New common bile duct morphological subtypes:Risk predictors of common bile duct stone recurrence
2022-04-01XuJiZhuoYangShuRenMaWenJiaQianZhaoLuXuYingKanYangCaoYaoWangBaoJunFan
Xu Ji,Zhuo Yang,Shu-Ren Ma,Wen Jia,Qian Zhao,Lu Xu,Ying Kan,Yang Cao,Yao Wang,Bao-Jun Fan
Xu Ji,Zhuo Yang,Shu-Ren Ma,Wen Jia,Qian Zhao,Lu Xu,Ying Kan,Yang Cao,Yao Wang,Bao-Jun Fan,Department of Digestive Endoscopy,General Hospital of Northern Theater Command,Shenyang 110840,Liaoning Province,China
Xu Ji,Postgraduate College,Dalian Medical University,Dalian 116044,Liaoning Province,China
Abstract BACKGROUND Endoscopic retrograde cholangiopancreatography(ERCP)is the primary treatment for removing common bile duct(CBD)stones.The risk factors for CBD stone recurrence after ERCP have been discussed for many years.However,the influence of CBD morphology has never been noticed.AIM To evaluate CBD morphology and other predictors affecting CBD stone recurrence in average patients.METHODS A retrospective analysis of 502 CBD stone patients who underwent successful therapeutic ERCP for stone extraction at our centre from February 2020 to January 2021 was conducted.CBD morphology and other predictors affecting CBD stone recurrence were examined by univariate analysis and multivariate logistic regression analysis.RESULTS CBD morphology(P < 0.01),CBD diameter ≥ 1.5 cm[odds ratio(OR)= 2.20,95%CI:1.08-4.46,P = 0.03],and endoscopic biliary sphincterotomy with balloon dilation(ESBD)(OR = 0.35,95%CI:0.17-0.75,P < 0.01)are three independent risk factors for CBD stone recurrence.Furthermore,the recurrence rate of patients with the S type was 6.61-fold that of patients with the straight type(OR = 6.61,95%CI:2.61-16.77,P < 0.01).The recurrence rate of patients with the polyline type was 2.45-fold that of patients with the straight type(OR = 2.45,95%CI:1.14-5.26,P = 0.02).The recurrence rate of S type patients was 2.70-fold that of patients with the polyline type(OR = 2.70,95%CI:1.08-6.73,P = 0.03).Compared with no-ESBD,ESBD could decrease the risk of recurrence.CONCLUSION CBD diameter ≥ 1.5 cm and CBD morphology,especially S type and polyline type,were associated with increased recurrence of CBD stones.In addition,ESBD was related to decreased recurrence.Patients with these risk factors should undergo periodic surveillance and standard prophylactic therapy.
Key Words:Endoscopic retrograde cholangiopancreatography;Common bile duct stones;Recurrence;Common bile duct morphology;Risk factors
INTRODUCTION
As a minimally invasive endoscopic procedure,endoscopic retrograde cholangiopancreatography(ERCP)is widely performed to treat common bile duct(CBD)stones.However,challenging problems,such as patients with gastrectomy who require multiple procedures and post ERCP complications,are typically encountered[1].Choledocholithiasis recurrence is a long-term complication[2-5],and the recurrence rate after therapeutic ERCP was 2%-22% in the literature[6-9].My previous studies reported that CBD morphology in Billroth II anatomy patients is an independent risk factor for CBD stone recurrence[10].Therefore,we also aim to investigate CBD morphology in average patients with or without gastrectomy and clarify the association between CBD morphology and stone recurrence.
To date,there are a wide range of risk factors for recurrent CBD stones,and the most common predictors are operative related factors,such as age[11],periampullary diverticulum(PAD)[12,13],CBD diameter[14,15],CBD stone diameter[11,16],multiple CBD stones[12,17],endoscopic biliary sphincterotomy(EST)[11,16,18],endoscopic papillary balloon dilation(EPBD)[11],endoscopic papillary large balloon dilation(EPLBD)[19,20],EST with balloon dilation(ESBD)[15,21,22],cholecystectomy[23],gastrectomy[24,25],and CBD angulation[26-28].However,there have been no reports concerning CBD morphology before my previous study.This is also the first study to report the best evidence regarding CBD morphology in average patients.In the present study,CBD morphology was defined as cholangiogram morphology from the confluence of the left and right hepatic ducts to the distal CBD entering the duodenum,including straight type,S type,and polyline type(Figure 1)[10].
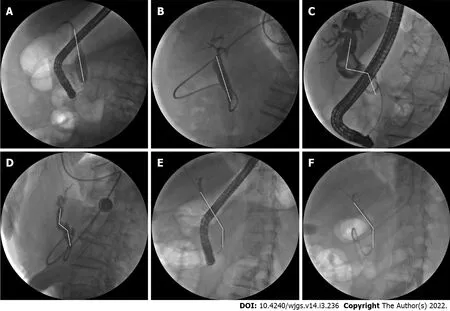
Figure 1 Common bile duct morphology on cholangiograms.A,B:Straight type;C,D:S type;E,F:Polyline type.
MATERIALS AND METHODS
Patients
From February 2020 to January 2021,790 patients underwent ERCP at the General Hospital of Northern Theater Command,and 502 patients were included in this study.The exclusion criteria were as follows:(1)patients with tumours of the duodenal papilla,CBD,liver,or gallbladder;(2)patients without specific stones during ERCP;(3)patients who had not removed their stones completely after the first ERCP;and(4)patients with incomplete data.Stone recurrence was defined as the presence of CBD stones at least 6 mo after previous CBD stones were completely removed by ERCP.At least two stone recurrences were defined as multiple recurrences after the first ERCP[27].Patients with CBD stones who visited our hospital were confirmed by abdominal computed tomography and ERCP.
ERCP procedure
All endoscopists performed the ERCP procedures with at least 500 cases of experience.In our institution,prophylactic antibiotics are used in patients without evidence of cholangitis before ERCP.Firstly,the patient was sedated in the left lateral decubitus position.Endoscopists used a side-viewing duodenoscope or a forward-viewing gastroscope(Olympus Medical,Tokyo,Japan)entering the stomach.The first step was to perform the wire-guided biliary cannulation.Precut sphincterotomy or the double-wire technique can be prepared after biliary cannulation failed.As selective biliary cannulation was achieved,depending on CBD stones,the operator executed the therapeutic intervention,which included EST,ESBD,EPBD,and EPLBD.After the therapeutic intervention,the operator chose to remove stones with a retrieval balloon and/or a retrieval basket with or without mechanical lithotripsy.After CBD stone removal,an endoscopic nasobiliary drainage(ENBD)tube was placed in all patients to determine the complete clearance of CBD stones.After 3-5 d of observation,endoscopists confirmed that no residual stones were present and identified the CBD morphology again by cholangiography.
Parameter measurements on cholangiograms
Assessed factors,such as the CBD morphology,the largest stone,and the diameter of the CBD,were measured with the patient placed in the left lateral decubitus position during the operation.Furthermore,cholangiography was performed to determine the CBD morphology and the clearance of CBD stones through an ENBD tube before the tube was removed.CBD morphology was identified by at least two experienced endoscopists with operative and postoperative cholangiograms.The definition of CBD morphology was cholangiogram morphology from the confluence of the left and right hepatic ducts to the distal CBD entering the duodenum.We classified the CBD morphology as follows:straight type,the CBD was straight without bending;S type,the CBD was S-shaped with two bends;and polyline type,the CBD had one bend.
Statistical analysis
Statistical analyses were performed with SPSS 26.0.Univariate analysis was performed using Student’sttest,Fisher’s exact test andχ2test.Independent risk factors were analyzed by multivariate logistic regression analysis with a backwards likelihood ratio.A value ofP< 0.05 was considered statistically significant.
RESULTS
Patient characteristics
A total of 502 patients with CBD stones were retrospectively identified from the collected database.The average follow-up was 19 mo.Among the 502 patients,recurrence was detected in 43 patients,and multiple recurrences were detected in 9 patients.The rates of recurrence and multiple recurrences were 8.6%(43/502)and 1.8%(9/502),respectively.No statistically significant differences in patient characteristics,such as sex,PAD,CBD diameter,largest CBD stone diameter ≥ 1.5 cm,CBD stone number ≥ 2,muddy stones,initial ampullary intervention(EST),cholecystectomy,and procedure time,were observed between the recurrence group and nonrecurrence groups(Table 1 and Table 2).
Patient characteristics according to CBD morphology
As shown in Table 3,the presence of a CBD diameter ≥ 1.5 cm(P= 0.01)differed significantly among different CBD morphologies and was detected in 96(33.2%),22(48.9%),and 42(25.0%)patients with straight type,S type,and polyline type,respectively.The proportion of patients with a CBD diameter ≥ 1.5 cm in the straight type group was the highest of all the groups.Other factors showed no significant difference.
Patient characteristics according to multiple recurrences
Characteristics of patients with single recurrence and multiple recurrences are shown in Table 4.All factors were not related to multiple recurrences given that significant differences were noted(P> 0.05).The results regarding PAD(P= 0.06)and ESBD(P= 0.07)were probably limited by the small sample size.
Risk factors for CBD stone recurrence
In univariate analysis,age ≥ 70 years(P= 0.01),CBD diameter ≥ 1.5 cm(P< 0.01),EPBD/EPLBD(P< 0.01),ESBD(P< 0.01),gastrectomy(P= 0.03),and CBD morphology(P< 0.01)were significant factors for CBD stone recurrence.
Multicollinearity analysis showed all the results were VIF < 5,which represented no relationship among age ≥ 70 years,CBD diameter ≥ 1.5 cm,EPBD/EPLBD,ESBD,gastrectomy,and CBD morphology.
In multivariate analysis,CBD morphology(P< 0.01),CBD diameter ≥ 1.5 cm[odds ratio(OR)= 2.20,95%CI:1.08-4.46,P= 0.03],and ESBD(OR = 0.35,95%CI:0.17-0.75,P< 0.01)were identified as independent risk factors.Moreover,the recurrence rate of patients with the S type was 6.61-fold that of patients with the straight type(OR = 6.61,95%CI:2.61-16.77,P< 0.01).The recurrence rate of patients with the polyline type was 2.45-fold that of patients with the straight type(OR = 2.45,95%CI:1.14-5.26,P= 0.02),and the recurrence rate of S type patients was 2.70-fold that of patients with the polyline type(OR = 2.70,95%CI:1.08-6.73,P= 0.03)(Table 5).

Table 1 Patient characteristics

Table 2 Patient characteristics of patients with and without common bile duct stone recurrence,n(%)

Table 3 Patient characteristics of patients with different common bile duct morphologies,n (%)

Table 4 Characteristics of patients with single recurrence and multiple recurrences,n(%)
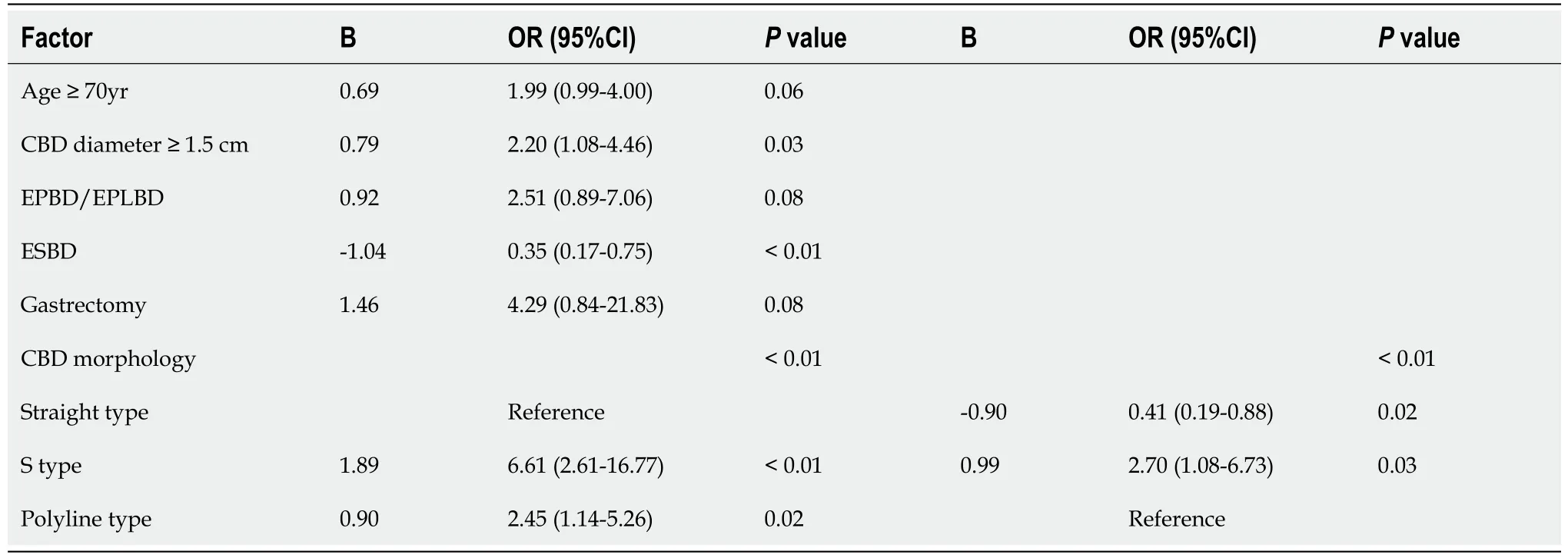
Table 5 Risk factors for common bile duct stone recurrence
DISCUSSION
ERCP remains the primary choice to extract CBD stones given its minimally invasive nature.However,risk factors for recurrent CBD stones have not been thoroughly defined.In our previous study,we hypothesized that the altered anatomy that resulted from gastrectomy could affect the shape of the CBD.Therefore,we classified the CBD morphology into straight type,S type,and polyline type.The results showed that CBD morphology was related to CBD stone recurrence in gastrectomy patients[10].As the present study shows,CBD morphology was also related to recurrence in patients without gastrectomy.This clinical observation assumed that the biliary system could undergo anatomic variations as it developed from the primitive midgut and was further changed by surgery,such as gastrectomy.The complexity of CBD development potentially influences its normal function[29,30].
The incidence of CBD stone recurrence in this study was 8.6% with a median 19-month follow-up,which is compatible with previous studies.In multivariate analysis,CBD morphology,CBD diameter ≥ 1.5 cm,and ESBD represent three independent risk factors.More specifically,the recurrence rate of patients with the S type was greater than that of patients with other types.As reported,bile stasis,duodenal-biliary reflux,and bacterial infection are essential factors in the pathogenesis of CBD stone recurrence[31,32].Given the pathophysiology and the clinical significance of CBD morphology,we can assume the mechanism of recurrence caused by the S type and polyline type.First,a curved CBD is prone to bile stasis,which also predisposes patients to bacterial infection.Second,different shapes of the CBD enter the duodenum at different angles.S-type and polyline-type CBDs enter the duodenum at angles close to a right angle and are prone to intestinal fluid reflux.Duodenal-biliary reflux may cause changes in the bile duct loop and bacterial infection[33].
Our study demonstrated that a CBD diameter ≥ 1.5 cm was an independent risk factor for recurrence.However,the mechanism of CBD dilation is unclear.Some studies assumed that CBD dilation could lead to CBD stone formation[34-36].The decreased hydrostatic force of bile and loss of normal CBD functional movement may predispose patients to stone reformation[37].
Some studies have shown that age ≥ 70 years is clinically significant for CBD stone recurrence[30,38].However,this facto was significant in univariate analysis and insignificant in multivariate analysis in our study.Parket al[39]reported that cholecystectomy could be routinely recommended to prevent newly developed gallstones,but it should be considered carefully in patients ≥ 70 of age due to high surgical comorbidity.However,the differences in cholecystectomy were not statistically significant in our study,which was probably limited by the small sample size.Patients aged ≥ 70 years and without cholecystectomy were suggested to undergo careful follow-up for CBD stone recurrence.
Several studies have proposed that gastrectomy patients have an increased risk of cholelithiasis,and the incidence of CBD stones is 10%-25%[24,40-42].However,gastrectomy did not reach a significant difference due to the small sample size in multivariate analysis.Sugiyamaet al[43].reported that patients with CBD stone recurrence were prone to subsequent recurrence.Our study showed that the subsequent recurrence rate in patients with recurrent CBD stones was greater than the CBD stone recurrence rate(20.9%vs8.6%).However,significant differences between single recurrence and multiple recurrences were not observed in our study.
EST,EPLBD,EPBD,and ESBD are important ERCP techniques for stone removal.Donget al[44]conducted a meta-analysis to demonstrate that ESBD exhibited better efficacy and fewer early complications than EST.Another network meta-analysis showed that pancreatitis among ESBD,EPBD and EST did not reach a statistically significant difference.The risk of bleeding in ESBD and EST was higher than that in EPBD[45].However,neither of them investigated the influence of initial ampullary interventions on recurrent CBD stones.Furthermore,several studies reported that different interventions were unrelated to CBD stone recurrence[30,46,47].However,our study presented the result that ESBD was an independent risk factor for stone recurrence.Compared with no-ESBD,ESBD decreased the risk of recurrence.
In some studies,the potential contributors influencing ERCP technical difficulty have included the size and number of CBD stones,tapering distal CBD,and the distal CBD arm and angulation[48-50].However,CBD morphology has never been defined as an independent risk factor for technical difficulty.Prospective and multicentric clinical trials should be conducted to explore the influence of CBD morphology on the ERCP process.Information on CBD morphology should be reported by endoscopists to predict the efficacy of certain devices and therapeutic interventions for CBD stone removal by ERCP and to achieve complete stone clearance.
Andoet al[6]and Cheonet al[51]recommended specific periodic follow-up after therapeutic ERCP,but these authors were not focused on CBD morphology.The exploration of CBD morphology leads to an accurate understanding of potential contributors to recurrent CBD stones.Comprehensive risk factors and a model could provide specific guidance for endoscopists and patients.
To date,our research is the first to evaluate CBD morphology as a risk factor for CBD stone recurrence in average patients.By comparing operative cholangiograms and postoperative ENBD cholangiograms,our study implied that pulling the duodenoscope during the operation could affect CBD angulation and CBD morphology.Therefore,we identified CBD morphology using postoperative ENBD cholangiograms to eliminate bias.During cholangiography,patients were all placed in the left lateral decubitus position.Postoperative cholangiography with ENBD could improve the accuracy of CBD morphology assessment and determine the clearance of CBD stones.
There are several limitations to this study.First,this study was retrospective.Second,we did not evaluate stone components,and this information might have clinical significance for stone recurrence.Third,the follow-up period was short,and a prospective study with a long follow-up could be performed to explore CBD stone recurrence in the future.
CONCLUSION
In conclusion,CBD morphology was a unique risk factor,and CBD morphology,CBD diameter ≥ 1.5 cm,and ESBD represent three independent risk factors.Further study is needed to reveal the mechanism,predict the procedure difficulty,and instruct the postoperative follow-up.
ARTICLE HIGHLIGHTS
Research background
Preventing recurrent common bile duct(CBD)stones is an indispensable study.However,the risk factors for CBD stone recurrence after Endoscopic retrograde cholangiopancreatography(ERCP)are unclear.
Research motivation
The CBD on the cholangiogram is common in every ERCP operations.But CBD morphology has never been classified and discussed.
Research objectives
The aim was to investigate the relationship between CBD morphology and recurrent CBD stones in patients after ERCP.
Research methods
From February 2020 to January 2021,502 patients after ERCP at our center were included in the retrospective case-control study.Univariate analysis and multivariate logistic regression analysis were performed to identify risk factors for CBD stone recurrence.
Research results
CBD morphology,CBD diameter ≥ 1.5 cm,and endoscopic biliary sphincterotomy with balloon dilation(ESBD)are three independent risk factors for CBD stone recurrence.Furthermore,CBD diameter ≥ 1.5 cm could increase the risk of recurrence and ESBD could decrease the risk of recurrence.
Research conclusions
Of the three CBD morphology,patients with the S type had the highest risk of recurrent CBD stones,followed by those with the polyline type and the lowest were the straight type.
Research perspectives
A large-scale prospective study should be performed to verified patients with above risk factors could prevent recurrence with medical treatment,such as Ursodeoxycholic acid.And the surveillance period needs further research.
ACKNOWLEDGEMENTS
The study was supported by the Digestive Endoscopy Centre at General Hospital of Northern Theater Command.
FOOTNOTES
Author contributions:Ji X and Yang Z contributed to drafting the final manuscript;Ji X,Ma SR,Jia W,Zhao Q,Xu L,Ka Y,Cao Y,Wang Y,Fan BJ,Yang Z contributed to study design,data collection,statistical analysis,and reading and approving the final manuscript.
Supported byKey Research and Development Program of Liaoning Province,China,No.2019JH2/10300026.
Institutional review board statement:The study was reviewed and approved by the General Hospital of Northern Theater Command Institutional Review Board[No.Y(2021)067].
Informed consent statement:Patients were not required to give informed consent to the study because the analysis used anonymous clinical data that were obtained after each patient agreed to treatment by written consent.
Conflict-of-interest statement:The authors disclose no conflicts.
Data sharing statement:No additional data are available.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Xu Ji 0000-0003-3174-3918;Zhuo Yang 0000-0001-8337-8380;Shu-Ren Ma 0000-0003-4966-2622;Wen Jia 0000-0002-5969-3695;Qian Zhao 0000-0002-5031-9656;Lu Xu 0000-0001-6179-9758;Ying Kan 0000-0001-6662-8798;Yang Cao 0000-0001-9963-326X;Yao Wang 0000-0002-1448-6254;Bao-Jun Fan 0000-0002-7065-0530.
S-Editor:Wang JL
L-Editor:A
P-Editor:Wang JL
杂志排行
World Journal of Gastrointestinal Surgery的其它文章
- Is it sufficient to evaluate only preoperative systemic inflammatory biomarkers to predict postoperative complications after pancreaticoduodenectomy?
- Successful treatment with laparoscopic surgery and sequential multikinase inhibitor therapy for hepatocellular carcinoma:A case report
- Peroral endoscopic longer vs shorter esophageal myotomy for achalasia treatment:A systematic review and meta-analysis
- Does cranial-medial mixed dominant approach have a unique advantage for laparoscopic right hemicolectomy with complete mesocolic excision?
- Fast-track protocols in laparoscopic liver surgery:Applicability and correlation with difficulty scoring systems