Risk factors and prediction of acute kidney injury after liver transplantation:Logistic regression and artificial neural network approaches
2022-04-02LuisCesarBredtLuisAlbertoBatistaPeresMichelRissoLeandroCavalcantideAlbuquerqueLeiteBarros
Luis Cesar Bredt,Luis Alberto Batista Peres,Michel Risso,Leandro Cavalcanti de Albuquerque Leite Barros
Luis Cesar Bredt,Department of Surgical Oncology and Hepatobilary Surgery,Unioeste,Cascavel 85819-110,Paraná,Brazil
Luis Alberto Batista Peres,Department of Nephrology,Unioeste,Cascavel 85819-110,Paraná,Brazil
Michel Risso,Department of Internal Medicine,Assis Gurgacz University,Cascavel 85000,Paraná,Brazil
Leandro Cavalcanti de Albuquerque Leite Barros,Department of Hepatobiliary Surgery,Unioeste,Cascavel 85819-110,Paraná,Brazil
Abstract BACKGROUND Acute kidney injury(AKI)has serious consequences on the prognosis of patients undergoing liver transplantation.Recently,artificial neural network(ANN)was reported to have better predictive ability than the classical logistic regression(LR)for this postoperative outcome.AIM To identify the risk factors of AKI after deceased-donor liver transplantation(DDLT)and compare the prediction performance of ANN with that of LR for this complication.METHODS Adult patients with no evidence of end-stage kidney dysfunction(KD)who underwent the first DDLT according to model for end-stage liver disease(MELD)score allocation system was evaluated.AKI was defined according to the International Club of Ascites criteria,and potential predictors of postoperative AKI were identified by LR.The prediction performance of both ANN and LR was tested.RESULTS The incidence of AKI was 60.6%(n=88/145)and the following predictors were identified by LR:MELD score > 25(odds ratio[OR]=1.999),preoperative kidney dysfunction(OR=1.279),extended criteria donors(OR=1.191),intraoperative arterial hypotension(OR=1.935),intraoperative massive blood transfusion(MBT)(OR=1.830),and postoperative serum lactate(SL)(OR=2.001).The area under the receiver-operating characteristic curve was best for ANN(0.81,95%confidence interval[CI]:0.75-0.83)than for LR(0.71,95%CI:0.67-0.76).The root-mean-square error and mean absolute error in the ANN model were 0.47 and 0.38,respectively.CONCLUSION The severity of liver disease,pre-existing kidney dysfunction,marginal grafts,hemodynamic instability,MBT,and SL are predictors of postoperative AKI,and ANN has better prediction performance than LR in this scenario.
Key Words:Logistic regression;Liver transplantation;Acute kidney injury;Machine learning;Artificial neural network
lNTRODUCTlON
Among the possible complications of complex abdominal and liver procedures,acute kidney injury(AKI)should be considered a major cause of postoperative morbidity and mortality[1-6].Updated data report a 0.9%-17.9% incidence of AKI after liver resection[7-9],and 4%-94% after LT[10,11],either livingdonor(LDLT)or deceased-donor LT(DDLT).Although there is a lack of a reported standard definition of postoperative AKI[12]after DDLT,it is of fundamental importance to identify patients at risk for AKI after LT,ideally by the set of preoperative clinical evaluation,as well as by the complementary information of the intraoperative period,thus enabling the adoption of preventive measures or early therapies for AKI in the postoperative period.
There are many studies available based on deep learning models for different clinical purposes in distinct fields of medicine,such as for complex imaging acquisition and processing[13-17],and artificial neural network(ANN)as a deep learning modality is commonly used to solve complex problems,where the behavior of variables is not rigorously known.In the specific field of AKI after LT,along with other machine learning techniques(gradient boosting machine,random forest,decision tree,support vector machine,naïve Bayes,and deep belief network),ANN has already been compared to multivariable logistic regression(LR)regarding their prediction performance[18].We hypothesized that ANN would be a feasible alternative with higher performance than the classic LR model,reinforcing the wide applicability of ANN and its ability to learn from input data with or without supervision.
The multifactorial origin of AKI after LT makes it complex to predict which candidate for the procedure has an increased risk of this complication,and in the face of this complexity,along with the classical LR,ANN would be a very reliable prognostic tool for AKI risk assessment,where the relative risk term is parameterized by an ANN instead of regression,enabling the application of deep learning,whereas comparative studies evaluating such a promising tool for predicting AKI following LT are scarce[19-20].
In face of this serious postoperative complication,this retrospective study of patients who underwent only-first DDLT aimed to identify the risk factors for postoperative AKI and compare the prediction performance of ANN with that of LR for this complication.
MATERlALS AND METHODS
Study design
A retrospective study was conducted on patients of both sexes,aged > 18 yr,diagnosed with liver cirrhosis and portal hypertension(platelets < 100000/mm3,splenomegaly and/or esophageal varices),eventually associated with hepatocellular carcinoma(HCC),and undergoing the first DDLT at a tertiary referral hospital between September 2017 and June 2021.The patients were allocated according to Model for End-Stage Liver Disease(MELD)score,with no evidence of end-stage kidney disease.The MELD score was dichotomized at 25 points for statistical purposes according to Romanoet al[21],and the minimum hospital stay was 7 d according to Wonget al[22]and the International Club of Ascites(ICA)definitions for the onset of AKI[23].
Renal dysfunction definitions
Kidney dysfunction(KD)subtypes were defined according to Wonget al[22](Table 1)and the ICA definitions(Table 2)[23],and both the acute deterioration of renal function and the background CKD could be structural or functional in nature,including hepatorenal syndrome(HRS)types 1 and 2(Table 3)[23].Estimated glomerular filtration rate(eGFR)was calculated by the Modified Diet in Renal Disease 6(MDRD6)formula:eGFR=198 ×[serum creatinine(mg/dL)-0.858× age-0.167× 0.822 if patient is female × 1.178 if patient is black]×[serum urea nitrogen concentration(mg/dL)]-0.293×[urine urea nitrogen excretion(g/d)]0.249[3].

Table 1 Diagnostic criteria for kidney dysfunction in cirrhosis(Wong et al[22],2011)

Table 2 Definition and classification of acute kidney injury for patients with liver cirrhosis according to the lnternational Club of Ascites(Angeli et al[23],2015)

Table 3 Diagnostic criteria and hepatorenal syndrome subtypes(Angeli et al[23],2015)

Table 4 Acute kidney injury stages according to lnternational Club of Ascites criteria(n=145)
Graft definitions
Marginal liver grafts of extended criteria donor(ECD)were defined as grafts with three or more of the following donor features:> 60 yr,body mass index(BMI)> 27-30 kg/m2,macrovesicular steatosis >30%,intensive care unit(ICU)stay > 4 d,sustained arterial hypotension > 1 h,cold ischemia times(CIT)> 8 h,warm ischemia times(WIT)> 40-45 min,controlled sepsis,history of alcoholism,serum creatinine> 1.2 mg/dL,arterial hypotensive episodes < 60 mmHg for > 1 h,bilirubin > 2.0 mg/dL,alanine transaminase(ALT)> 170 U/L and aspartate transaminase(AST)> 140 U/L,the use of dopamine doses > 10 microg/kg per min,and peak serum sodium > 155 mEq/L[24-26].
Routine biopsy was performed on the donor allograft for all patients included in the study.Liver specimens were evaluated by hematoxylin and eosin staining using either frozen or permanent section.Macrovesicular steatosis was defined as a single vacuole larger than the nucleus,replacing most of the hepatocyte cytoplasm and displacing the nucleus to the cell membrane[27].Macrosteatosis was categorized as no steatosis(< 5%),mild steatosis(10%-29%),moderate steatosis(30%-60%),and severe steatosis(> 60%)[28].
Hemodynamic status and monitoring
Fluid administration consisted of a baseline infusion of a balanced crystalloid(Plasmalyte,Baxter,Belgium)with or without 4% albumin(depending on patient conditions).Rapid infusers,perfusion heaters,and a Cell Saver(Haemonetics,Massachusetts,EUA)for blood recovery were ready for use prior to induction.In accordance to American Society of Anaesthesiologists(ASA)guidelines,Cell Saver has effectiveness in reducing the volume of allogeneic blood transfused[29].
A Flow Trac/EV1000 System(Edwards Lifesciences,Irvine,USA)was inserted and hemodynamic interventions were guided using continuous cardiac index(CCI),stroke volume index(SVI),mixed venous oxygen saturation(SvO2),central venous pressure(CVP),and mean arterial pressure(MAP).Fluids were administered if SVI was < 30 mL/m2and/or CCI < 2 L/min/m2for compensation for blood lossvia250-500 mL fluid boluses of Plasmalyte,to strictly maintain MAP > 65 mmHg,avoiding hemodynamic instability as described elsewhere[30,31].
Blood loss monitoring consisted of visual assessment of the surgical field,including the extent of blood present,presence of microvascular bleeding,surgical sponges,clot size and shape,and volume in suction canister.In case of active hemorrhage,blood product administration was guided by using rotational thromboelastometry monitoringviaROTEM(Tem Innovations GmbH,Munich,Germany),hemoglobin/hematocrit monitoring,coagulation tests(international normalized ratio[INR]),activated partial thromboplastin time[aPTT],fibrinogen concentration[normal range:200 to 400 mg/dL],and platelet count[29].Whereas there is no clear evidence that ROTEM improved survival in LT patients,it was effective in reducing bleeding and fewer patients required both platelets and fresh frozen plasma(FFP)transfusion[32].Monitoring for perfusion of vital organs included standard ASA monitoring,renal monitoring(urine output),and analysis of arterial blood gases and serum(SL)level(cutoff of 2.0 mmol/L)[29].
Massive blood transfusion(MBT)protocol for avoidance of dilutional coagulopathy was activated when hemorrhage was expected to be massive(anticipated need to replace 50% or more of blood volume within 2 h),or bleeding continued after the transfusion of 4 units of packed red blood cells(PRBC)within a short period of time(1-2 h),or systolic blood pressure(SBP)was below 90 mmHg and heart rate was above 120 beats per minute in the presence of uncontrolled bleeding[33].According to the Pragmatic Randomized Optimal Platelet and Plasma Ratios(PROPPR)study group recommendations,blood transfusion of RBC,fresh frozen plasma(FFP),and platelets were at a 1:1:1 ratio[34].
Postreperfusion(PRS)was defined as a decrease in MAP > 30% below the baseline value,for at least 1 min,occurring during the first 5 min after reperfusion of the liver graft,asystole,or hemodynamically significant arrhythmias,or the need to start the infusion of vasopressors during the postreperfusion period[35].Intraoperative arterial hypotension(IOAH)was defined as MAP less than 65-60 mmHg for at least 5 min,or any exposure to MAP less than 55-50 mmHg[31],irrespective of the cause:Prolonged surgery time,massive bleeding,PRS,and/or hemodynamic instability because of end-stage liver disease.
Statistical analysis
The baseline characteristics of the patients are expressed in absolute values,the mean ± SD,and percentages,when appropriate.The comparison between groups was performed for continuous variables using the Kruskal-Wallis test and the Mann-Whitney test.The assumptions were made to perform or not the parametric tests,and the categorical variables were compared using the chi-square test.Independent variables with significance in the univariate model was selected for the bootstrap classical LR model to assess the effect of bivariate independent variables(graft quality,patients characteristics,and intraoperative events)on the incidence of postoperative AKI.The results of the model are expressed by odds ratio(OR),together with the corresponding 95% confidence intervals[CIs],Nagelkerke R2 statistic,and Hosmer and Lemeshow goodness of fit test.Pvalues < 0.05 were considered significant.A relationship map between the significant variables in the LR model was alsoconstructed.
The explanatory variables selected in the LR model were used for the ANN machine learning.Before developing prediction models,our collected data were divided into 70% of training dataset cases and 30% of test dataset cases.The cases in the training dataset were used for developing machine learning models.The ANN method had its own hyperparameters(number of layers in multilayer perceptron ANN),with a 10-fold cross-validation.This cross-validation process was used for developing the model,and performance was evaluated.The activation function of the hidden layer was made by hyperbolic tangent activation function,and Softmax for the output layer.All possible combinations of hyperparameters were investigated,and the hyperparameters with the highest average validation AUROC(area under the receiver-operating characteristic curve)were considered as optimal hyperparameters,and after that,the final model was tested for performance by root-mean-square error(RMSE)and mean absolute error(MAE)calculation.The importance of variables for the model was calculated.ANN structural model was constructed according to Haykin[36].
Our primary analysis attempted to analyze the prediction ability of machine learning and LR model in terms of AUROC.Accuracy was defined as the sum of the number of cases with true positive and true negative results divided by the total number of test sets.Statistical calculations were performed using the SPSS 28.0 software for Windows.
RESULTS
During the period from September 2017 to June 2021,145 DDLT cases were included in the present study.Of the total patients included,88(60.6%)presented any further stage of postoperative AKI during the 7-d follow-up,22(15.1%)developed stage 1 AKI,36(24.8%)developed stage 2,and 30(20.6%)developed stage 3 AKI(Table 4);renal replacement therapy(RRT)was required in 12 patients(8.7%).All patients’ preoperative baseline information,donors,and grafts characteristics according to the occurrence of AKI are shown in Tables 5 and 6.The intraoperative data related to IOAH,blood derivatives transfusion,and piggy-back clamping,and laboratorial tests until the seventh postoperative(PO)day are shown in Table 7.
In the LR analysis,Nagelkerke R2 statistic was 0.147.Hosmer and Lemeshow goodness of fit test was not significant at 5%(P=0.247).The six following factors were confirmed as predictors(Table 8):Biological(not adjusted)MELD score ≥ 25(OR=1.999,95%CI=1.586-2.503,P <0.001),pre-existing KD(OR=1.279,95%CI=0.916-1.686,P <0.001),ECD(OR=1.191,95%CI=0.711-1.787,P=0.002),IOAH(OR=1.935,95%CI=1.505-2.344,P <0.001),MBT(OR=1.830,95%CI=1.428-2.241,P <0.001),serum lactate at the end of LT(OR=2.001,95%CI=1.616-2.421,P <0.001).The relationships between the significant variables were explored by a relationship map detailed in Figure 1.

Table 5 Patients’ preoperative baseline information according to the occurrence of acute kidney injury after deceased-donor liver transplantation(n =145)

Table 6 Donor and graft characteristics according to the occurrence of acute kidney injury after deceased-donor liver transplantation(n=145)

Table 7 lntraoperative events in 145 deceased-donor liver transplantations according to the occurrence of postoperative acute kidney injury

Table 8 Logistic regression analysis of risk factors for acute kidney injury after deceased-donor liver transplantation(n=145)
Data of the two models with regard to AUROC for predicting AKI of all stages are detailed in Figure 2.ANN had the largest test AUROC(0.81,95%CI:0.75-0.83)and highest accuracy(0.68)than LR analysis[AUROC(0.71,95%CI:0.67 to 0.76),accuracy=0.68].
Importance plot for ANN is shown in Figure 3(KD and MELD score ranked first and second,respectively).Multilayer perceptron ANN presented one hidden layer by hyperbolic tangent activation function with four nodes in the layer,as presented in the ANN structural model diagram(Figure 4),and the prediction RMSE was 0.47 and the prediction MAE was 0.38.

Figure 1 Relationship map between the selected variables in the logistic regression for acute kidney injury after deceased-donor liver transplantation(n=145).MELD:Model for End-stage Liver Disease;KD:Kidney dysfunction;ECD:Extended criteria donor;IOAH:Intra-operative arterial hypotension;MBT:Massive blood transfusion;SL:Serum lactate.LR:Logistic regression;AKI:Acute kidney injury.

Figure 2 Area under the receiver-operating characteristic curve of the two different models for predicting acute kidney injury(n=145).LR:Logistic regression;AUROC:Area under the receiver-operating characteristic curve;ANN:Artificial neural network;AKI:Acute kidney injury.

Figure 3 Variance importance plot of predictors of acute kidney injury for artificial neural network.KD:Kidney dysfunction;MELD:Model for Endstage Liver Disease;IOAH:Intra-operative arterial hypotension;MBT:Massive blood transfusion;ECD:Extended criteria donor;AKI:Acute kidney injury;ANN:Artificial neural network.
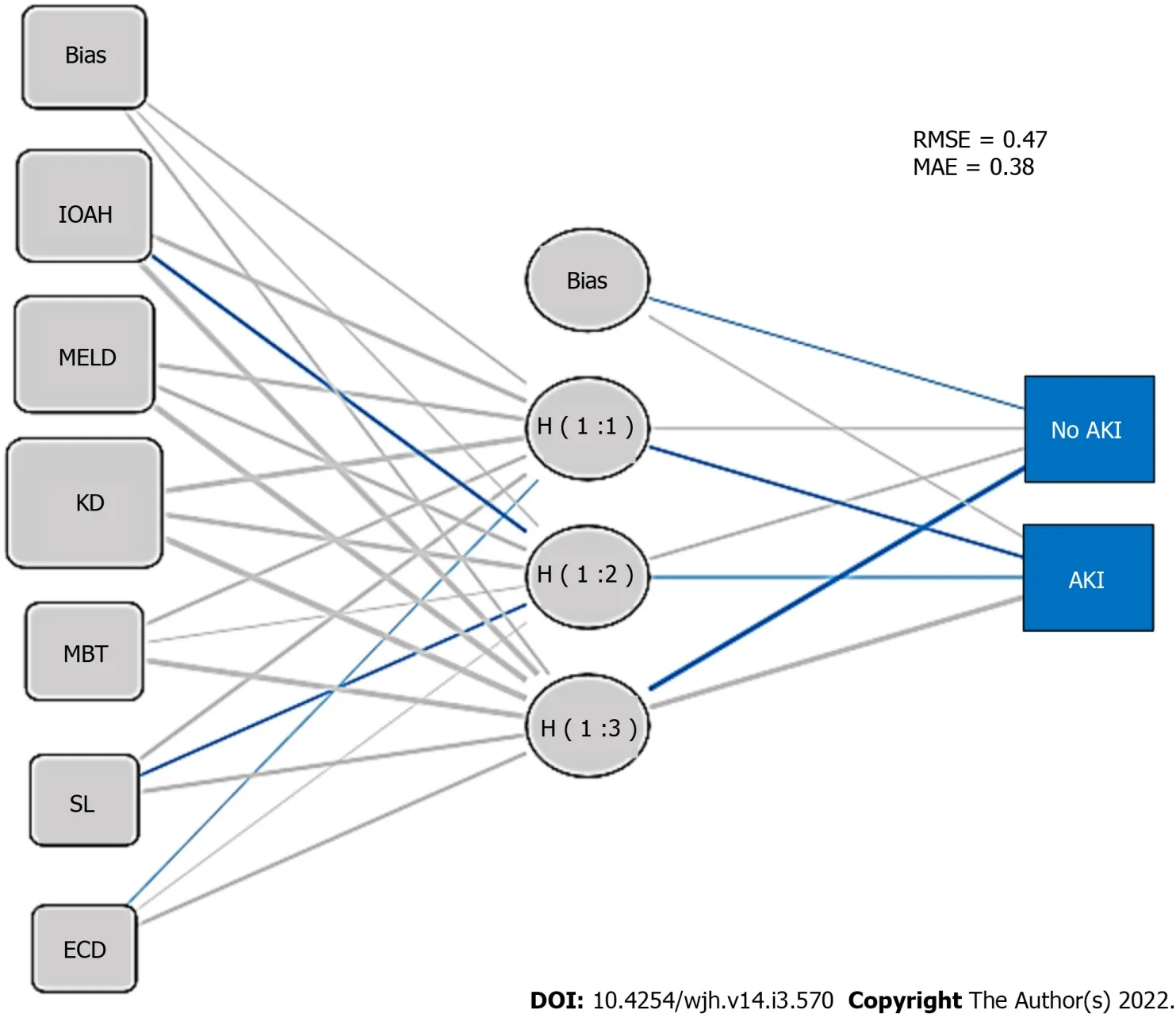
Figure 4 Artificial neural network structural model diagram for acute kidney injury after deceased-donor liver transplantation.IOAH:Intraoperative arterial hypotension;MELD:Model for End-stage Liver Disease;KD:Kidney dysfunction;MBT:Massive blood transfusion;ECD:Extended criteria donor;AKI:Acute kidney injury;ANN:Artificial neural network;RMSE:Root-mean-square error;MAE:Mean absolute error.
DlSCUSSlON
As described elsewhere[36],the findings in the present study demonstrated a high incidence of postoperative AKI,and the predictive ability of ANN and LR models for this complication.An important point in this research is that AKI prediction was focused on the identification of significant risk factors at the end of the procedure,thus enabling the adoption of preventive measures or early therapies for AKI in the postoperative period.
In the present study,the severity of chronic liver disease,pre-existing KD,marginal grafts,hemodynamic instability,MBT,and consequent inadequate tissue perfusion during LT were predictors of AKI after DDLT,and the relationship map illustrated through a visual pattern,the relationshipbetween the variables,although it is important to understand that a visual relationship does not always mean statistical causation.As demonstrated in our study,in the case of machine learning-based techniques,the importance of each variable in the dataset can be indicated by the characteristic importance measure,which can improve the transparency of the algorithm according to Heet al[20].
According to our results,ANN had larger AUROC and higher accuracy to predict AKI after DDLT than LR,which is consistent with the previous study with different machine learning tools,whereas the performance of the ANN was inferior to that of all other machine learning techniques in prediction of AKI after LT[19].Multilayer perceptron has already been associated to a good performance in predicting in-hospital mortality,reinforcing the good performance of ANN to predict clinical outcomes,although there have been some reports that the performance of the machine learning techniques is not superior to that of LR model in predicting mortality[18].
Regarding the risk factors identified in the present research,several other authors have already described that higher MELD scores[37]were associated with AKI after LT[20,38].Xuet al[21]showed that MELD score > 25 was a predictor of AKI,and in patients with MELD scores > 30,the most required RRT[11,39].Moreover,in the cirrhosis scenario,the functional renal disorders can be added as risk factors for AKI,such as recipient HRS[11,23,40].Donor marginal liver grafts of ECD were identified elsewhere as a strong predictor of PGD[24-26]and post-LT AKI[20].Patients undergoing LT can experience IOAH and consequent AKI because of multiple factors,including the duration of surgery,massive bleeding[16,40-42],the severity of the PRS[36,43,44],and the severity of the end-stage liver disease[21,45-49].In addition,MBT may be an additional risk factor for postoperative AKI[34,49,50].
The present retrospective study has important limitations,regarding sample size and moreover,the lack of evaluation of clinical outcomes of patients according to the occurrence of post-LT AKI,either for short or long-term evolution of patients.Despite these limitations,the high incidence of AKI reported highlights the importance of this issue,and the predictors identified may provide a focus for further research.ANN methods may provide feasible tools for forecasting AKI after LT,and perhaps provide a high-performance predictive model that may ultimately improve perioperative management of these patients at risk for this serious complication.
CONCLUSlON
According to our results,the severity of chronic liver disease,pre-existing KD,marginal grafts,hemodynamic instability,MBT,and inadequate tissue perfusion during LT are predictors of AKI after
DDLT,and ANN has better prediction performance than LR in this scenario.
ARTlCLE HlGHLlGHTS
Research background
Acute kidney injury(AKI)post-liver transplantation(LT)is a serious complication,and its prediction with validated tools is crucial.
Research motivation
To improve the perioperative management of patient candidates for LT.
Research objectives
To identify the risk factors for AKI after deceased-donor liver transplantation(DDLT)and validate a prediction tool for this complication.
Research methods
Logistic regression(LR)analysis for predictor identification,and comparative analysis of artificial neural network(ANN)and LR prediction performance were performed.
Research results
The severity of liver disease,preexisting kidney dysfunction,marginal grafts,hemodynamic instability,massive blood transfusion,and SL were predictors of postoperative AKI,and ANN had better prediction performance than LR.
Research conclusions
ANN has better performance than the classical LR for AKI prediction after DDLT.
Research perspectives
A risk score of AKI after DDLT can be developed according to these identified predictors.
FOOTNOTES
Author contributions:Bredt LC,Peres LAB,Risso M,and Barros LCAL contributed equally to this study with regard to conception and design,literature review and analysis,manuscript drafting,critical revision,and editing,and approval of the final version.
lnstitutional review board statement:The study was approved by the Research Ethics Board at Assis Gurgacz University(No.4.190.165).The study was performed according to the ethical guidelines of the 1975 Declaration of Helsinki.
Conflict-of-interest statement:All authors that contributed equally to this manuscript declare no potential conflicts of interest and no financial support.
Data sharing statement:All authors declare that the original anonymous dataset is available on request from the corresponding author(lcbredt@gmail.com).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution Noncommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Brazil
ORClD number:Luis Cesar Bredt 0000-0002-8487-1790;Luis Alberto Batista Peres 0000-0001-5863-6720;Michel Risso 0000-0002-3268-0392;Leandro Cavalcanti de Albuquerque Leite Barros 0000-0003-1704-6868.
S-Editor:Wang LL
L-Editor:Wang TQ
P-Editor:Wang LL
杂志排行

World Journal of Hepatology的其它文章
- Hepatitis E in immunocompromised individuals
- Small duct primary sclerosing cholangitis:A discrete variant or a bridge to large duct disease,a practical review
- New progress in understanding roles of nitric oxide during hepatic ischemia-reperfusion injury
- Renal manifestations of hepatitis E among immunocompetent and solid organ transplant recipients
- Safety of direct acting antiviral treatment for hepatitis C in oncologic setting:A clinical experience and a literature review
- Fertaric acid amends bisphenol A-induced toxicity,DNA breakdown,and histopathological changes in the liver,kidney,and testis