS
Study population and data collection
This was a prospective observational study which included consecutive patients with liver cirrhosis with AKI admitted in Department of Medicine at Pandit Bhagwat Dayal Sharma Post Graduate Institute of Medical Sciences,Rohtak,India from Jan 2018 to June 2019.Liver cirrhosis was defined as per clinical,biochemical,and radiological parameters on ultrasound(nodular liver,portal vein diameter > 13 mm,splenomegaly,presence of collateral)and liver biopsy if needed.After written and informed consent,patients aged 18-70 years with cirrhosis of the liver presenting with AKI were included into the study.Patients aged < 18 years or > 70 years,pregnancy,chronic respiratory disease,chronic kidney disease,and hepatocellular carcinoma were excluded from the study.A detailed history and clinical examination were performed in all patients.AKI was defined as an increase in serum creatinine ≥ 0.3 mg/dL within 48 h;or a percentage increase in serum creatinine ≥ 50% from baseline which is known,or presumed,to have occurred within the prior 7 d.Baseline serum creatinine was defined as serum creatinine obtained in the previous 3 mo.In patients with more than one value within the previous 3 mo,the value closest to the admission time to the hospital was taken as the baseline value.
AKI staging
AKI staging was done as per international club of Ascites criteria;Stage 1 was defined as an increase in serum creatinine ≥ 0.3 mg/dL or ≥ 1.5-2 ULN from baseline,Stage 2 as an increase in serum creatinine >2-3 ULN from baseline and Stage 3 as increase in serum creatinine > 3 ULN from baseline or serum creatinine ≥ 4.0 mg/dL with an acute increase ≥ 0.3mg/dL or initiation of renal replacement therapy.Further “Progression” of AKI was defined as progression to a higher stage and/or need of renal replacement therapy and “Regression” was defined as regression of AKI to a lower stage.The response to treatment was defined as “Full response” when serum creatinine value decreased to within 0.3 mg/dL of the baseline value,“Partial response” if reduction of serum creatinine ≥ 0.3mg/dL above baseline value and “No response” if there was no response in creatinine values.All patients were followed till 3 months to evaluate for 28-d and 90-d mortality.On admission,all patients were evaluated for the presence of infection by performing ascitic fluid analysis,blood culture,urine examination,urine culture,sputum gram stain and culture,chest X-Ray,and any other body fluid examination as indicated.
Pneumonia:Any new lung infiltrate with either symptom(cough,sputum,pleuritic pain,dyspnoea)or rales/crepitation on auscultation with components of systemic inflammatory response,i.e.,temperature> 38 °C or < 36 °C or TLC > 10000/mm3or < 4000/mm3or respiratory rate > 20/min or PaCO2< 32 mmHg or pulse > 90/min.
SBP:Either ascitic fluid PMNs(polymorphonuclear)> 250 cells/mm3with/without a positive ascitic fluid culture.
Spontaneous bacterial empyema:Either pleural fluid PMNs > 250 cells/mm3with positive culture or >500 cells/mm3irrespective of culture positivity.
Bacteraemia:Blood culture positivity without any source of infection.
Cellulitis
Urinary tract infection(UTI):Urine microscopy showing WBC > 10/high power field with/without positive culture.
All patients with AKI were grouped into infection AKI,diuretic induced AKI and pre-renal AKI.Diuretic induced AKI was defined as patients who were on diuretics(furosemide and spironolactone)for the control of ascites with negative work up for infection or pre-renal causes.Pre-renal AKI was defined in patients with cirrhosis presenting with upper GI bleed,fluid losses due to diarrhea or vomitingetc.and with negative work up for infections and no history of diuretics.Diuretic induced AKI and pre-renal AKI were grouped as non-infection AKI.
Statistical analysis
All continuous variables were taken as mean ± SD(range)or median[IQR;Q1,Q3]and categorical variables as frequency and percentages.For comparison of continuous variables,Mann-Whitney U test/Student t-test and for categorical variables,χ2and Fisher exact tests were used.28-and 90-d mortality was assessed using survival analysis.P< 0.05 was taken as significant.SPSS v21.0(IBM,USA)was used for analysis.
RESULTS
Out of 140 patients of cirrhosis with AKI were admitted during the study period,21 patients did not fulfil inclusion criteria(Figure 1).Finally,119 patients of cirrhosis with AKI were included into the study.
The most common etiology of cirrhosis was alcohol(n=98),chronic hepatitis B and C(n=5 each),non-alcoholic steatohepatitis related cirrhosis(n=4),both alcohol and chronic hepatitis C(n=4),both alcohol and chronic hepatitis B(n=2),and autoimmune cirrhosis(n=1).
Among 119 patients,infection with AKI was present in 67(56%).Non-infection AKI included 36(30%)patients with pre-renal and 16(14%)patients with diuretic induced AKI(Figure 1).Out of 67 patients of infection AKI,SBP was present in 30(45%),pneumonia in 9(13%),cellulitis in 7(10%),UTI in 2(3%),splenic abscess in 1(1.5%)and source of infection unidentified in 18(27%)patients.
At baseline,Infection AKI group had higher creatinine(2.6 mg/dLvs2.2 mg/dL,P=0.016)as compared to non-infection AKI.Further,infection AKI group had higher mean serum bilirubin,higher INR,lower serum albumin,lower serum sodium,higher haemoglobin,higher TLC,and higher prevalence of HE than non-infection AKI group respectively(Table 1).
Infection AKI had higher progression of AKI(19/67vs2/52;P=0.01)and higher 28-d mortality(38/67vs4/52;P< 0.001)than non-infection AKI group respectively.In non-infection AKI group,four non-survivors belonged to prerenal AKI.At 90-d,there was no significant difference of mortality among infection AKI and non-infection AKI group(49/67vs13/52;P=0.2)respectively(Table 2).
Overall,out of 119 patients,at 28-d,there were 77 survivors and 42 non-survivors.On univariate analysis,survivors had lower serum bilirubin,lower INR,lower TLC,and lower prevalence of HE compared to non-survivors.The multivariate analysis revealed higher bilirubin and presence of HE to predict 28-d mortality(Table 3).
In subgroup analysis of Infection AKI group,non-survivors(n=38)had higher TLC,higher bilirubin,higher INR and higher prevalence of HE as compared to survivors(n=29).On multivariate analysis,serum bilirubin and presence of HE were independent predictors of 28-d mortality(Table 4).
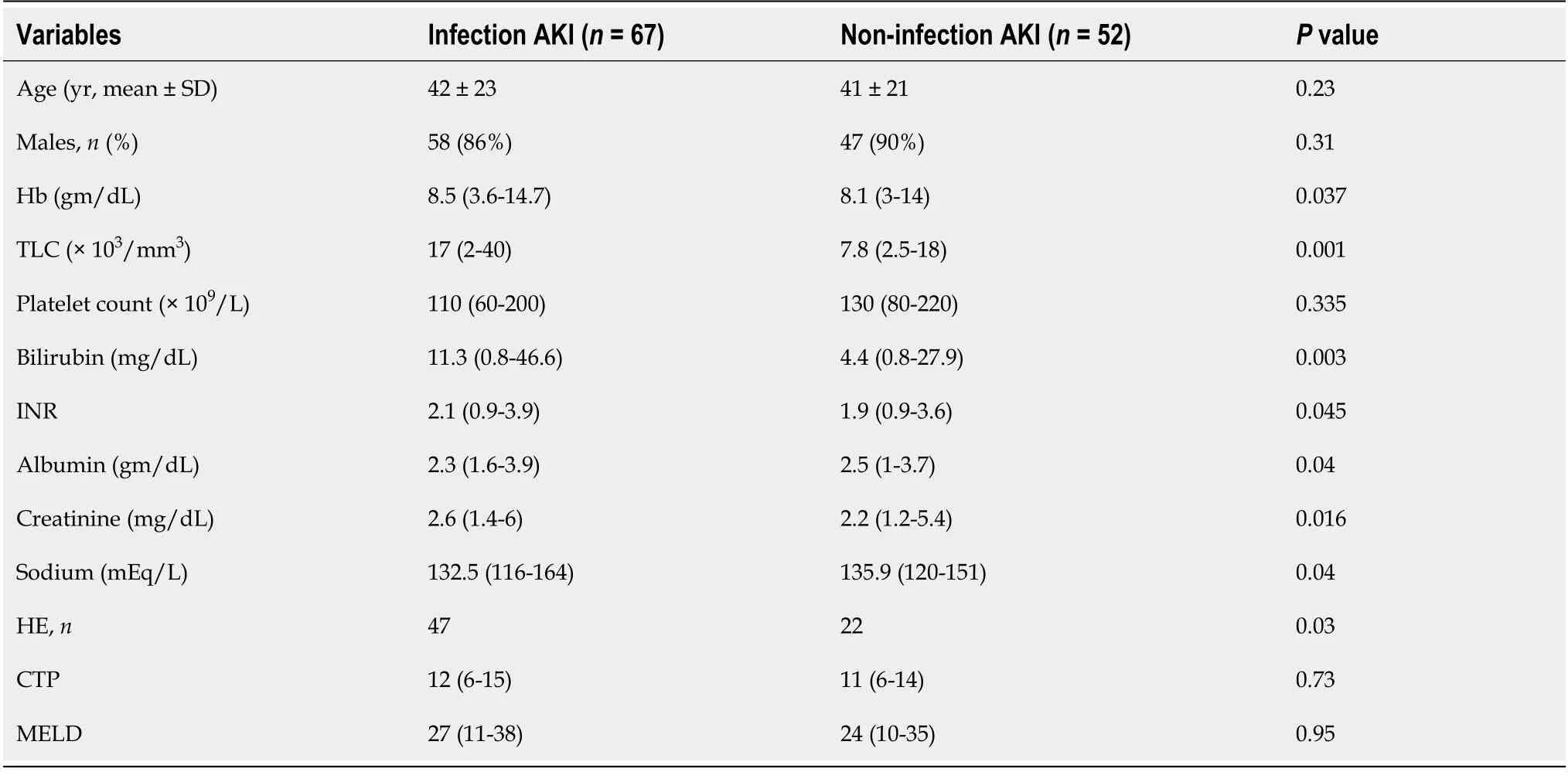
Table 1 Baseline characteristics of patients in lnfection and non-infection acute kidney injury groups

Table 2 Mortality data among infection and non-infection acute kidney injury groups

Table 3 Univariate and multivariate analysis of survivors and non-survivors at 28-d

Table 4 Univariate and multivariate analysis of survivors and non-survivors in infection acute kidney injury group(n =67)at 28-d
As per CANONIC grading of ACLF,there were 35 patients in no ACLF,23 in ACLF grade-1,27 in ACLF grade-2,34 in ACLF grade-3.At 28-d,there was mortality of one patient with no ACLF,three in ACLF grade-1,13 in ACLF grade-2,and 25 in ACLF grade-3.At 90-d,there was a mortality of five patients in no ACLF,five in ACLF grade-1,18 in ACLF grade-2,and 34 in ACLF grade-3(Figure 2).In infection AKI group(n=67),55 patients had ACLF and 12 had no ACLF.
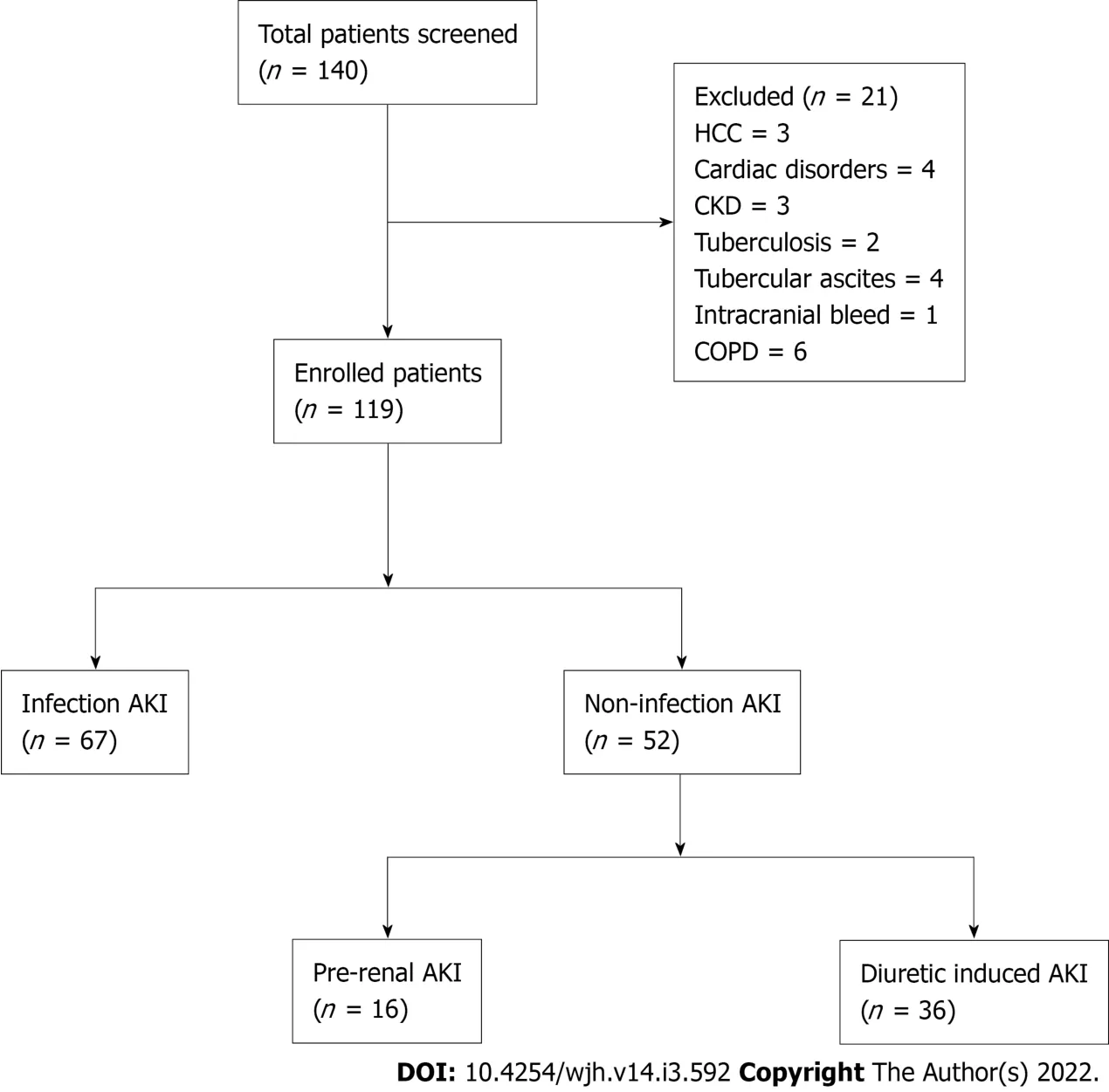
Figure 1 Flow of patients into the study.AKI:Acute kidney injury;HCC:Hepatocellular carcinoma;CKD:Chronic kidney disease.
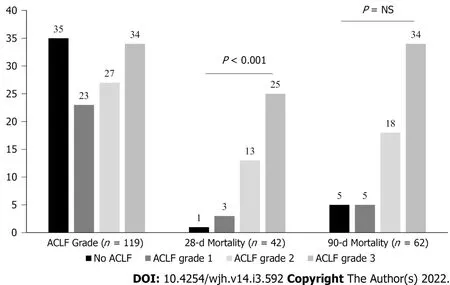
Figure 2 Distribution of acute-on-chronic liver failure grades and 28- and 90-d mortality as per acute-on-chronic liver failure grades among patients of all groups.ACLF:Acute-on-chronic liver failure.
DlSCUSSlON
The study gives three important findings in relation to infection AKI in cirrhosis of liver:(1)prevalence of infection AKI in cirrhosis;(2)One-and three-mo mortality;and(3)predictors of mortality at 28-d in infection AKI group.There was a 56% prevalence of infection AKI in patients with cirrhosis presenting with AKI.Remaining patients had AKI due to pre-renal and diuretic-related causes.This study had SBP as the cause of infection in 45% followed by pneumonia(13%)and cellulitis(10%)in acute decompensation of cirrhosis.The CANONIC series had SBP in 25% of all infections and source of infection was undefined in 13%[9].The International Club of Ascites Global Study Group also showed higher prevalence of SBP(35%vs27%)and pneumonia(28%vs19%)in Asia compared to Europe respectively[2].The Global study group showed higher rates of ACLF in Asia compared to global data(46%vs35%;P< 0.01)in patients with cirrhosis with infection respectively[10].Our study had ACLF in 82% of patients in infection AKI group.We had selectively included patients of cirrhosis with AKI and as renal dysfunction is a late manifestation in the course of cirrhosis,this may be the reason behind the higher rates of ACLF in our study population as compared to previous studies which included all patients with acute decompensation of cirrhosis.
The previous data from India suggest higher rates of acute viral hepatitis A and E as a cause for acute insult in acute decompensation of cirrhosis and ACLF[11].However,recent studies show a trend towards increasing rates of infection with multidrug resistant(MDR)and extremely drug resistant(XDR)bacteria in Asia[12].The Global study showed higher prevalence of MDR(76%vs16%)and XDR bacteria(33%vs1%-16%)in Indian centers,as compared to Western centers respectively[10].
Presence of infections in cirrhosis activates systemic inflammation and results in multi-organ dysfunction[13].The pathogen associated molecular patterns(PAMPs)arising from the gut and damage associated molecular patterns(DAMPs)released from necrotic hepatocytes stimulate toll like receptors(TLRs)on hepatocytes and cause release of Interleukin(IL)-1,IL-6,tumor necrosis factor(TNF)-alpha,etc.The cytokine storm,PAMPs and DAMPs in the circulation increase the expression of TLR4 receptors in the kidneys leading to increased permeability,proteinuria,and alteration in vascular tone.Through various molecular pathways,oxidative stress and apoptosis in tubular epithelial cells increases and results in sepsis induced AKI[14,15].In animal studies,pharmacological interventions targeting TLR receptors in the kidney have shown reduced injury in sepsis induced AKI[16].Shahet al[17]showed that there is already increased expression of TNF-alpha,TLR4,etc.in kidneys in cirrhosis,making themsusceptible to inflammatory insult and gut decontamination with norfloxacin prevents renal dysfunction after LPS stimulation.The present study revealed that 1-mo mortality in the infection AKI group was significantly higher than non-infection AKI(38vs4;P< 0.0001)respectively.It is likely that the greatest impact of infection as an acute insult is on short term mortality,and if aggressive and appropriate management is given timely,it may improve renal function also.
Various studies on histopathology of renal tissues in cirrhosis have shown direct renal damage due to high bilirubin levels.There is formation of bile casts in the tubular lumen and accumulation of conjugated bilirubin in tubular epithelial cells,which leads to mitochondrial damage with defective oxidative phosphorylation.All above changes predispose patients of cirrhosis with jaundice to cholemic nephropathy[18].Nazaret al[19]evaluated response of terlipressin in treatment of hepatorenal syndrome type-1 and found serum bilirubin level > 10 mg/dL as a predictor of poor response to therapy.The response rate in patients with bilirubin > 10 mg/dL was 13% as compared to 67% in bilirubin values < 10 mg/dL(P=0.001).We reported higher mean bilirubin values in the infection AKI group than non-infection AKI group(11.3vs4.4 mg/dL)respectively.Possibly with increasing severity of chronic liver disease as assessed by MELD score,the immune function worsens and there is propensity to get infection in these patients.Our study also revealed significantly higher serum bilirubin values(15.7vs4.2 mg/dL)in non-survivors than survivors at 28-d,respectively.
In ACLF,HE is multifactorial.Sepsis,metabolic disturbances like hypokalemia,hyponatremia secondary to diuretic use or volume loss,liver dysfunction with hyperammonemia can precipitate HE.We have shown previously that there is increasing cerebral edema in patients with increasing grades of ACLF[20].Therefore,HE also marks a poor prognosis in patients with infection AKI.
Our study has some limitations.The sample size could be higher,due to which subgroup analysis could not be done as the number of patients were small in individual groups.Second,being a tertiary care institute,most of the patients were referred from primary and secondary care centers after receiving antibiotics,therefore,culture reports were not available in all the patients.Also,the data onbeta blockers was not available at baseline for all the patients and could not be analyzed.
In ACLF,renal dysfunction is multifactorial with the presence of sepsis,circulatory dysfunction either due to volume loss or sepsis and higher bilirubin levels.We showed that pre-renal,upper GI bleed and diuretic-induced AKI is less severe with favorable outcomes after successful management with very low rate of recurrence.On the other hand,in patients with infections,it is not only the control of infection,but also the number of organ failures which is crucial to determine the final outcome of these patients.Finally,higher grades of ACLF in patients with infection,AKI having liver dysfunction and cerebral failure has worst prognosis with high 28-d mortality.
CONCLUSlON
Infections lead to worsening hemodynamics in cirrhosis which results in organ failures.Renal dysfunction in these patients further complicates the clinical scenario.We noted that higher bilirubin levels and Hepatic encephalopathy in patients with infection associated AKI portends a dismal prognosis.The present study emphasizes the worse prognosis with infection and need of early identification and aggressive management on admission to improve short-term mortality.
ARTlCLE HlGHLlGHTS
Research background
Acute kidney injury(AKI)in cirrhosis has dismal outcomes.Recent data suggests infections being most common insult for acute decompensation of cirrhosis.Infections lead to acute deterioration of already compromised hemodynamics in cirrhosis.
Research motivation
Infections in cirrhosis is a precursor towards multi-organ dysfunction.Kidney failure is one of the early manifestation in cirrhosis which has a potential for reversibility.Identifying high risk of mortality in patients with AKI in cirrhosis may warrant early institution of treatment,especially in presence of infection.This may help to develop new protocols to salvage kidney in presence of infections in cirrhosis.
Research objectives
To compare infection and non-infection AKI in cirrhosis,and to determine predictors of mortality at 28-d in patients with infection associated AKI.
Research methods
It was a prospective,observational study conducted at a tertiary care hospital for a period of 1 year.After written,informed consent total 119 patients with AKI in cirrhosis were included into the study.AKI was defined as per International Club of Ascites-AKI 2015 criteria.Patients were divided into infection and non-infection AKI groups.Non-infection AKI included patients with pre-renal and diuretic induced AKI.Infection and non-infection AKI groups were compared for clinical and laboratory data.In infection AKI group logistic regression analysis was performed to determine 28-d predictors of mortality.
Research results
There were 119 patients of cirrhosis with AKI.Alcohol(n=104)was most common etiology of cirrhosis.The infection AKI group had 67(56%)patients and non-infection AKI had 52(44%)patients which included pre-renal AKI in 36(30%)and diuretic-induced AKI in 16(14%).Infection AKI patients had higher progression of AKI(19/67vs2/52;P=0.01)and 28-d mortality(38/67vs4/5;P≤ 0.01)as compared to non-infection AKI patients.On subgroup analysis of Infection AKI group,on multivariate analysis,serum bilirubin as well as presence of HE were independent predictors of 28-d mortality.There was no significant difference of mortality at 90-d between two groups.
Research conclusions
This study says that AKI in cirrhosis with infection has high short term mortality.High bilirubin and presence of hepatic encephalopathy predicts high 28-d mortality in infection associated AKI.Probably AKI in patients with cirrhosis is multifactorial with sepsis,volume depletion,bilirubin as important factors.
Research perspectives
High bilirubin levels can contribute to nephropathy as well as encephalopathy.Still,we do not have effective therapies for high bilirubin values.Future research should focus on drugs to lower bilirubin levels.And probably more data is needed on infections in cirrhosis.
ACKNOWLEDGEMENTS
We thank Prof Rakesh Mittal,Department of Pharmacology,Pt B D Sharma Institute of Medical Sciences for reviewing outcomes of statistical analysis.
FOOTNOTES
Author contributions:Gupta T was the guarantor and designed the study;Ranga N was involved in acquisition of data and drafted the initial manuscript;Goyal SK performed statistical analysis and interpretation of data;Gupta T revised the manuscript critically for important intellectual content.
lnstitutional review board statement:The study was reviewed and approved by the institutional ethics committee at Pt.BD Sharma Institute of Medical Sciences,Rohtak(India).
lnformed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:There are no conflicts of interest to report.
Data sharing statement:No additional data are available.
STROBE statement:The authors have read the STROBE Statement—checklist of items,and the manuscript was prepared according to the STROBE Statement—checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:India
ORClD number:Tarana Gupta 0000-0003-3453-2040;Naveen Ranga 0000-0002-1697-8252;Sandeep Kumar Goyal 0000-0002-9113-7664.
S-Editor:Chang KL
L-Editor:Filipodia
P-Editor:Chang KL
杂志排行

World Journal of Hepatology的其它文章
- Hepatitis E in immunocompromised individuals
- Small duct primary sclerosing cholangitis:A discrete variant or a bridge to large duct disease,a practical review
- New progress in understanding roles of nitric oxide during hepatic ischemia-reperfusion injury
- Renal manifestations of hepatitis E among immunocompetent and solid organ transplant recipients
- Safety of direct acting antiviral treatment for hepatitis C in oncologic setting:A clinical experience and a literature review
- Fertaric acid amends bisphenol A-induced toxicity,DNA breakdown,and histopathological changes in the liver,kidney,and testis