Drug-induced stuttering:A comprehensive literature review
2022-04-01NaemehNikvarzSaleheSabouri
Naemeh Nikvarz,Salehe Sabouri
Naemeh Nikvarz,Department of Clinical Pharmacy,Faculty of Pharmacy,Kerman University of Medical Sciences,Kerman 7616911319,Iran
Salehe Sabouri,Neuroscience Research Center,Institute of Neuropharmacology,Kerman 7616911319,Iran
Salehe Sabouri,Department of Pharmaceutical Biotechnology,Kerman University of Medical Sciences,Kerman 7616911319,Iran
Abstract Drug-induced stuttering (DIS) is a type of neurogenic stuttering (NS).Although DIS has not been reported as frequently as other cases of NS in the literature,it is not a negligible adverse drug reaction (ADR) which can significantly affect the quality of life if not treated.This literature review aims to evaluate the epidemiological and clinical characteristics of DIS and suggests some pathophysiological mechanisms for this ADR.Relevant English-language reports in Google Scholar,PubMed,Web of Science,and Scopus were identified and assessed without time restriction.Finally,a total of 62 reports were included.Twenty-seven drugs caused 86 episodes of stuttering in 82 cases.The most episodes of DIS were related to antipsychotic drugs (57%),mostly including clozapine,followed by central nervous system agents (11.6%) and anticonvulsant drugs (9.3%).The majority of the cases were male and between the ages of 31 and 40 years.Repetitions were the most frequent core manifestations of DIS.In 55.8% of the episodes of DIS,the offending drug was withdrawn to manage stuttering,which resulted in significant improvement or complete relief of stuttering in all cases.Based on the suggested pathophysiological mechanisms for developmental stuttering and neurotransmitters dysfunctions involved in speech dysfluency,it seems that the abnormalities of several neurotransmitters,especially dopamine and glutamate,in different circuits and areas of the brain,including cortico-basal ganglia-thalamocortical loop and white matter fiber tracts,may be engaged in the pathogenesis of DIS.
Key Words:Drug;Dysfluency;Dysphemia;Psychotropics;Speech;Stammering
lNTRODUCTlON
Speech production is a complex process involving various areas of the brain.Stuttering is a fluency disorder classified as developmental or acquired stuttering.Developmental stuttering,which is mentioned as childhood-onset fluency disorder in the diagnostic and statistical manual of mental disorders,fifth edition[1],often manifests between the ages of 2 and 6 years and spontaneously remits in most cases[2,3].Acquired stuttering which has a secondary cause can occur in both children and adults.There are two types of acquired stuttering,psychogenic and neurogenic stuttering (NS).NS is caused by the traumatic brain injury,stroke,neurodegenerative disorders like Parkinson’s disease (PD) and multiple sclerosis,seizure disorders,drugs,etc.[4].In contrast to the other cases of NS,in which injuries to the brain areas involved in the speech production result in neuroanatomical and neurochemical abnormalities leading to stuttering,in the cases of drug-induced stuttering (DIS),short intervals between the initiation of culprit drug and the occurrence of stuttering and also between the dose reduction or discontinuation of the drug and the relief of stuttering suggest that DIS may be caused merely by neurochemical changes in the brain[5].
Although DIS has not been reported as frequently as other cases of NS in the literature,it is not a rare and negligible adverse drug reaction as Trenqueet al[6] have reported that 724 individual case safety reports (ICSRs) containing the lowest level terms “stuttering” or “stutter” have been registered in Vigibase,the world health organization international pharmacovigilance database,up to May 31,2020.The aim of this review is to describe the reported cases of DIS,including their demographic characteristics,medical history,predominant manifestations of stuttering,and the interventions done to manage stuttering and propose some probable pathophysiological mechanisms of this type of NS.
SEARCH STRATEGY
The electronic databases Google Scholar,PubMed,Web of Science,and Scopus were searched by two reviewers without time limitation to find the relevant data.The keywords “stutter”,“stuttering”,“speech dysfluency”,“drug-induced stuttering”,“medication-induced stuttering”,“psychotropics”“antipsychotics”,“antiepileptics”,“antiseizure drug”,“anticonvulsants”,“antidepressants”,“clozapine”,and “mood stabilizers” were used as search terms.The references of published articles were also examined to find any additional relevant reports.Case reports and case series were included.The reports whose full texts were not available and those being written in non-English language were excluded.According to the above-mentioned inclusion and exclusion criteria,63 articles reporting DIS in 82 cases were considered in this review.
Twenty-seven drugs caused 86 episodes of stuttering in 82 cases.In four cases,two drugs caused stuttering[8-11].Of 86 episodes of DIS,49 (57%) were caused by antipsychotic drugs,followed by 10(11.6%) by central nervous system (CNS) agents and 8 (9.3%) by anticonvulsant drugs (Table 1).As mentioned above,Trenqueet al[6] have done a disproportionality analysis using reports registered in Vigibase to estimate the association between exposure to a drug and occurrence of stuttering.Of 22632669 reports registered in this database,724 ICSRs contained the lowest level term “stuttering” or“stutter”.Consistent with our findings,the most reports of stuttering were related to clozapine (n=40),pregabalin (n=33) methylphenidate (n=27),adalimumab (n=26),and olanzapine (n=25)[6].The results of the disproportionality analysis done by Trenqueet al[6] showed that the following drugs had the highest reported odds ratio:Methylphenidate (19.57;95%CI:13.3-28.7);topiramate (12.48;95%CI:7.1-22.1);olanzapine (11.98;95%CI:8-17.9);golimumab (10.25;95%CI:5.5-19.1);clozapine (8.44;95%CI:6.1-11.6);and pregabalin (8.36;95%CI:5.9-11.9).
DEMOGRAPHlC CHARACTERlSTlCS OF THE PATlENTS
Twenty-eight (34.6%) cases were female.Most patients were in the age range of 31 to 40 years.Fifteen cases were less than 12 years old.Gender and age of a patient were not reported in one case report[12](Table 2).
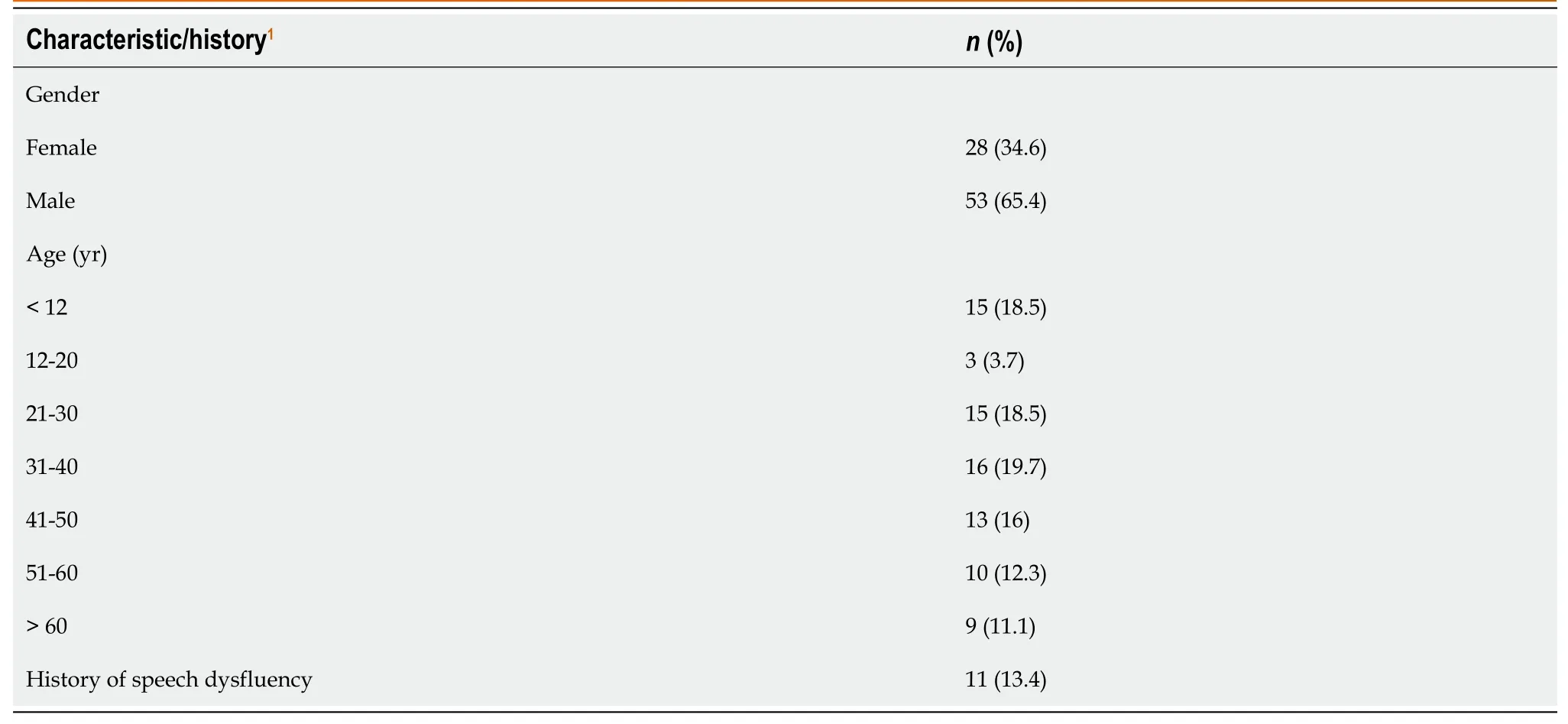
Table 2 Demographic characteristics and clinical history of patients
MANlFESTATlONS OF STUTTERlNG
The primary or core behaviors of stuttering include sound,syllables,and monosyllabic whole-word repetitions,sound prolongations,and speech blocks[4].The core behaviors were described only in 40 cases.Repetitions (n=42) were the most frequent primary behavior,followed by blockages (n=21) and sound prolongations (n=16).Twenty-one cases had more than one type of primary behavior (Table 3).
Individuals with developmental stuttering and persistent developmental stuttering (PDS) have anxiety related to stuttering[4].However,patients with acquired stuttering may be annoyed by stuttering but do not experience anxiety.None of the reports included in this review described the psychological presentations of patients when producing a dysfluent speech.
Individuals with developmental stuttering[4,13] as well as patients with NS[13-15] often develop secondary behaviors including eye blinking,facial grimacing,interjections,word or phrase substitution,etc.The secondary behaviors are acts that are learnt in long term to cope with stuttering[13].In the cases included in the present review,the secondary behaviors related to the stuttering were not reported.It may not be unusual because in comparison to the developmental stuttering,secondary behaviors are less prominent in the acquired stuttering[13].Furthermore,we believe that since the development of the secondary behaviors requires a sufficient period,it is unlikely that patients with DIS have enough time to present these behaviors because interventions such as dose reduction or discontinuation of the culprit drug are carried out as soon as possible,which result in the complete relief or significant improvement of stuttering.
MANAGEMENT
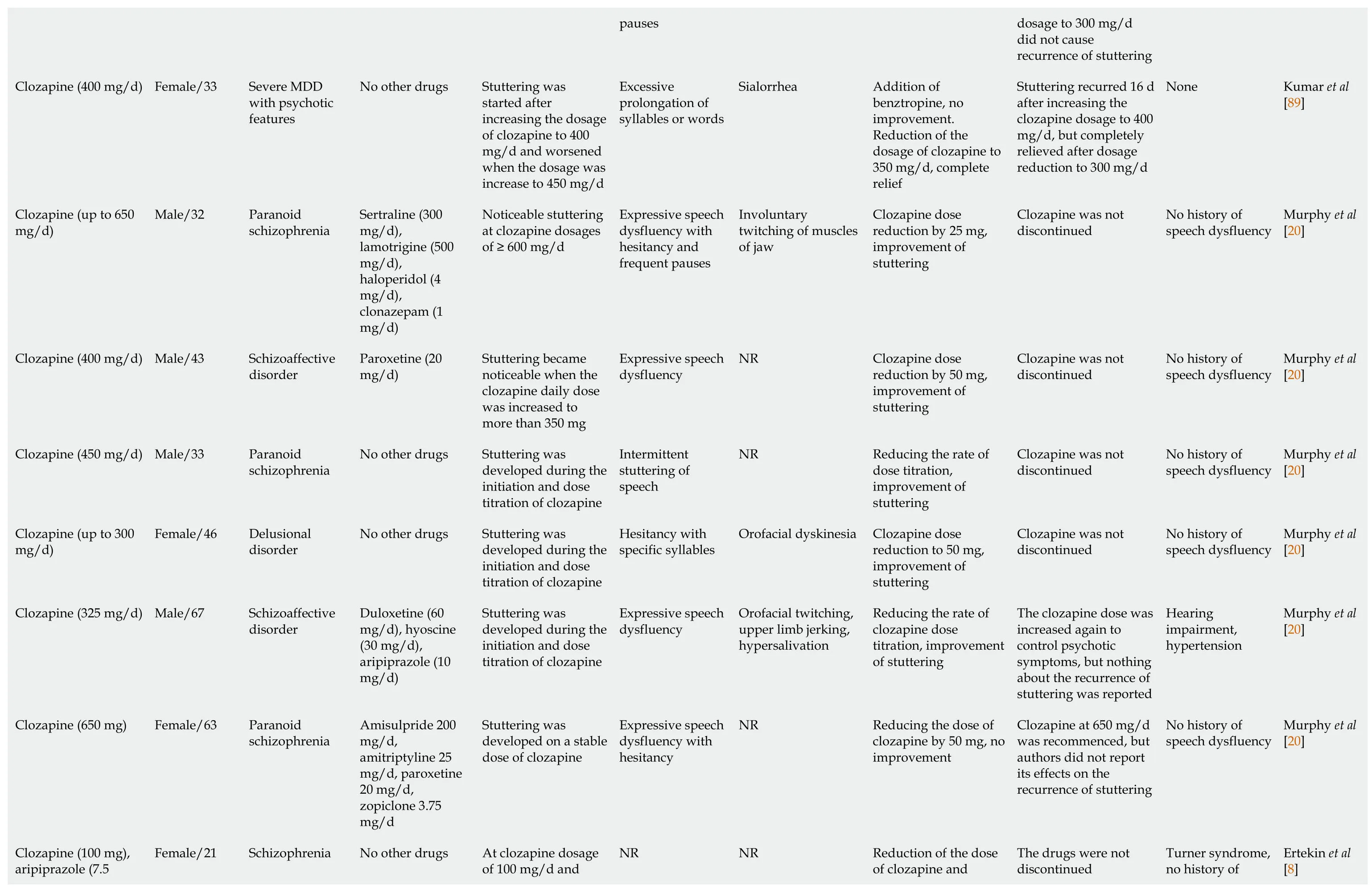
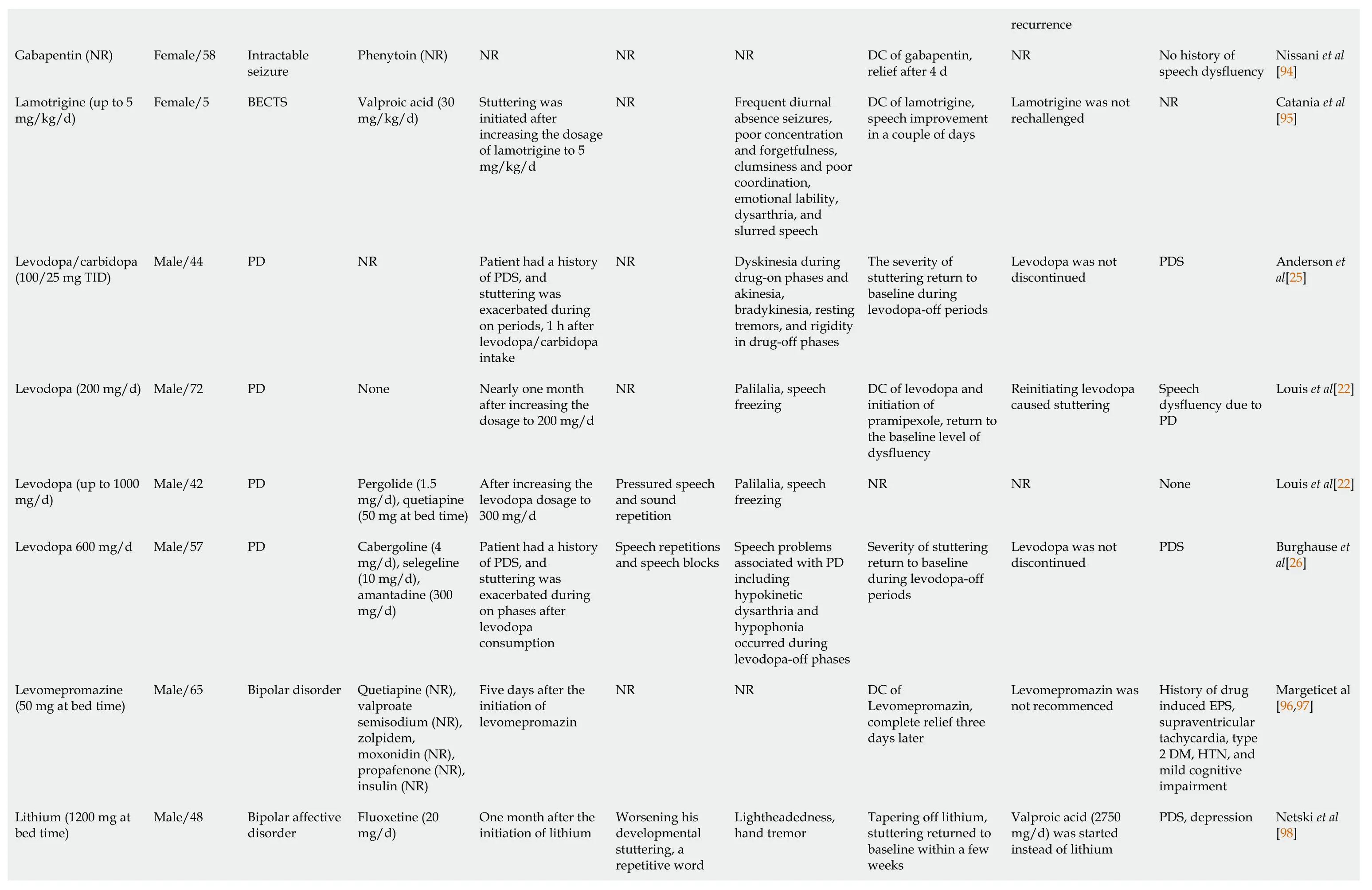
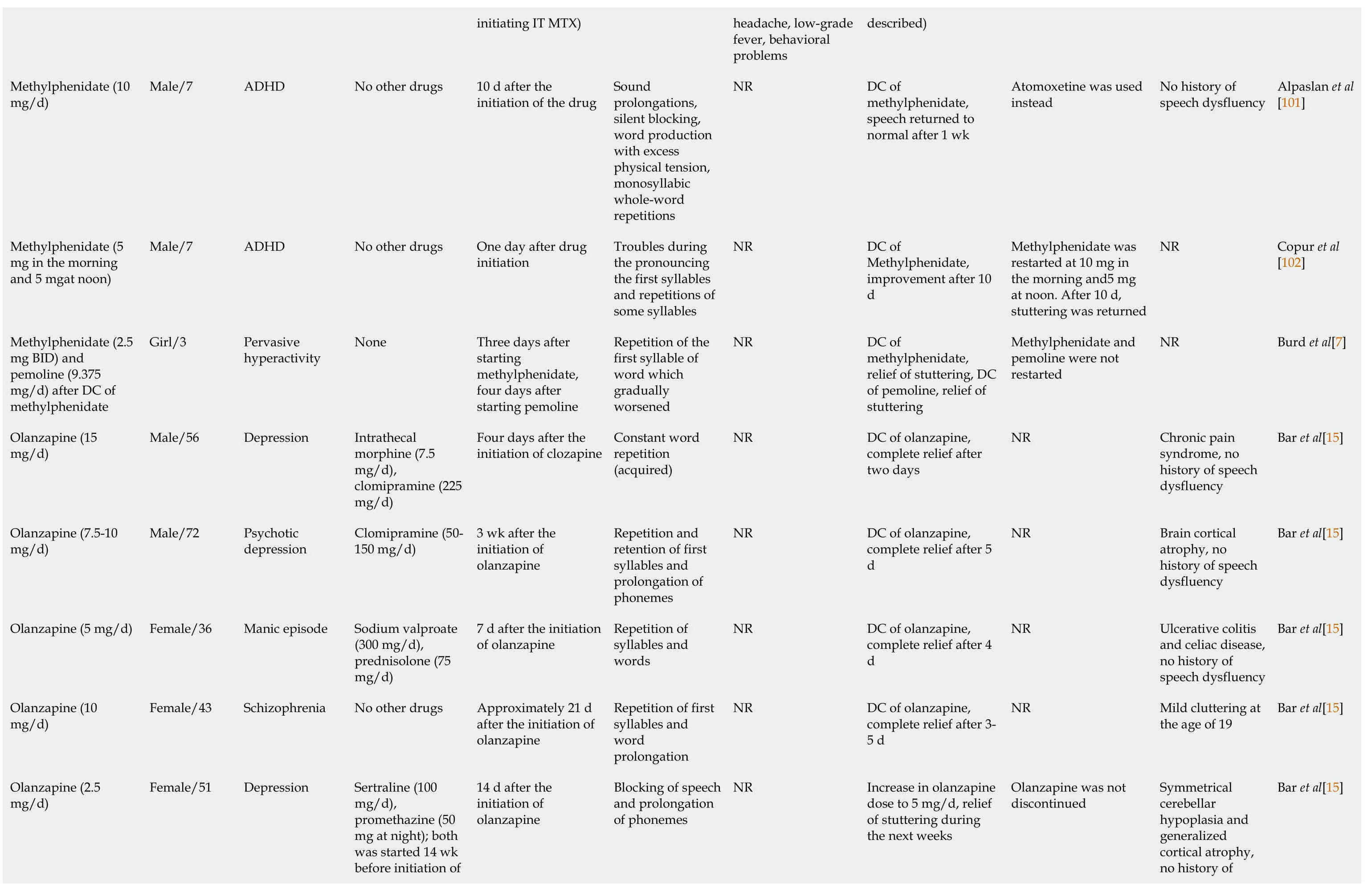
Therapeutic measures that resulted in significant improvement or complete relief of stuttering were drug withdrawal in 48 (55.8%) episodes,dose reduction in 18 (21%),addition of a new drug in three(3.6%),addition of a new drug besides dose reduction of the culprit drug in three (3.5%),and slow dose titration in two (2.3%).Moreover,in three (3.5%) episodes,the stuttering spontaneously remitted despite continuation of the offending drug with no dose reduction[16-18].However,three (3.5%) episodes did not respond to the dose reduction[19-21].For four (4.6%) episodes,the authors did not describe the actions taken to manage stuttering[22-25].In two (2.3%) cases with PDS and PD,stuttering was exacerbated during levodopa-on periods,and levodopa was not discontinued[26,27] (Table 3).

Table 3 Summary of the case reports of drug-induced stuttering

considerabl of developm stuttering Bupropion (SR) 150 mg BID Female/59 Major depressive disorder No other drugs Four days after starting the drug Sound prolongations,silent blocking,word production with excess physical tension,and monosyllabic whole-word repetitions.The stuttering was anxiogenic and restricted to initial syllables Slight finger dysdiadochokinesia DC of bupro complete re stuttering af Bupropion SR (300 mg/d)Male/38 Major depressive disorder No other drugs Two days after increasing the dosage from 150 to 300 mg/d Involuntary silent pauses or blocks,repetitions,prolongations of sounds,syllables,and words,affected rhythm of speech NR DC of bupro complete re stuttering Bupropion XL (300 mg/d)Male/53 Depression No other drugs After increasing the dosage of Bupropion Difficulty starting words and repetition of syllables NR Administra mg oral halo stuttering w improved a completely after 7 h Clozapine (up to 400 mg/d)Female/32 Paranoid schizophrenia No other drugs 4 wk after the initiation of clozapine NR Pharyngeal dystonia and buccolingual and facial dyskinesia associated with laryngeal dystonia DC of cloza dcomplete re Clozapine (was initiated at 400 mg/d and gradually increased to 900 mg/d)Female/28 schizoaffective disorder No other drugs Shortly after the initiation of clozapine at 400 mg/d and not relieved during the gradual increase in the dosage to 900 mg/d NR NR Dosage redu 700 mg/d,c relief Stuttering was initiated when the clozapine dosage was Generalized seizure followed by myoclonic jerks of The additio phenytoin a sodium valp Clozapine (450-750 mg/d)Female/49 Psychosis No other drugs NR

Risperidone and then clozapine (450 mg/d and 75 mg/d)Male/55 Schizophrenia No other drugs NR Occasional blocking,prolongation on word-initial sounds and repetitions of speech elements including onesyllable words at the beginning of his speech utterances Stammering and unusual limb and trunk movements related to risperidone,belching,persistent hiccupping,worsening of the facial tic,and the orofacial dyskinesia involving the lips and tongue related to clozapine Risperidone stuttering:N episode of c induced stu dose reduct mg/d and c clozapine;s improveme complete re stuttering;t time of cloz induced stu addition of valproate,considerabl improveme Clozapine (up to 600 mg/d)Male/35 Schizotypal personality disorder No other drugs At clozapine dosage of 250 mg/d and progressive worsening with dose escalation NR NR Reducing th of clozapine mg/d,comp Clozapine (200 mg/d)Male/24 Paranoid schizophrenia No other drugs After increase in the dosage of clozapine to 200 mg/d NR NR DC of cloza complete re Clozapine (250 mg/d)Male/23 Paranoid schizophrenia No other drugs At clozapine dosage of 250 mg/d (interval was not reported)NR NR Clozapine d reduction to mg/d,comp Clozapine (350 mg/d)Male/15 Undifferentiated schizophrenia Clomipramine (225 mg/d)Three years after the initiation of clozapine and clomipramine Repetitions of syllables and transient accelerations of speech rate Involuntary paroxysmal perioral movements,facial tic-like movements,myoclonic jerks of the upper limbs,GTC seizure Addition of acid at 500 m complete re stuttering w Frequent repetition and prolongation of syllables or words with frequent hesitations,blocking and Clozapine (up to 250 mg/d)Male/29 Undifferentiated schizophrenia No other drugs After the clozapine dosage titration from 137.5 mg/d to 150 mg/d No focal dystonia or any evidence of seizure-like activity Reducing an the dose of to 50 mg in and 75 mg a improveme stuttering
pauses Clozapine (400 mg/d)Female/33 Severe MDD with psychotic features No other drugs Stuttering was started after increasing the dosage of clozapine to 400 mg/d and worsened when the dosage was increase to 450 mg/d Excessive prolongation of syllables or words Sialorrhea Addition of benztropine improveme Reduction o dosage of cl 350 mg/d,c relief Clozapine (up to 650 mg/d)Male/32 Paranoid schizophrenia Sertraline (300 mg/d),lamotrigine (500 mg/d),haloperidol (4 mg/d),clonazepam (1 mg/d)Noticeable stuttering at clozapine dosages of ≥ 600 mg/d Expressive speech dysfluency with hesitancy and frequent pauses Involuntary twitching of muscles of jaw Clozapine d reduction b improveme stuttering Clozapine (400 mg/d)Male/43 Schizoaffective disorder Paroxetine (20 mg/d)Stuttering became noticeable when the clozapine daily dose was increased to more than 350 mg Expressive speech dysfluency NR Clozapine d reduction b improveme stuttering Clozapine (450 mg/d)Male/33 Paranoid schizophrenia No other drugs Stuttering was developed during the initiation and dose titration of clozapine Intermittent stuttering of speech NR Reducing th dose titratio improveme stuttering Clozapine (up to 300 mg/d)Female/46 Delusional disorder No other drugs Stuttering was developed during the initiation and dose titration of clozapine Hesitancy with specific syllables Orofacial dyskinesia Clozapine d reduction to improveme stuttering Clozapine (325 mg/d)Male/67 Schizoaffective disorder Duloxetine (60 mg/d),hyoscine(30 mg/d),aripiprazole (10 mg/d)Stuttering was developed during the initiation and dose titration of clozapine Expressive speech dysfluency Orofacial twitching,upper limb jerking,hypersalivation Reducing th clozapine d titration,im of stuttering Clozapine (650 mg)Female/63 Paranoid schizophrenia Amisulpride 200 mg/d,amitriptyline 25 mg/d,paroxetine 20 mg/d,zopiclone 3.75 mg/d Stuttering was developed on a stable dose of clozapine Expressive speech dysfluency with hesitancy NR Reducing th clozapine by improveme Clozapine (100 mg),aripiprazole (7.5 At clozapine dosage of 100 mg/d and Reduction o of clozapine Female/21 Schizophrenia No other drugs NR NR

mg/d)aripiprazole dosage of 7.5 mg/d addition of aripiprazole complete re Reduction o of aripipraz to 7.5 mg/d relief Clozapine (gradually increased to 450 mg/d)Male/16 Schizoaffective disorder Citalopram (NR),clonazepam (NR),atenolol (NR),lithium (NR)Approximately 22 d after increasing the clozapine dosage to 400 mg/d Persistent stuttering(difficulties with the pronunciation of letters “I,” “D,”and “T”)Orofacial dyskinesia with perioral twitching (started at clozapine dosage of 350 mg/d),microseizure according to EEG (at clozapine dosage of 400 mg/d)Substituting with divalp sodium,imp in stuttering receiving di sodium at 5 Clozapine (up to 600 mg/d)Female/22 Schizophrenia Fluoxetine (60 mg/d)Stuttering was developed after the clozapine dose escalation to 300 mg/d NR NR Reduction i clozapine d initiation of minimal im Clozapine (450 mg/d)Man/in early 40s NR No other drugs After increasing the clozapine daily dose from 400 mg to 450 mg NR Marked increase in seizure activity DC of cloza nothing was reported by authors Clozapine (200 mg/d)Male/38 Schizophrenia No other drugs Stuttering was evident at 200 mg/d and became so disabling at 350 mg/d NR NR Dose reduct clozapine an of amisulpir BDZ,reduc stuttering,D clozapine,c relief Clozapine (300 mg BID)Male/57 Paranoid schizophrenia Risperidone,IM injection (37.5 mg every 2 wk),Risperidone,oral(1.5 mg/d which increased to 2 mg BID on admission)Two days after admission (the dosage of clozapine,300 mg BID,was not changed on admission)NR Orofacial and extremities myoclonic jerks,drop attacks Clozapine d reduction to BID,resolut stuttering w days Clozapine (125 mg/d)Male/29 Schizophrenia No other drugs A few days after titrating the clozapine dosage to 125 mg/d Frequent repetitions of words that included broken words NR Reducing th clozapine d 100 mg/d,s improveme

Clozapine (up to 200 mg/d)female/25 Schizophrenia No other drugs At clozapine dosage dose of 150 mg/d(interval was not mentioned)NR Tonic-clonic epileptic seizure DC of cloza start of amis and biperid complete re stuttering an Divalproex sodium(600 mg/d)Male/45 Affective instability and irritability Citalopram (30 mg/d),promazine(100 mg/d)Four days after initiation of divalproex sodium Sound repetitions and prolongations(not restricted to the initial syllable and caused pronounced difficulty in starting and completing his sentences)NR DC of dival dcomplete re Divalproex sodium(1500 mg/d in divided dose)Male/56 Bipolar affective disorder Olanzapine (10 mg/d),lorazepam(4 mg/d,gradually stopped along with increase in the dose of divalproex)Two weeks after increasing the dosage of divalproex from 1000 to 1500 mg/d A moderately pressured speech,articulation of speech,alterations in intensity and timings of utterance segments,Involuntary repetitions and prolongations of sounds,syllables,words or phrases,involuntary silent pauses or blocks NR DC of dival instant ame the stutterin Desipramin (300 mg/d)Male/28 Dystimia,primary type,major depression Doxepin (50 mg at bed time)Two months after increasing the dosage of desipramine Stuttering with difficulty in articulation Minimal dryness of mouth before stuttering,myoclonic jerking (twitching movements around his jaw) concomitant with stuttering DC of both hcomplete re Fluphenazine (up to 50 mg/d)Male/35 Schizophrenia Benztropine mesylate (4 mg/d)12 d after increasing fluphenazine dosage to 50 mg/d NR EPS Dosage redu mg/d,comp
Gabapentin (NR)Female/58 Intractable seizure Phenytoin (NR)NR NR NR DC of gabap relief after 4 Lamotrigine (up to 5 mg/kg/d)Female/5 BECTS Valproic acid (30 mg/kg/d)Stuttering was initiated after increasing the dosage of lamotrigine to 5 mg/kg/d NR Frequent diurnal absence seizures,poor concentration and forgetfulness,clumsiness and poor coordination,emotional lability,dysarthria,and slurred speech DC of lamo speech impr in a couple Levodopa/carbidopa(100/25 mg TID)Male/44 PD NR Patient had a history of PDS,and stuttering was exacerbated during on periods,1 h after levodopa/carbidopa intake NR Dyskinesia during drug-on phases and akinesia,bradykinesia,resting tremors,and rigidity in drug-off phases The severity stuttering re baseline du levodopa-of Levodopa (200 mg/d)Male/72 PD None Nearly one month after increasing the dosage to 200 mg/d NR Palilalia,speech freezing DC of levod initiation of pramipexol the baseline dysfluency Levodopa (up to 1000 mg/d)Male/42 PD Pergolide (1.5 mg/d),quetiapine(50 mg at bed time)After increasing the levodopa dosage to 300 mg/d Pressured speech and sound repetition Palilalia,speech freezing NR Levodopa 600 mg/d Male/57 PD Cabergoline (4 mg/d),selegeline(10 mg/d),amantadine (300 mg/d)Patient had a history of PDS,and stuttering was exacerbated during on phases after levodopa consumption Speech repetitions and speech blocks Speech problems associated with PD including hypokinetic dysarthria and hypophonia occurred during levodopa-off phases Severity of s return to ba during levo periods Levomepromazine(50 mg at bed time)Male/65 Bipolar disorder Quetiapine (NR),valproate semisodium (NR),zolpidem,moxonidin (NR),propafenone (NR),insulin (NR)Five days after the initiation of levomepromazin NR NR DC of Levomepro complete re days later Worsening his developmental stuttering,a repetitive word Lithium (1200 mg at bed time)Male/48 Bipolar affective disorder Fluoxetine (20 mg/d)One month after the initiation of lithium Lightheadedness,hand tremor Tapering of stuttering re baseline wit weeks

stutter that severely limited his verbal communication ability Lithium (900 mg twice daily)Male/10 Bipolar disorder Risperidone (4 mg bed time),clonidine (0.1 mg 3 times daily),melatonin (3 mg at bed time),famotidine (20 mg BID)Two days after increasing the dose of lithium,stuttering was worsened Syllable repetitions,occurred only at the beginning of sentences NR Dose adjust lithium to 6 the morning mg at night returned to after 2 d Lithium (the dose was not mentioned,but lithium was used for a long time)Female/86 Bipolar disorder Donepezil (NR),primidone (NR),risperidone (NR)After a chronic use of lithium,stuttering was started and stayed for 3 more mo.The lithium level was elevated (2.0 mmol/L)Starting a few words fluently,then repeating syllables and words and terminating the sentence abruptly NR DC of lithiu complete re stuttering af weeks Memantine (10 mg/d)Male/9 Autistic disorder No other drugs After increasing the dose Deterioration of primary behaviors of developmental stuttering includingsound repetition,and sound prolongation on first and middle vowels,and difficulty for starting to speak.His parents explained that the child could only start to speak after a deep and audible breath NR Reduction o memantine 7.5 mg/d,improveme acquired stu after severa of memanti stuttering w to baseline a Memantine (5 mg/d)Male/4 Autism No other drugs After increasing the dose The difficulty was with the start of the speech and the child could only start to speak after a deep and audible breath NR The drug w continued a dose as the was tolerab gradually w increased to relief of spe difficulty After achieving cumulative dose of 62.5 mg (26 d after Dysphasia progressed to aphasia,mild Three mont initiation of(no interven Methotrexate(cumulative dose of 62.5 mg,IT)Female/22 Pre-B acute lymphoblastic leukemia NR NR
initiating IT MTX)headache,low-grade fever,behavioral problems described)Methylphenidate (10 mg/d)Male/7 ADHD No other drugs 10 d after the initiation of the drug Sound prolongations,silent blocking,word production with excess physical tension,monosyllabic whole-word repetitions NR DC of methylphen speech retu normal afte Methylphenidate (5 mg in the morning and 5 mgat noon)Male/7 ADHD No other drugs One day after drug initiation Troubles during the pronouncing the first syllables and repetitions of some syllables NR DC of Methylphen dimproveme Methylphenidate (2.5 mg BID) and pemoline (9.375 mg/d) after DC of methylphenidate Girl/3 Pervasive hyperactivity None Three days after starting methylphenidate,four days after starting pemoline Repetition of the first syllable of word which gradually worsened NR DC of methylphen relief of stut of pemoline stuttering Olanzapine (15 mg/d)Male/56 Depression Intrathecal morphine (7.5 mg/d),clomipramine (225 mg/d)Four days after the initiation of clozapine Constant word repetition(acquired)NR DC of olanz complete re two days Olanzapine (7.5-10 mg/d)Male/72 Psychotic depression Clomipramine (50-150 mg/d)3 wk after the initiation of olanzapine Repetition and retention of first syllables and prolongation of phonemes NR DC of olanz dcomplete re Olanzapine (5 mg/d)Female/36 Manic episode Sodium valproate(300 mg/d),prednisolone (75 mg/d)7 d after the initiation of olanzapine Repetition of syllables and words NR DC of olanz dcomplete re Olanzapine (10 mg/d)Female/43 Schizophrenia No other drugs Approximately 21 d after the initiation of olanzapine Repetition of first syllables and word prolongation NR DC of olanz complete re 5 d Sertraline (100 mg/d),promethazine (50 mg at night);both was started 14 wk before initiation of Olanzapine (2.5 mg/d)Female/51 Depression 14 d after the initiation of olanzapine Blocking of speech and prolongation of phonemes NR Increase in o dose to 5 m of stuttering the next we

olanzapine Olanzapine (10 mg/d)Male/42 Schizophrenia Zopiclone (7.5 mg/d)Two days after the initiation of olanzapine Difficulty in articulating words properly NR DC of olanz complete re two days Olanzapine (10 mg/d)Male/42 Paranoid ideation Venlafaxine (150 mg/d),promazine(200 mg/d)Four days after the initiation of olanzapine Repetition and retention of first syllables and prolongation of phonemes NR DC of olanz complete re two days Olanzapine (10 mg/d)Male/21 Psychotic disorder No other drugs Three days after the initiation of olanzapine disturbance in the fluency and time patterning of speech,repetition of sounds and syllables,blocking between words NR DC of olanz start of quet complete re three days Phenytoin (200 mg/d)Male/42 Seizure due to head injury No other drugs Shortly after initiation of phenytoin Predominantly part-word repetitions and prolongation Abnormality of speech muscle fine motor control Addition of gradual DC phenytoin,s decrease in frequency o dysfluencie improved m performanc Phenytoin (20 mg/kg LD and 5 mg/kg/d MD)Male/3 GTC seizure due to head trauma No other drugs 10 d after the initiation of phenytoin NR NR DC of phen initiation of valproate,c relief 10 d a phenytoin Pregabalin (75 mg twice daily)Female/31 Complex regional pain syndrome No other drugs After taking the second dose of pregabalin on the first day A slurred speech NR DC of prega complete re one week Pregabalin (75 mg twice daily)Female/68 Herpes zoster Acyclovir (800 mg five times daily)Three days after the initiation of pregabalin NR Frequent blepharospasm DC of pregabalin;a of symptom days and co relief after o Pyrethrin product containing 0.33%pyrethrum extract and 4% piperonyl butoxide (3 times Female/2 (the child’s mother,who was breastfeeding An increase in clumsiness,slight erythematous rash ofapproximately 3 cm × 2 cm on the Repeated episodes of head lice No other drugs Two days after the last period of mother’s treatment An acute onset of stuttering especially at the initiation of the speech Six weeks postexposu

overa period of 12 d left on the scalp for 10 min)her atleast one time per day,were receiving this topical product)occiput of the scalp Risperidone (4 mg/d,then 8 mg/d)Male/32 Aggravated psychotic disorder Lorazepam (1 mg/d)Stuttering was initiated after the dose increase to 4 mg/d,and worsened 16 d after the dose increase to 8 mg/d Severe sound repetitions and interjections in a way that it was difficult to understand his words Slight akathisia-like symptoms such as anxiety and restlessness (not prominent)No action,s diminished Risperidone (4 mg)Female/48 Psychosis Lorazepam (1 mg PRN),procyclidine(5 mg BID for treatment of EPS)11 d after taking risperidone Repetitions in the speech,pausing within a word and her speech,an excess of physical tension in the speech NR A little decr risperidone reduction in Risperidone (at a dose of 1 mg/d for 2 yr)Male/21 Behavioral disorder No other drugs After chronic treatment with lowdose of risperidone Prolongation of sounds,hearable blocks,repetitions of single-syllable words NR No action,s was decreas dminimal lev Sertraline (100 mg daily)Male/36 Major depression Alprazolam (0.25 mg 3 TID)Two weeks after increasing the dosage from 50 to 100 mg/d Normal vocabulary,decreased rate of speech,normal tone,interrupted words NR DC of serter speech prob resolved aft Sertraline (50 mg daily)Female/32 Recurrent depression No other drugs During the third week of starting the drug¸ stuttering occurred and worsened over a 3-d period Difficulty in starting and completing the sentences Feeling nervous,increased restlessness,and insomnia two days before the onset of stuttering DC of sertra complete re stuttering af
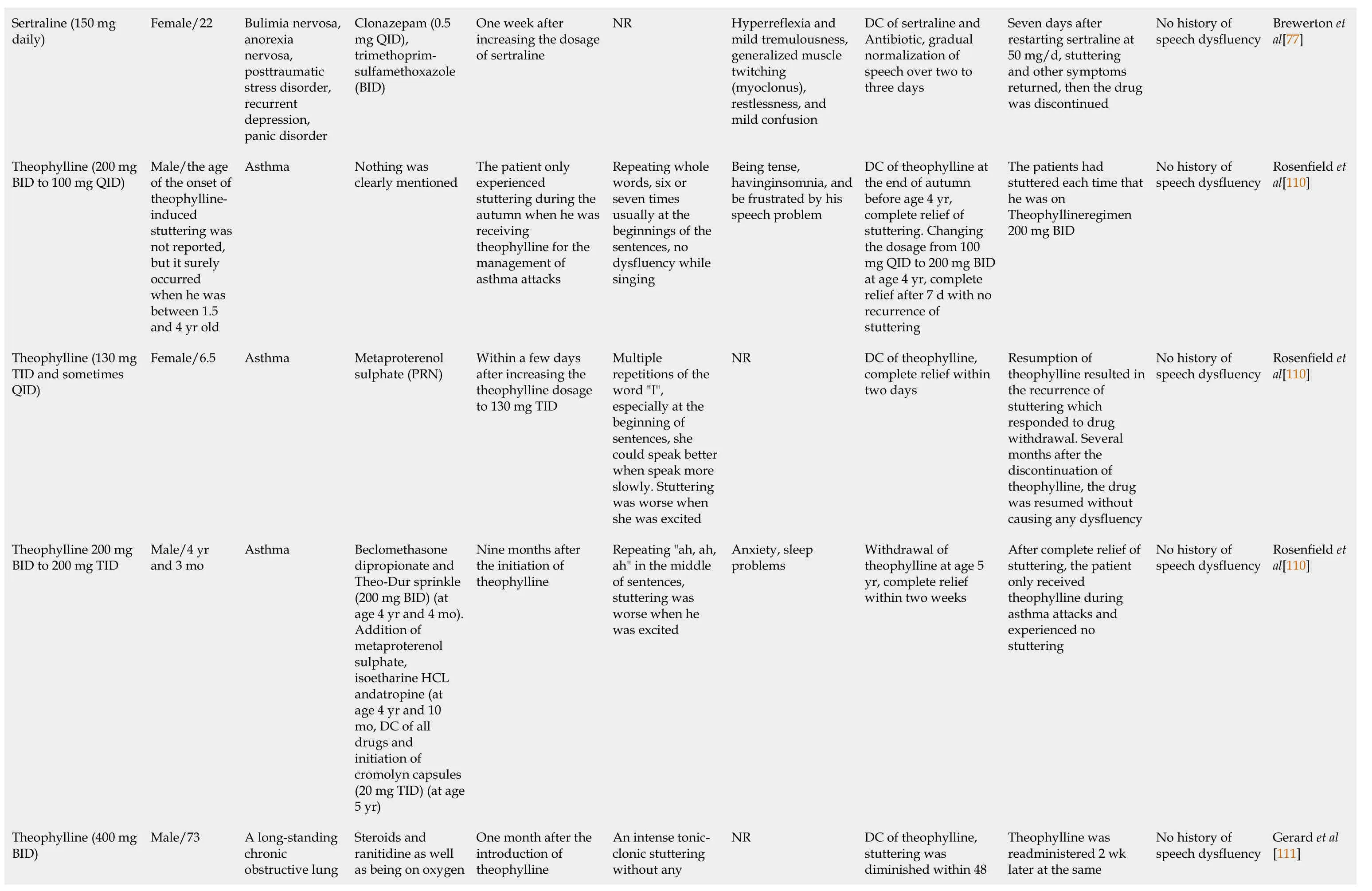
Sertraline (150 mg daily)Female/22 Bulimia nervosa,anorexia nervosa,posttraumatic stress disorder,recurrent depression,panic disorder Clonazepam (0.5 mg QID),trimethoprimsulfamethoxazole(BID)One week after increasing the dosage of sertraline NR Hyperreflexia and mild tremulousness,generalized muscle twitching(myoclonus),restlessness,and mild confusion DC of sertra Antibiotic,g normalizati speech over three days Theophylline (200 mg BID to 100 mg QID)Male/the age of the onset of theophyllineinduced stuttering was not reported,but it surely occurred when he was between 1.5 and 4 yr old Asthma Nothing was clearly mentioned The patient only experienced stuttering during the autumn when he was receiving theophylline for the management of asthma attacks Repeating whole words,six or seven times usually at the beginnings of the sentences,no dysfluency while singing Being tense,havinginsomnia,and be frustrated by his speech problem DC of theop the end of a before age 4 complete re stuttering.C the dosage f mg QID to 2 at age 4 yr,relief after 7 recurrence o stuttering Theophylline (130 mg TID and sometimes QID)Female/6.5 Asthma Metaproterenol sulphate (PRN)Within a few days after increasing the theophylline dosage to 130 mg TID Multiple repetitions of the word "I",especially at the beginning of sentences,she could speak better when speak more slowly.Stuttering was worse when she was excited NR DC of theop complete re two days Theophylline 200 mg BID to 200 mg TID Male/4 yr and 3 mo Asthma Beclomethasone dipropionate and Theo-Dur sprinkle(200 mg BID) (at age 4 yr and 4 mo).Addition of metaproterenol sulphate,isoetharine HCL andatropine (at age 4 yr and 10 mo,DC of all drugs and initiation of cromolyn capsules(20 mg TID) (at age 5 yr)Nine months after the initiation of theophylline Repeating "ah,ah,ah" in the middle of sentences,stuttering was worse when he was excited Anxiety,sleep problems Withdrawal theophyllin yr,complete within two A long-standing chronic obstructive lung An intense tonicclonic stuttering without any DC of theop stuttering w diminished Theophylline (400 mg BID)Male/73 Steroids and ranitidine as well as being on oxygen One month after the introduction of theophylline NR

day;TID:Three times a day;VPA:Valproic acid.LD:Loading dose;MD:Maintenance dose;MDD:Major Depressive Disorder;MTX:Methotrexate;NR:Not reported;PD:Parkinson disease;PDS:Persistent developmental stuttering;PRN:Pro re nata (as needed);QID:Four times a disease;DC:Discontinue,DM:Diabetes mellitus;EPS:Extrapyramidal side effect;GERD:Gastroesophageal reflux disease;GTC:Generalized tonic-colonic seizure;HTN:Hypertension;IM:Intramuscular;IT:Intrathecal;IV:Intravenous;ADHD:Attention-deficit hyperactivity disorder;BECTS:Benign focal epilepsy of childhood with centrotemporal spikes;BID:Two times per day;BDZ:Benzodiazepine;CBZ:Carbamazepine;COPD:Chronic obstructive pulmonary(up to 800 mg/d)2.Chlorpromazine mg/d)1.Trifluoperazine (30 Male/40 Schizophrenia pneumoconiosis secondary to disease mg/d)Trihexyphenidyl (5 dosage to 800 mg/d chlorpromazine 2.After increasing dosage to 30 mg/d trifluoperazine increasing the 1.Four days after NR components extrapyramidal NR relief to 400 mg/d,complete chlorpromazine dose Reduction of improvement.benztropine,no 2.Addition of complete relief trifluoperazine,improvement.DC of trihexyphenidyl,no 1.Increasing dosage of h of stuttering mg/d caused cessation chlorpromazine to 400 reducing the dosage of return of stuttering;700 mg/d caused the of chlorpromazine to Increasing the dosage treatment was stopped daysand persisted until recurred within a few speech disorder dosage,and the same speech dysfluency No history of al[10]Nurnberg et
PATHOPHYSlOLOGY
In this section,the abnormalities suggested in the pathogenesis of developmental stuttering and PDS are described.Then,we propose some mechanisms for DIS based on the underlying impairments involved in the pathogenesis of PDS and developmental stuttering.
For producing a fluent speech,orofacial as well as respiratory muscles must work properly.Different areas of the brain including several parts of the cerebral cortex and subcortical structures such as the basal ganglia (BG) and cerebellum are involved in speech production.Functional abnormalities of each part of these areas may cause speech dysfluency.It has been suggested that dysfunction in the different parts and networks of cerebral cortex engaged in speech production[28],the impairments in the neural connections between the cerebral cortex,the BG,and the thalamus,which are called cortico-BGthalamocortical circuit (CBTC)[28,29],and/or the dysfunction of the BG are involved in the pathogenesis of developmental stuttering[28,29].
CBTC AND STUTTERlNG
Several neural circuits are engaged in the process of speech production.One of these circuits that has received much attention in the pathogenesis of stuttering is CBTC[28,29].The BG consist of input,intrinsic,and output nuclei.The input nuclei receive information from different parts of the brain,especially the cerebral cortex,the thalamus,and the substantia nigra,and send signals to the intrinsic nuclei for further processing and then to the output nuclei.The output nuclei relay signals to the thalamus which sends signals back to the part of the cerebral cortex from which the primary signal was originated.The input nuclei consist of the putamen and the caudate nucleus,collectively named the striatum.The intrinsic nuclei consist of the external segment of the globus pallidus (GPe),the subthalamic nucleus (STN),and the substantia nigra pars compacta (SNpc).The internal segment of the globus pallidus (GPi) and the substantia nigra pars reticulata (SNpr) make the output nuclei[30].
The striatum has two types of neurons including gamma-aminobutyric acid-ergic (GABAergic)medium-sized spiny neurons (MSNs) representing 90%-95% of the striatal neurons and GABAergic/cholinergic interneurons.The striatum receives inputs from different parts of the brain including excitatory glutamatergic inputs from different parts of the cerebral cortex,motor cortex,supplementary motor area (SMA),pre-SMA,auditory cortex,somatosensory cortex,and the thalamus and dopaminergic inputs from SNpc[30].BG match motor,sensory,and cognitive context received from different parts of the cerebral cortex[31] and send signals to the thalamus to stimulate the cerebral cortex to initiate the desired movement,e.g.,terminating production of the previous phoneme and initiating the next phoneme in the case of speaking,and inhibit competing movements[32].The cerebral cortex sends signals through corticobulbar tracts to the orofacial and respiratory muscles including the muscles of larynx,pharynx,lips,and tongue[33],activates the proper group of muscles,and inhibits competing muscles whose activation interferes with the production of the desired movement.
The signals that are received by the input nuclei of BG are transmittedviatwo pathways:Direct and indirect.The activation of the direct pathway stimulates the cerebral cortex and therefore activates the right motor program while the activation of the indirect pathway inhibits the cerebral cortex and therefore,all other competing motor programs[2,28].
In the direct pathway,MSNs,which have N-methyl-D-aspartate (NMDA) glutamate receptors,D1 dopamine receptors,A1 adenosine receptors,and M4 muscarinic receptors[34] and release gammaaminobutyric acid (GABA),substance P,and dynorphin[35],project to the SNpr and GPi,the output nucleus of BG.MSNs are stimulated by glutamatergic projections from the cerebral cortex.The activated MSNs release GABA,which inhibits the output nucleus.GABAergic projections from the output nucleus inhibit the glutamatergic neurons of the thalamus.Therefore,the inhibition of the output nucleus by MSNs disinhibits thalamic neurons which ultimately activate the cerebral cortex and increase locomotor activity[35] (Figure 1).
MSNs in the indirect pathway,which have NMDA glutamate receptors,D2 dopamine receptors,A2A adenosine receptors,and M1 muscarinic receptors[34] and release GABA and enkephalin,project to the output nucleus through the GPe and STN.The GPe has GABAergic neurons that inhibit STN neurons which are glutamatergic cells.The release of glutamate because of the activation of the cerebral cortex stimulates MSNs in the indirect pathway to release GABA.GABA inhibits the GPe and therefore disinhibits the STN.Release of glutamate from the STN stimulates the inhibitory GABAergic neurons of the output nucleus,which inhibits thalamic neurons and therefore cerebral cortex,resulting in decreased locomotor activity (Figure 1).It has been proposed that the direct and indirect pathways have interactions with each other,and their integration and balanced activation during movement selection is required for the proper execution of motor programs[36,37].
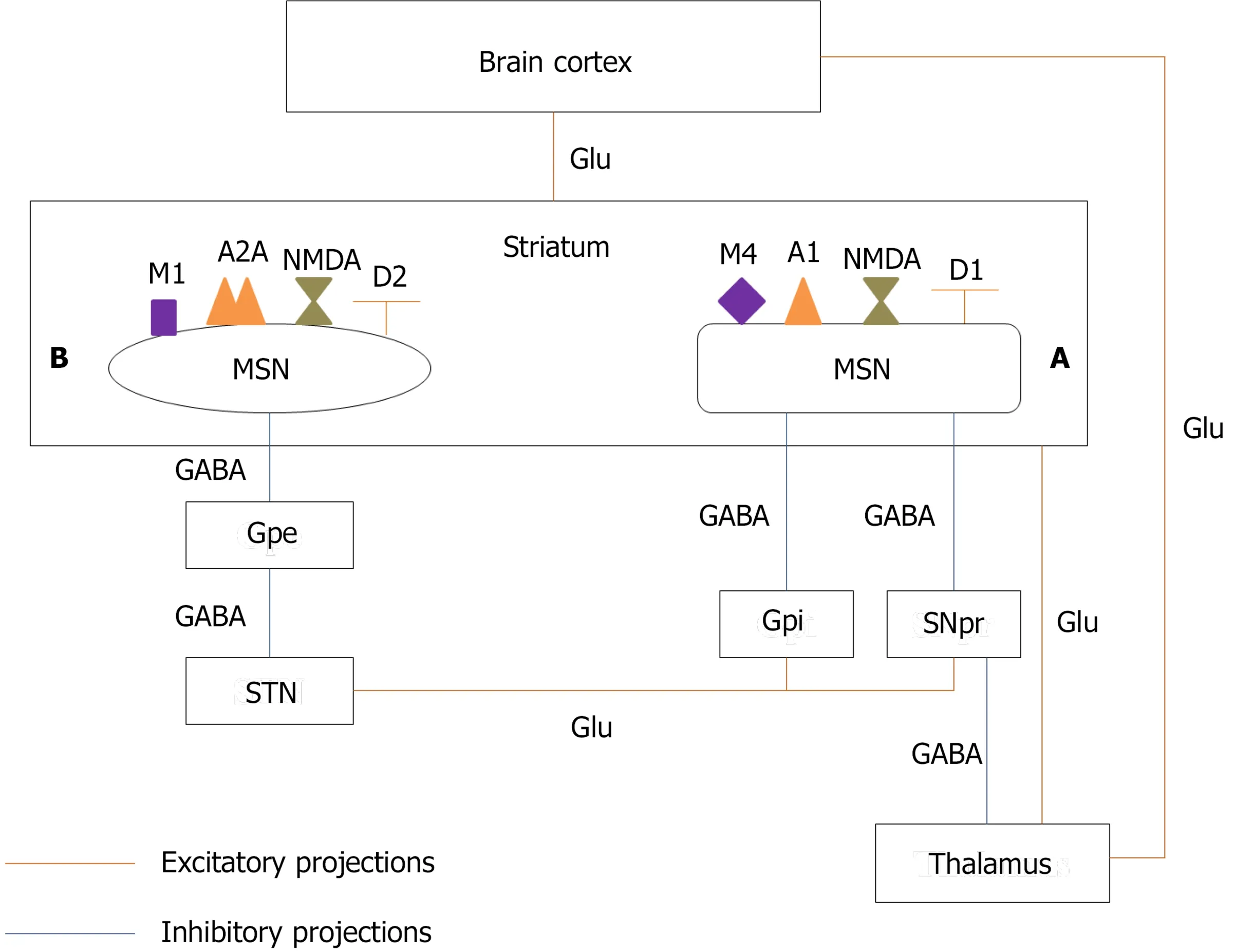
Figure 1 Schematic graph of direct and indirect pathways of basal ganglia.
ROLE OF DOPAMlNE lN THE BG MOTOR ClRCUlT
As mentioned above,D1,A1,and M4 receptors are colocalized on MSNs in the direct pathway[34].The stimulation of D1 receptors activates MSNs in the direct pathway and stimulates this pathway[28].Blocking A1 and M4 receptors facilitates the dopamine neurotransmission.Therefore,A1 and M4 antagonists also stimulate the direct pathway[34].Neurons of the indirect pathway have D2,A2A,and M1 receptors[34].The activation of D2 receptors inhibits the indirect pathway[28].A2A and M1 receptors antagonists also increase the dopamine signaling and therefore suppress the indirect pathway.Since these two pathways have a cross talk and coordinated activity,disturbing their coordination can cause movement disorders such as dystonia,dyskinesia,and stuttering.Therefore,both increased and decreased dopamine neurotransmission in the striatum may cause stuttering by impairing the balance between the direct and indirect pathways.
WHlTE MATTER FlBER TRACTS AND STUTTERlNG
Other changes that can affect connectivity between different areas of the brain involved in the speech motor control are the white matter abnormalities.The white matter tracts,bundles of myelinated axons,relay signals between different areas of the brain and therefore coordinate their communication and function[38].Severalin vitroand animal studies and a small number of human studies have found multiple neurotransmitters,including glutamate,adenosine,GABA,glycine,dopamine,serotonin,acetyl choline,histamine,norepinephrine,and substance P,and their receptors in the white matter.It has been proposed that glutamate and purine signaling have the most prominent effects on the white matter functioning;however,it seems that the white matter requires a coordinated action of all of these neurotransmitters for conduction of action potentials and maintaining signal integrity through very long signal transmission axonal pathways[38].Different studies in adults[33,39] and adolescents and young people[40] with developmental stuttering demonstrated the reduced integrity of the white matter fiber tracts.It may be proposed that an agent that impairs the normal activity of one or some of the neurotransmitters in the white matter may impair signal transmission between different areas of the brain engaged in speech motor control and result in stuttering.Moreover,in some psychiatric disorders such as schizophrenia and bipolar disorder,one of the pathological findings in the CNS is myelin loss or disruption[41].Of cases included in the present review,25,5,and 6 had schizophrenia,schizoaffective disorder,and bipolar disorder,respectively.As a result,it can be suggested that drugs disrupting normal neurotransmitter balance in the white matter,which already has an underlying impairment in these patients,may exacerbate white matter dysfunction.
STUTTERlNG lNDUCED BY DRUGS AFFECTlNG DOPAMlNE NEUROTRANSMlSSlON
Increased dopamine neurotransmission in BG and stuttering
Evidence that supports the role of the dopamine excess in the pathophysiology of stuttering includes the reduction of stuttering by antipsychotic drugs,which are dopamine blockers,such as haloperidol,risperidone,olanzapine,aripiprazole,and asenapine[42],the finding of Wuet al[43] that showed the excessive striatal dopamine activity and increased uptake of fluoro-l-3,4-dihydroxy-phenylalanine,a precursor of dopamine,in several parts of the brain in persons who stutter in comparison to healthy controls,and computational modeling of stuttering by Civieret al[44].Furthermore,it has been shown that children aged 2.5-3 years,the age of onset of developmental stuttering in most children,have more density of D2 than D1 receptors and therefore low D1/D2 density in the striatum in comparison to older children.Therefore,drugs like haloperidol,which is a highly selective D2 antagonist,decrease this D1/D2 imbalance and the severity of stuttering.Besides the above-mentioned studies conducted in persons with developmental stuttering,cases of exacerbation of stuttering by levodopa in patients with PD[23,26,27] also propose a role for dopamine excess in the pathogenesis of NS.Changet al[28] have suggested that the inhibition of the indirect pathway in the states of dopamine excess decreases the suppressing effect of this pathway on the competing motor programs.Therefore,choosing correct motor program over incorrect ones becomes difficult,which could ultimately delay the initiation of the right motor program.This delay may cause speech blockage or sound prolongation.Furthermore,in this situation,the proper signal that originated from the direct pathway and stimulates the right motor program may be initiated but suffers premature termination which may lead to the repetitions[28].
In conclusion,drugs such as levodopa,a precursor of dopamine,methylphenidate that increases the extracellular level of dopamine in the striatum[45],amphetamines that increase the release of catecholamines mainly dopamine and nerve-end particles (NEP) from presynaptic nerves and inhibit the reuptake of dopamine and NEP into presynaptic neurons[46],and phenytoin that has been proposed as a dopamine enhancer in the BG pathways may cause stuttering by increasing the dopamine neurotransmission in BG[47,48].
Decreased dopamine neurotransmission in BG and stuttering
Reduced dopamine neurotransmission in the striatum also can cause stuttering.For example,some patients with PD,the disorder that is mainly characterized by the dopamine depletion from BG,experience new-onset NS[49],exacerbation of PDS[26,27],or re-emergence of developmental stuttering[50].Changet al[28] proposed that in this state,the decreased excitation of the direct pathway results in reduced stimulation of the correct motor program and its ability to compete other motor programs.This also may result in unstable or delayed production of signals initiating the right speech motor program.
ANTlPSYCHOTlCS-lNDUCED STUTTERlNG
Although some studies have shown the relative efficacy of antipsychotic drugs in the treatment of stuttering[42],there are case reports of antipsychotics-induced stuttering.All studies that reported efficacy of antipsychotic drugs in reducing stuttering were conducted in patients with PDS.However,all cases of antipsychotics-induced stuttering had a psychotic disorder,which was schizophrenia in the majority of them.Elevated dopamine levels and excessive dopamine activity in the striatum are present in both developmental stuttering[42,43] and schizophrenia.Therefore,the opposite effects of dopamine blockers in these disorders,improving stuttering in some cases of developmental stuttering but causing stuttering in some patients with schizophrenia,indicate that effects of these drugs on the dopamine activity in other parts of the brain and on other neurotransmitters may be responsible for their different effects on speech motor control.Furthermore,abnormalities in the brain of patients with psychotic disorders are extensive and are not comparable to persons with developmental stuttering.These differences also may justify why a dopamine blocker can be a therapeutic option in PDS but a causative agent of stuttering in the psychotic disorders.
However,it should be noted that studies by Fishet al[51] and Langovaet al[52] demonstrated that not all persons with developmental stuttering respond to the dopamine blockers.In the study conducted by Fishet al[51],14 out of 28 persons who stuttered Prader-Willi syndrome (PWS) and received amphetamine experienced improvement in stuttering while two got worse.Of 12 PWS who did not improve by amphetamine,eight got better on trifluoperazine,a D2 blocker.Four participants did not show any improvement neither by each medication nor by their combination.Similarly,in the study conducted by Langovaet al[52],88% of PWS got better on phenmetrazine,a stimulant,while 67% deteriorated using chlorpromazine.These findings have led to the suggestion of the hypothesis that persons with developmental stuttering may be classified as the dopamine blocker-responsive or stimulantresponsive[29].
In the present review and study conducted by Trenqueet al[6],the majority of cases of DIS were caused by clozapine.Regarding the effects of antipsychotics on dopamine receptors,all antipsychotics except than clozapine,olanzapine,ziprasidone,and asenapine have a higher affinity for D2 receptors than D1 receptors.Clozapine,olanzapine,ziprasidone,and asenapine equally block both D1 and D2 receptors.Furthermore,clozapine and asenapine have a lower affinity for dopamine receptors in comparison to olanzapine and ziprasidone[53].Clozapine is one of the most effective antipsychotic drugs[54];however,because of its serious side effects such as agranulocytosis,seizure,and cardiovascular adverse effects[55],clozapine is considered as one of the last options in the treatment of schizophrenia and other psychotic disorders.Therefore,many patients had received several antipsychotics prior to the initiation of clozapine.Long-term blockage of D2 receptors while sparing D1 receptors caused by other antipsychotics results in the supersensitivity of D2 receptors[56].The affinity of clozapine for blocking D2 receptors is lower than that of many other antipsychotics[53].Therefore,after the initiation of clozapine,decreased D2 blocking combined with the supersensitivity of D2 receptors creates a state of increased D2 stimulation which finally inhibits the indirect pathway.On the other hand,antagonizing the D1 receptors inhibits the direct pathway.The inhibition of the indirect pathway impairs the suppression of the competing motor programs.Besides,the inhibition of the direct pathway decreases cerebral cortex stimulation and locomotor activity,which causes difficulties in initiating next segment in a movement sequence like speaking.Clozapine also is a 5HT2aand 5HT2creceptor blocker[55].Reducing the serotonin neurotransmission increases the dopamine transmission in the prefrontal cortex,which may also cause stuttering.Although clozapine is a potent M1 antagonist[55],the effect that facilitates the dopamine neurotransmission in the direct pathway,the final result of antagonizing all above-mentioned receptors is the inhibition of both direct and indirect pathways and therefore impaired speech motor control.Moreover,changing the normal function of dopamine,serotonin,acetylcholine,and norepinephrine,by blocking α1 receptors,and histamine,by blocking H1 receptors[55],can disturb normal functions of the white matter and cause stuttering.
Other antipsychotics that are included in the present review are olanzapine,risperidone,aripiprazole,chlorpromazine,fluphenazine,and trifluoperazine.Olanzapine is very similar to clozapine regarding the affinity for different receptors including D1,D2,5HT2A,5HT2C,M1,α1,and H1 receptors[57].Other antipsychotics such as risperidone,chlorpromazine,and fluphenazine are potent inhibitors of D2 receptors without any considerable effect on D1 receptors.Chlorpromazine also is a potent M1 antagonist while risperidone and fluphenazine have no considerable effect on M1 receptor.The efficacy of risperidone in antagonizing 5HT receptors is comparable to that of olanzapine and more than the efficacy of chlorpromazine,fluphenazine,and trifluoperazine.Aripiprazole is a partial agonist of D2 and 5HT1Areceptors and antagonist of 5HT2Areceptor[57].We suggest that these antipsychotics can cause extrapyramidal side effects (EPS) which may manifest as stuttering as well as other movement disorders by impairing the balanced and coordinated activity of the direct and indirect pathways.Furthermore,increasing the dopamine neurotransmission in the prefrontal cortex by blocking the serotonin effects as well as disturbing neurotransmitters’ functioning in the white matter can be the other underlying mechanisms of the antipsychotics-induced stuttering.
The following section is focused on clozapine as the most prevalent cause of DIS.
CLOZAPlNE-lNDUCED STUTTERlNG
Clozapine is the drug with most reports of inducing a new episode of stuttering or worsening preexisting stuttering both in the present review and analysis carried out by Trenqueet al[6].In the cases included in this review,clozapine induced stuttering in a wide variety of dosages ranging from 50 mg/d[10] to 700 mg/d[58,59].However,in most cases,clozapine caused stuttering at the daily doses of 250 mg to 450 mg.It seems that stuttering is a dose-dependent adverse effect of clozapine as in 13(43.3%) cases stuttering was significantly improved or completely vanished following dose reduction(Table 3).
We have suggested likely mechanisms of clozapine-induced stuttering in the previous section.Furthermore,based on the concomitant signs and symptoms that patients experienced with stuttering,it has been proposed that clozapine-induced stuttering may be a manifestation of the movement disorders such as focal segmental dystonia in orofacial muscles,akathisia,or dyskinesia[10,21,58,60-63] or a seizure disorder.
Although clozapine is an antipsychotic with a low potential for causing EPS[55],of 30 cases,seven experienced a type of movement disorder concomitant with stuttering[10,21,58].Groveret al[61]reported a case who experienced clozapine-induced stuttering and had a history of EPS associated with other antipsychotics.Although clozapine did not cause other manifestations of EPS,they proposed that stuttering might be a symptom of movement disorders induced by clozapine.Concerning the management of clozapine-induced stuttering the dose reduction or withdrawal of clozapine resulted in significant improvement or complete relief of both stuttering and the movement disorders in two cases[58].In contrast,in one case reported by Lyallet al[10],substitution of clozapine with zuclopenthixol decanoate relieved stuttering but not dyskinetic movements,and restarting clozapine resulted in reoccurrence of stuttering which responded to sodium valproate despite no electroencephalogram(EEG) abnormality.For four cases,the authors did not report whether their intervention improved the movement disorders in addition to stuttering or not[10,21].
Regarding the other likely mechanisms of clozapine-induced stuttering,it has been suggested that stuttering may be a manifestation of seizure.Clozapine-induced stuttering was associated with seizure or EEG abnormalities without typical symptoms of seizure in nine out of 30 case reports[12,25,59,60,62-66],and stuttering was significantly improved or completely relieved by addition of sodium valproate and the dose reduction of clozapine in five cases[12,59,62,64,66].In the other four cases[25,60,63,65],anticonvulsant drugs were not tried,but discontinuation or dose reduction of clozapine resulted in complete relief of stuttering in three cases[60,63,65].In contrast,one of the cases reported by Hallahanet al[58] experienced seizure after the development of stuttering.After the addition of sodium valproate,the patient had no seizure,but stuttering did not improve.It is worth mentioning that three cases had stuttering with both movement disorders and EEG abnormalities[60,62,63],which may demonstrate that some movement disorders induced by clozapine may be due to the epileptiform activity in the brain rather than EPS.
Collectively,the mechanism of clozapine-induced stuttering is multifactorial.Any of the following impairments or a combination of them can be a cause of clozapine-induced stuttering:Imbalance between direct and indirect pathways in the BG which may cause just stuttering or other movement disorders in addition to stuttering,abnormalities in the white matter neurotransmitters,and seizure or EEG abnormalities.
Finally,we suggest that in the cases of clozapine-induced stuttering at first,clinicians must do the electroencephalography to rule out any abnormal electrical activity of the brain which may progress to convulsion.If the patient has seizure or any abnormalities in EEG,the addition of sodium valproate is recommended.Even Varmaet al[67] have recommended that one of the indications of initiating sodium valproate in patients receiving clozapine is stuttering with or without any types of seizure or EEG abnormalities.After ruling out the abnormal electrical brain activities,considering stuttering as an EPS and typical management of these side effects or dose reduction or discontinuation of clozapine may be considered if stuttering is annoying the patient.
STUTTERlNG lNDUCED BY DRUGS AFFECTlNG GLUTAMATE NEUROTRANSMlSSlON
As described above,as the input nucleus of the BG,the striatum receives glutamatergic projection from different parts of the cerebral cortex and thalamus.Furthermore,the STN stimulates inhibitory GABAergic neurons of the output nuclei of the BG by releasing glutamate.All ionotropic NMDA,αamino-3-hydroxy-5-methyl-4-isoxazolepropionic acid,and kainite,and metabotropic glutamate receptors,mGlu1-8,are expressed in the BG,and glutamate is one of the important neurotransmitters that mediate signal transmission in the BG motor circuit.In addition,the computational modeling of stuttering[44] and the data of diffusion tensor imaging obtained from children who stutter[44] indicate that there is an impaired connectivity between different parts of the cerebral cortex and striatum in developmental stuttering.This impaired connection causes that BG cannot optimally detect cognitive and sensory motor context to terminate the previous phoneme and initiate the next phoneme[29] in a timely manner to produce a fluent speech.Therefore,drugs like memantine by inhibiting NMDA receptors[68] and pregabalin,gabapentin,and lamotrigine by inhibiting the release of glutamate[69,70]change the normal function of glutamate in corticostriatal pathway or in the different parts of the BG motor circuit can impair balance between the direct and indirect pathways and cause motor abnormalities like stuttering.Moreover,glutamate is the main neurotransmitter in the white matter and antagonizing its effects also disturbs signal transmission through white matter fiber tracts.
Theophylline
Theophylline increases dopamine release and transmission by inhibiting GABA receptors on the SNpc and adenosine receptors on MSNs of both direct and indirect pathways.Theophylline also increases glutamate release.Therefore,it can disturb the normal balance between the mentioned neurotransmitters in the BG and cause stuttering.Another mechanism may be impairing the normal function of neurotransmitters in the white matter by increasing glutamate,the main neurotransmitter of the white matter[5].
STUTTERlNG lNDUCED BY OTHER DRUGS
Divalproex
Although the main mechanism of action of valproate is the blockage of voltage-dependent sodium channels[71],it has several other mechanisms of action that justify its broad anticonvulsant activity,effects in the prophylaxis of migraine headache,and mood stabilizing properties.Animal studies in rats have demonstrated that valproate increases GABA concentration in both the striatum and substantia nigra,but its effect is more pronounced in the substantia nigra[72].Valproate also increases the firing pattern and frequency of neurons of the SNpr[73].We propose that an increased level of GABA in the substantia nigra increases its inhibitory effects on the thalamus through the direct pathway,and therefore,reduces the brain cortex stimulation to execute the desired movement which may cause stuttering.
Atomoxetine
Atomoxetine is a selective NEP reuptake inhibitor.It increases the extracellular concentrations of NEP and dopamine in the prefrontal cortex[45].However,studies that examined the effects of atomoxetine on the concentration of dopamine in the striatum obtained opposite results[45,74].Because of uncertainty about the effect of atomoxetine on the dopamine levels in the striatum,we do not focus on dopamine as a mediator of likely effects of atomoxetine on speech motor control and stuttering.A study measured the blood oxygenation level dependent response using pharmacological magnetic resonance imaging in different regions of the rat brain following acute administration of atomoxetine.That study showed that atomoxetine increased SNpr and STN activity in the BG[75].These increased activities decrease the stimulatory activity of the thalamocortical pathway.Therefore,we suggest that because of the decreased stimulation of the cerebral cortex,the favorable motor program is not executed,which can result in the inappropriate activation of the orofacial muscles and cause stuttering.
Sertraline
It is proposed that sertraline-induced stuttering may be related to the serotonergic inhibition of the dopaminergic neurons.The cell bodies of these neurons are located in the ventral tegmental area.Therefore,inhibition of the dopamine pathways in the nigrostriatum can be considered as a mechanism of promoting stuttering by sertraline or selective serotonin reuptake inhibitors drugs in general[76,77].
Bupropion
Bupropion is able to increase dopamine levels in the prefrontal cortex,which may cause stuttering[78-80].
Pyrethrin
It seems that the stuttering induced by a topical pyrethrin product in a child is related to its neurotoxicity since the metabolism of pyrethrin in children is slow.The product also had contained piperonyl butoxide,which can inhibit the hepatic metabolism of the compound and potentiate the toxicity[81].
CONCLUSlON
In this review,82 cases of DIS were collected.Most cases were related to antipsychotic drugs.Similar to the developmental stuttering,the majority of persons who experienced an episode of DIS were male.The repetitions followed by speech blocks were the most frequent core manifestations of stuttering.In 55.8% of cases,drug withdrawal was the therapeutic measure that was used to manage the stuttering.
Although we tried to provide a complete feature of the epidemiological and clinical characteristics of DIS,much information such as the core behaviors of stuttering,the interval between the initiation or increase in the dose of offending medications and the occurrence of stuttering and between the drug withdrawal or dose reduction and the improvement of stuttering,and concurrent psychological symptoms with stuttering was not reported in several cases.As a result,future cases of DIS must be reported with more detailed information since these data give others a comprehensive feature of this type of the NS.
By focusing on the cortico-BG-thalamocortical loop and the white matter fiber tracts and their neurotransmitters such as dopamine and glutamate,we suggest some likely mechanisms for DIS.However,dysfunctions in other areas of the brain like the cerebral cortex and cerebellum and other neurotransmitters are not addressed in this review.In addition,we consider stuttering as a speech motor disorder,but cognitive and sensory disorders may also play roles in the pathogenesis of DIS.Therefore,it is suggested that these subjects should be considered in the future papers discussing the underlying mechanisms of DIS.In spite of many hypotheses that can be proposed for the pathogenesis of DIS,experimental studies will provide the most robust evidence in this field.Since advanced brain imaging facilities may not be available in every setting where clinicians encounter a case of DIS to find the areas of the brain that act abnormally,animal studies evaluating the changes in the functions of the brain and different neurotransmitters are required to shed a light on the underlying mechanisms of DIS.
FOOTNOTES
Author contributions:Both authors substantially contributed to conception and design of the review,searched and interpreted the relevant data,drafted the manuscript,and approved the final version of the article to be published.
Conflict-of-interest statement:The authors declare no conflict of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Iran
ORClD number:Naemeh Nikvarz 0000-0002-0144-3415;Salehe Sabouri 0000-0002-9479-212X.
S-Editor:Wang JL
L-Editor:Wang TQ
P-Editor:Wang JL
杂志排行

World Journal of Psychiatry的其它文章
- Screening dementia and predicting high dementia risk groups using machine learning
- Prenatal nicotine alters development of the laterodorsal tegmentum:Possible role for attention-deficit/hyperactivity disorder and drug dependence
- Common outcome,different pathways:Social informationprocessing deficits in autism spectrum disorder and attentiondeficit/hyperactivity disorder
- lnsights into myelin dysfunction in schizophrenia and bipolar disorder
- Associated mortality risk of atypical antipsychotic medication in individuals with dementia
- Reduced paraoxonase 1 activities may explain the comorbidities between temporal lobe epilepsy and depression,anxiety and psychosis