Clinical efficacy of the Ankle Spacer for the treatment of multiple secondary osteochondral lesions of the talus
2022-03-05JariDahmenNienkeAltinkGwendolynVuurbergCoenWijdicksSjoerdASStufkensGinoMMJKerkhoffs
lNTRODUCTlON
Osteochondral lesions of the Talus(OLT)are pathologic lesions of the talar cartilage and the subchondral bone.These lesions can occur in up to 50% of acute ankle fractures and sprains[1].For OLTs of larger size(above 10 or 15 mm in diameter)and of non-fragmentous morphology,the‘standard’ operative treatment options such as autologous chondrocyte implantation,osteochondral autograft transfer systems,and a Talar OsteoPeriostic grafting from the Iliac Crest procedure may result in satisfactory clinical outcomes[2-4].However,in some patients,there are multiple secondary lesions present of large and cystic nature.For these lesions,it is not always possible to harvest an osteo(chondral)autograft that is large enough to replace all the diseased osteochondral tissue of the talus without damaging the donor site or compromising the congruency of the ankle joint.Allograft treatment could be considered for the treatment of these type of lesions.However,these contain the disadvantages of loss of viability and stability in one-third of the grafts,and possibly clinically fail due to immunological reactions[5,6].However,when there are multiple secondary(failed prior surgery)lesions present on the talar articular surface in combination with a large and cystic nature,the abovedescribed operative interventions are to be expected to result in relatively inferior outcomes.
To avoid inferior surgical outcomes in patients with persisting complaints after previous unsuccessful conservative management and operative therapy,other effective operative interventions are performed including an ankle arthrodesis or a total ankle prosthesis[7-9].An(arthroscopic)ankle arthrodesis results in satisfactory clinical outcomes mostly concerning pain[10-12].However,the operative intervention in question can result in functional limitations due to loss of the range of motion(ROM)of the ankle[13].Furthermore,an ankle arthrodesis may potentially result in an increased long-term risk of arthritis in adjacent hindfoot joints,particularly the subtalar joint[14].An alternative option is the placement of a total ankle prosthesis,for which a substantial amount of bone needs to be resected[15].In order to address the problem of decreased joint motion(in the case of an ankle arthrodesis)and major bone resection(in the case of a prosthesis),a one-piece hemi-arthroplasty covering the talar surface,and leaving the tibia plafond untouched,can be a potential solution to the aforementioned challenges.
Although previous operative interventions similar to such a hemi-arthroplasty have been described in the literature,the studies applied operative techniques with resection of a substantial part of the talar cortical bone and cartilage in order to verify fitting of the implant thereby taking away a potential successful ankle arthrodesis in case of clinical failure[16-18].Consequently,a novel bone-sparing hemiprosthesis has been developed(The Ankle Spacer)to enable resurfacing of the talar dome and simultaneously preserving the ROM and potentially optimize physical functioning.Potential advantages include preservation of ankle motion,decreased stress on the midfoot and subtalar joints,and the possibility to perform an ankle fusion after failed hemi-arthroplasty.Up to now,no operative technique description combined with the first clinical outcomes has been described in the literature.It is therefore the purpose of the present study to describe the operative technique and the clinical efficacy of the Ankle Spacer for the treatment of multiple,cystic OLTs in patients with failed prior operative treatment.Despite the fact that no clinical trials have been published on this specific implant,it is hypothesized that the 2-year postoperative follow-up will show a clinically relevant pain reduction and prosthesis survival.
MATERlALS AND METHODS
Study design
The study concer ns a non-randomized,non-blinded,non-comparative prospective trial,with a 2-year follow-up period at the outpatient clinic aiming at assessing pain,function and implant survival,and thereby investigating the clinical efficacy of the Ankle Spacer.The study was approved by the local Medical Ethics Committee(Internal Review Board,IRB)of the Amsterdam University Medical Centre with reference number MEC 2017_175 and was performed in accordance with the principles of the Declaration of Helsinki and the medical Research Involving Human Subjects Act.The study was sponsored by Arthrex as a post market study with reference number EMEA-17037.
The Ankle Spacer showed clinically relevant pain reduction during walking,improvement in clinical outcomes as assessed with PROMs,and no complications or re-operations.This treatment option may therefore evolve as a joint-sparing alternative to an ankle arthrodesis,a total talar implant or a total ankle arthroplasty/resurfacing.
Patient selection
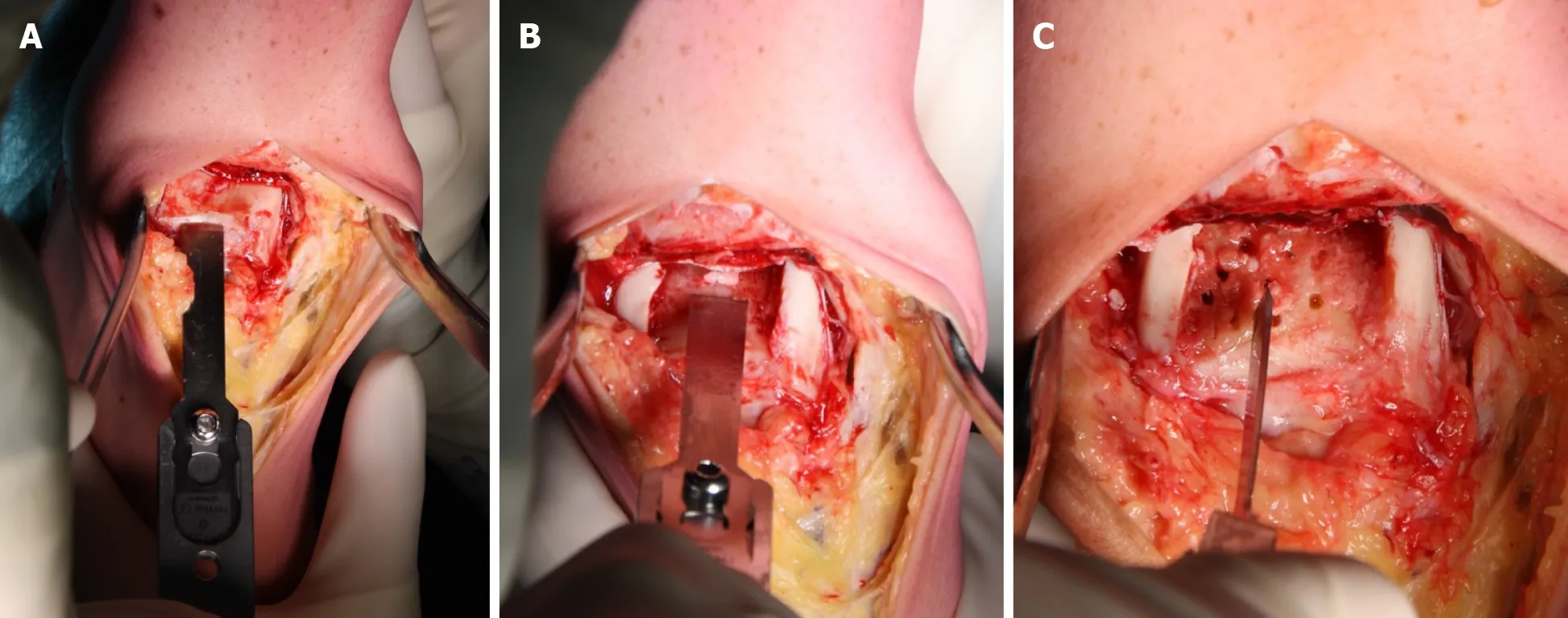
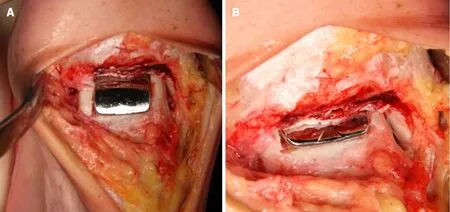
Before receiving the Ankle Spacer,the patient received 2 g of cefazoline pre-operatively.The procedure was carried out under general anesthesia.The patient was placed in the supine position with a tourniquet applied around the thigh and a rolled-up apron underneath the lateral malleolus to facilitate eversion of the foot to improve exposure of the talus.A longitudinal incision between 10 and 15 cm was centered over the ankle immediately lateral to the tibialis anterior tendon.The incision was deepened to the ankle joint while retracting the extensor hallucis longus and the neurovascular bundle laterally.If present,the osteophytes on the anterior tibia edge were removed.Subsequently,the cartilage wasremoved(Figure 3A)on the upper talar surface as well as part of the underlying subchondral bone(Figure 3B).
This night also he was awakened by the same sounds as before, and in the morning they found, near the stream, the most beautiful cow-house that ever was seen, with stalls and milk-pails and stools all complete, indeed, everything that a cow-house could possibly want, except the cows
Timeframe and outcome assessment
My children, I feel that I am growing odd and weak, and that I shall not live long. Before I die I should like to build a house for each of you, as this dear old sty in which we have lived so happily will be given to a new family of pigs, and you will have to turn out. Now, Browny, what sort of a house would you like to have?
Description of the device
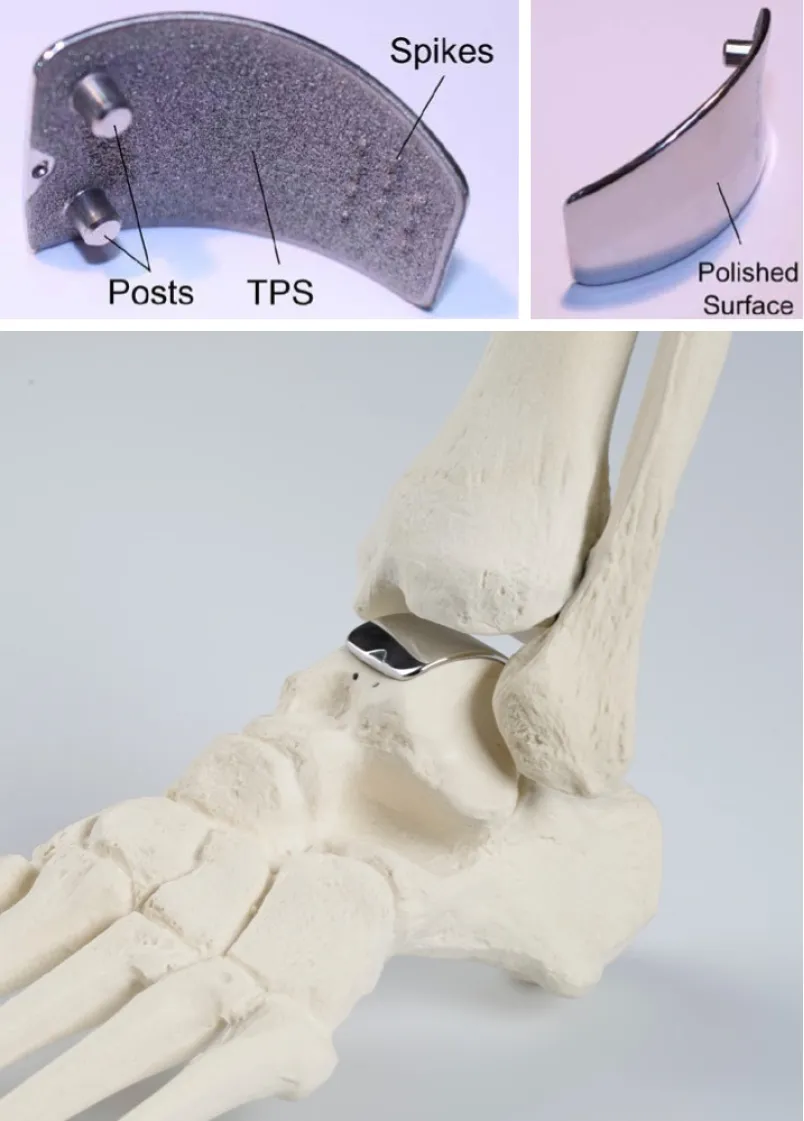
The Arthrex Ankle Spacer is a one-piece implant system that replaces the talar side of the tibio-talar joint(Figure 2).The Ankle Spacer replaces the articulating upper surface of the talus and offers several implant sizes in millimeters(18,20,22,24,26,28)in order to fit to the different sizes of the talus.It is anatomically designed to the native talar dome to provide an optimal fit to the distal articular tibial surface.The implant is polished to a mirror effect on the articulating surface and has a rough titanium plasma spray(TPS)coated under surface with two posts and spikes for implant fixation(US10,350,079 B2).The rough surface enables secondary fixation due to bone ingrowth.Spikes at the posterior part of the prosthesis allow for further fixation to the bone.The weight of the ankle spacer weighs varies from 11 to 22 g,depending on the size of the spacer.
That is a sensible little pig, replied his mother, looking fondly at him. I will see that the three houses are got ready at once. And now one last piece of advice. You have heard me talk of our old enemy the fox. When he hears that I am dead, he is sure to try and get hold of you, to carry you off to his den11. He is very sly and will no doubt disguise himself, and pretend to be a friend, but you must promise me not to let him enter your houses on any pretext12 whatever.
Operative technique
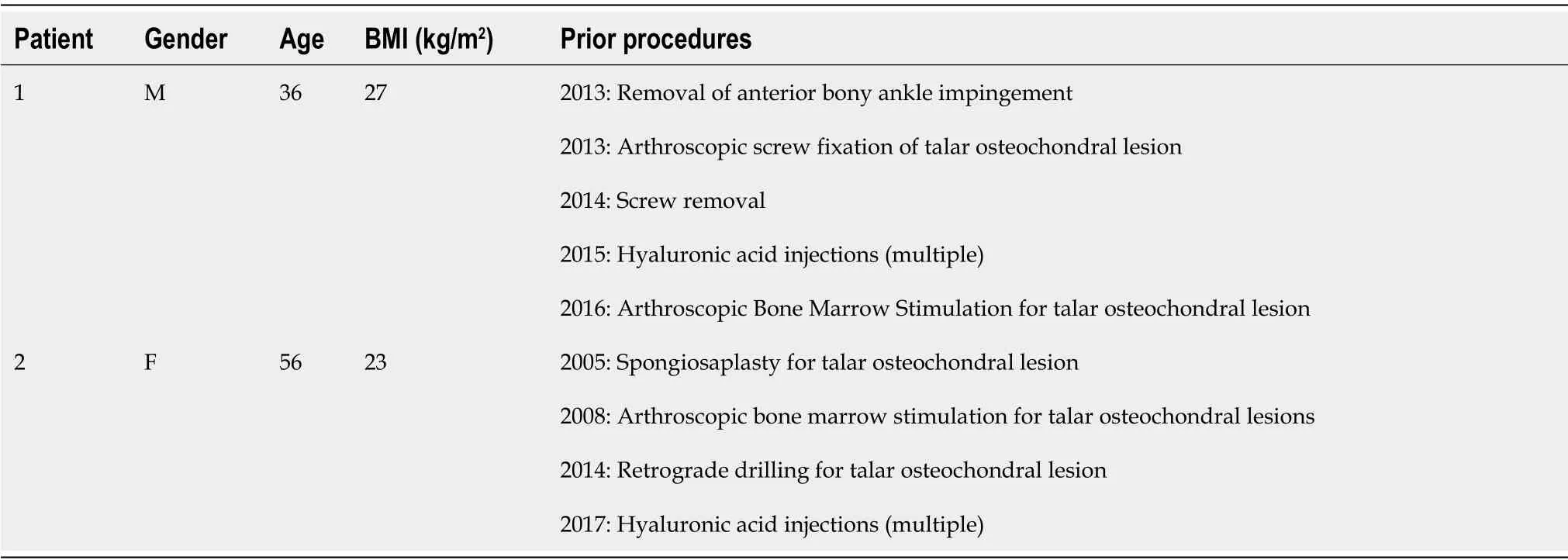
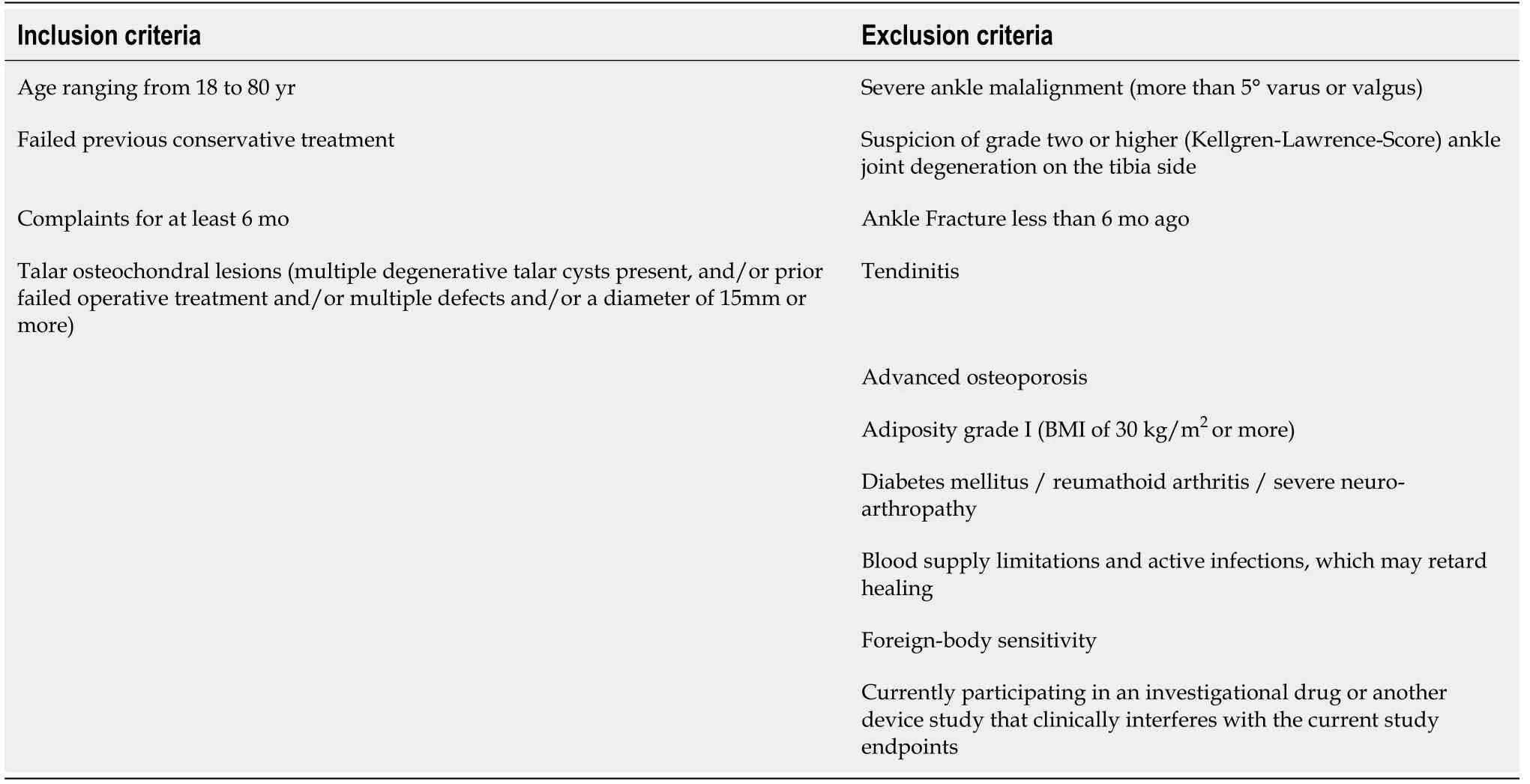
All patients eligible for operative implantation of the Ankle Spacer visiting the outpatient clinic between March 2017 and March 2019 for an OLT with a diameter of 15mm or more(anterior-posterior or mediallateral),an OLT that failed prior operative intervention(s)or patients with multiple OLTs on the talar dome surface,were requested if they were willing to participate in the present clinical trial.If they were interested,patients were informed about this study and were given two wk to decide upon participation.In case patients provided their consent,they were screened for meeting the inclusion and exclusion criteria(Table 1).
Additionally,microfracturing was performed to support ingrowth for secondary ankle spacer fixation(Figure 3C).
The double drill sleeve was aligned to the two holes on the Ankle Spacer and were maintained in a perpendicular angle relative to the surface of the ankle spacer.Subsequently,drilling was started with the first drill until the moment it stopped on the drill sleeve.This first drill was left for fixation in the drill hole,and then the second drill was to drill the second hole,in exactly the same manner.
Then,dynamic dorsi-and plantarflexion of the ankle was performed as this allowed self-alignment of the temporarily fixed trial.Afterwards,the trial spacer was fixated with a K-wire in the second hole in order to prevent dislocation,after which both K-wires were advanced bi-cortically in order to achieve proper fixation.Fluoroscopy was used to confirm proper sizing and positioning of the trial Ankle Spacer.
After supper, they returned as they had come to the ebony room, where he was compelled to look on while his companions played interminable games of chess, and not until he was nearly dying of weariness did they, slowly and ceremoniously as before, conduct him to his sleeping apartment
The tibiotalar joint was manually distracted and the appropriate trial Ankle Spacer was inserted into the joint.The trial Ankle Spacer was placed in a central position in the medial-lateral direction.The trial was fixated in the slotted hole with a K-wire and the trial inserter was removed afterwards.
Good people, you who are reaping, if you do not tell the King that all this corn belongs to the Marquis of Carabas, you shall be chopped as small as herbs for the pot.
Then all instruments were removed.Prior to inserting the Ankle Spacer,the prepared bone bed was thoroughly cleaned and inspected.The Ankle Spacer was inserted on the talar dome using the ankle space inserter,while placing the two posts on the bottom of the Ankle Spacer into the prepared drill holes for fixation.The implant was impacted with an impactor until the posts were fully seated in the drill holes(Figure 4A and Figure 4B).The joint capsule was closed and the layers were closed subsequently.
Post-operative protocol
Postoperatively,wound dressing with adequate padding was applied.At hospital discharge a removable lower leg splint was applied.Careful active and passive dorsi-and plantarflexion motion(flexion-extension exercises)without weight bearing monitored by a physiotherapist were started two days after surgery.After two wk of non-weight bearing,depending on the degree of wound and soft tissue healing,mobilization was started with progressive weight bearing to tolerance in a Walker.Flexion-extension exercises were continued.Six wk after surgery,intensive physiotherapy and rehabilitation was started for at least a period of 6 wk.
Power calculation and study population
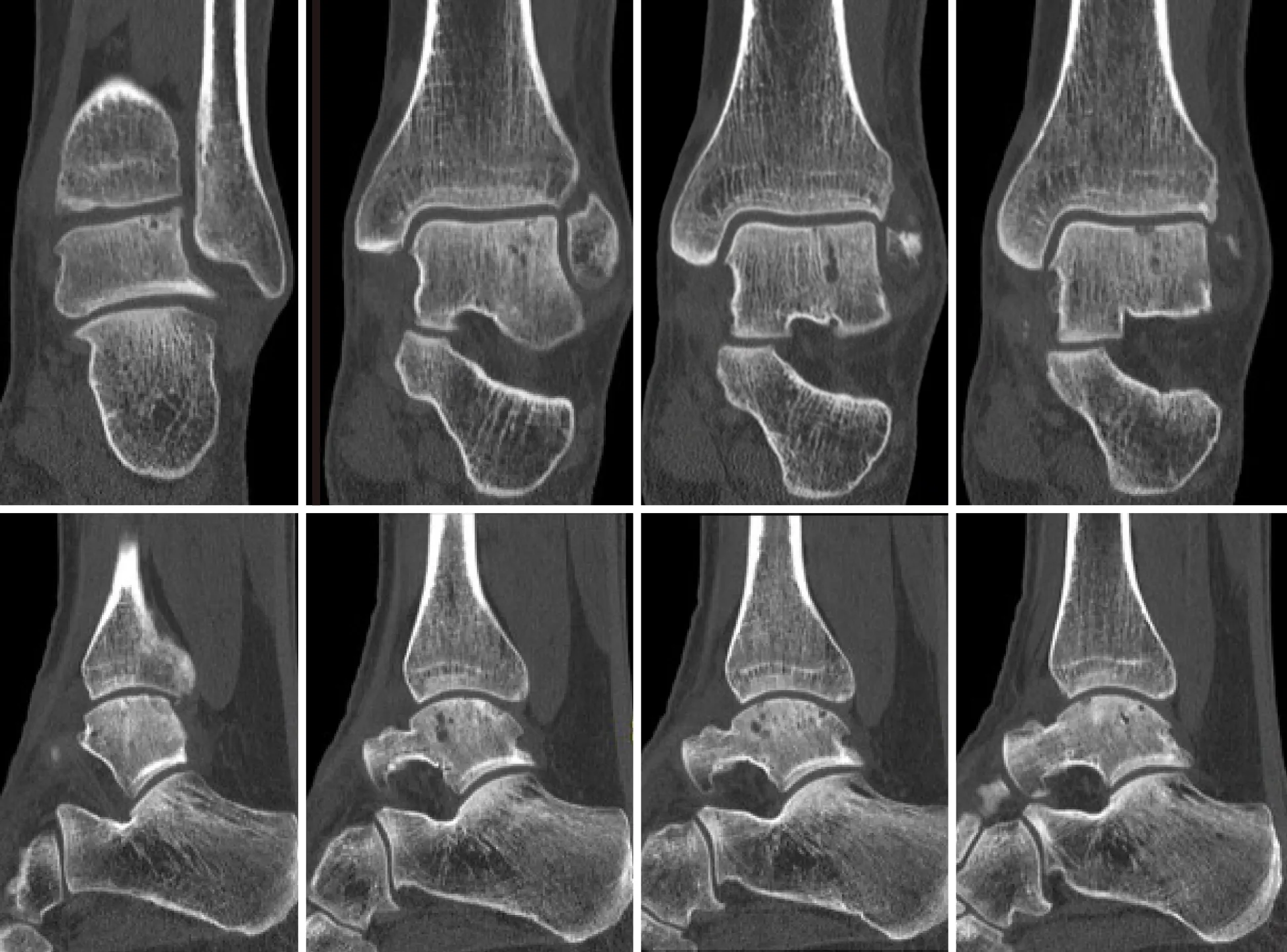
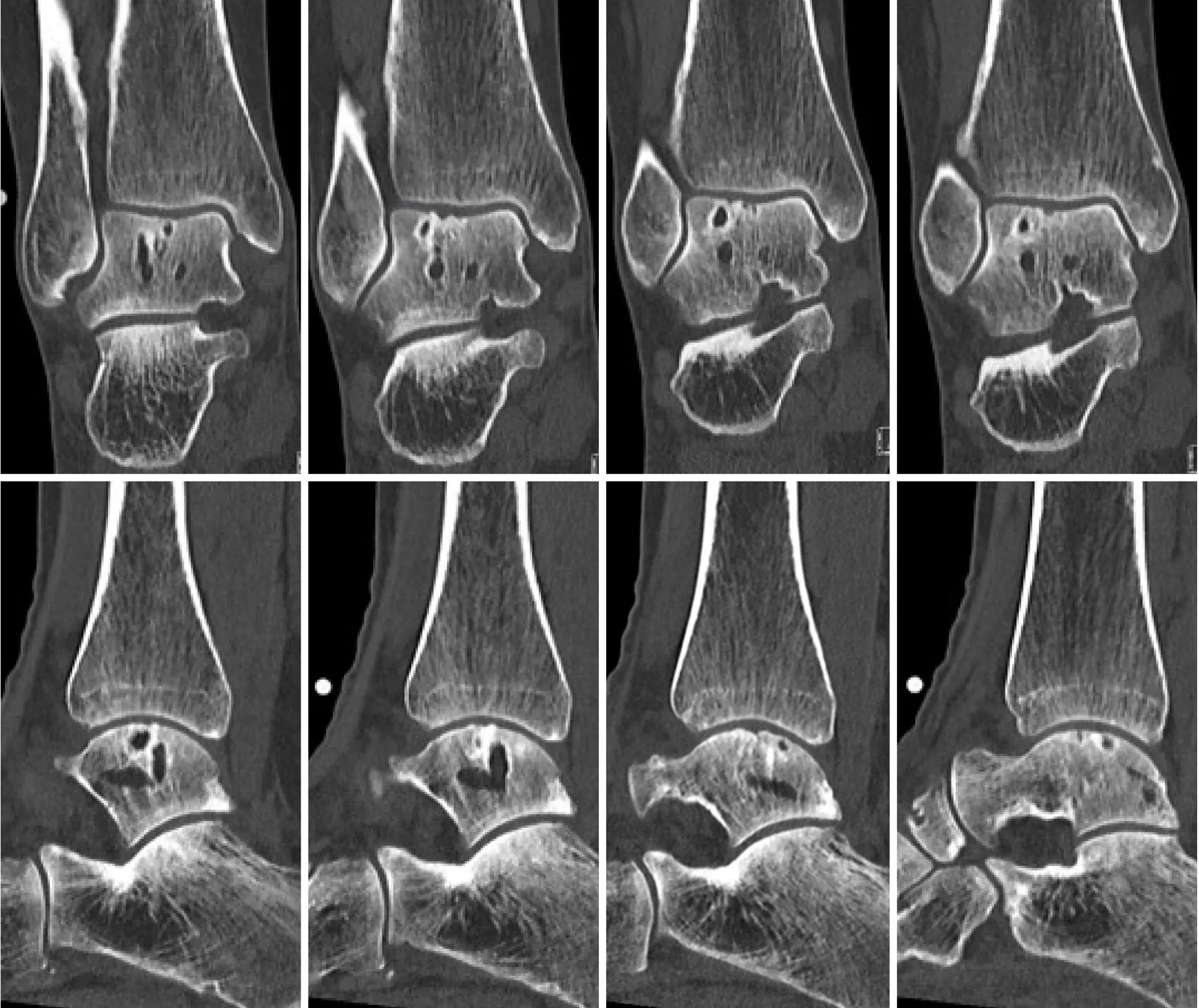
A power analysis was conducted to estimate the needed sample size for this prospective noncomparative trial using the NRS for pain as primary outcome measure with a clinical relevant difference of 1 point and a standard deviation of 1.5 points.Additionally,in this calculation a standard p-value of 0.05(α = 0.05)and a power of 80% were used.This indicated that a total of 20 patients would need to be included in the trial in order to detect a clinically important difference in pain comparing pre-and postoperative NRS scores.Due to the relative rarity of patients presenting at our outpatient department with the exact above-described inclusion and exclusion criteria,two patients could be identified with fitting indications who were operated on with the implantation of the Ankle Spacer.The age of these patients was 36 and 56 years old(one male,one female).No patients were lost to follow-up.Prior procedures that were performed are listed in Table 2 alongside demographic factors.The pre-operative CT scans of the patients as presented in Figures 5 and 6.
Statistical analysis
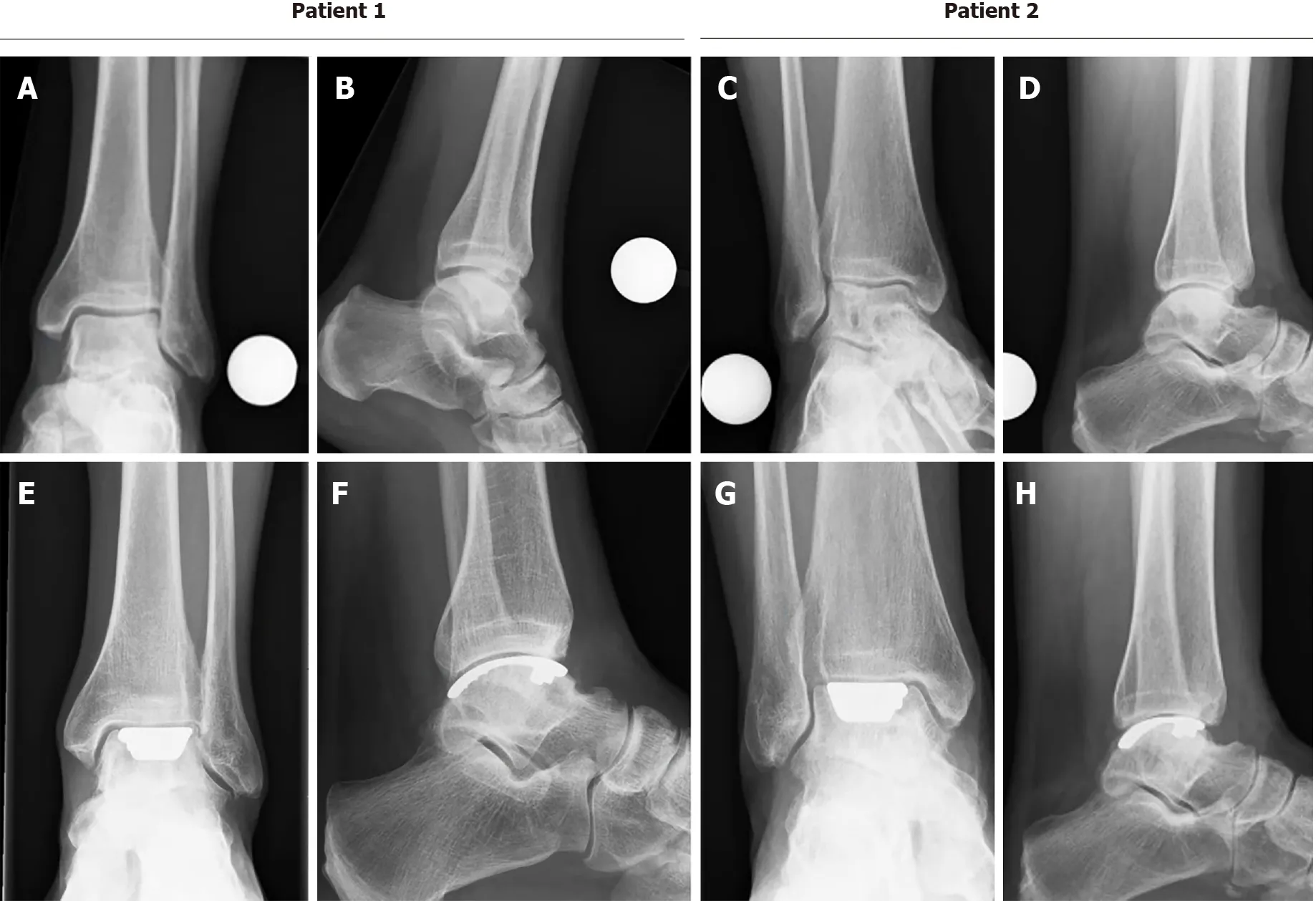
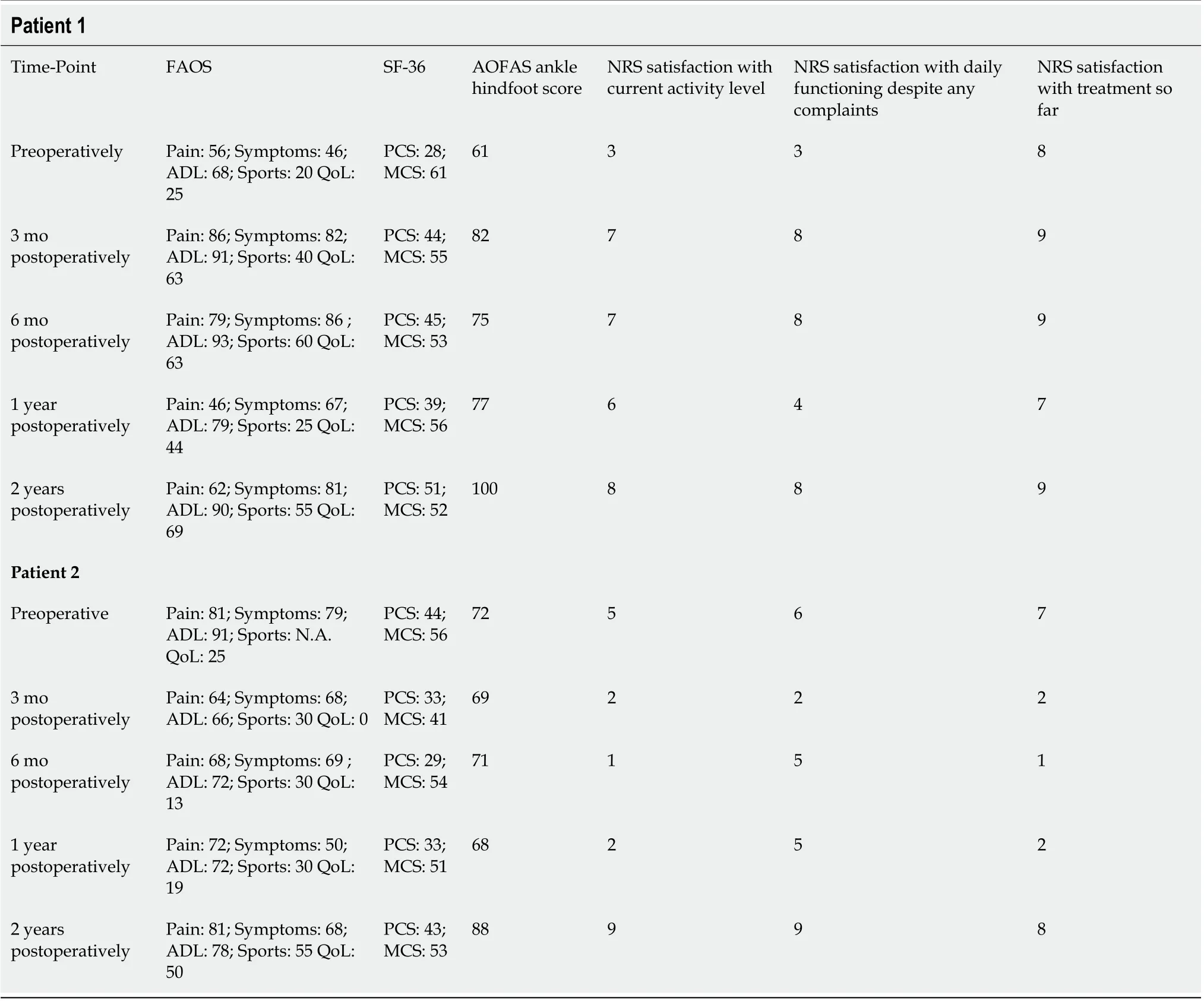
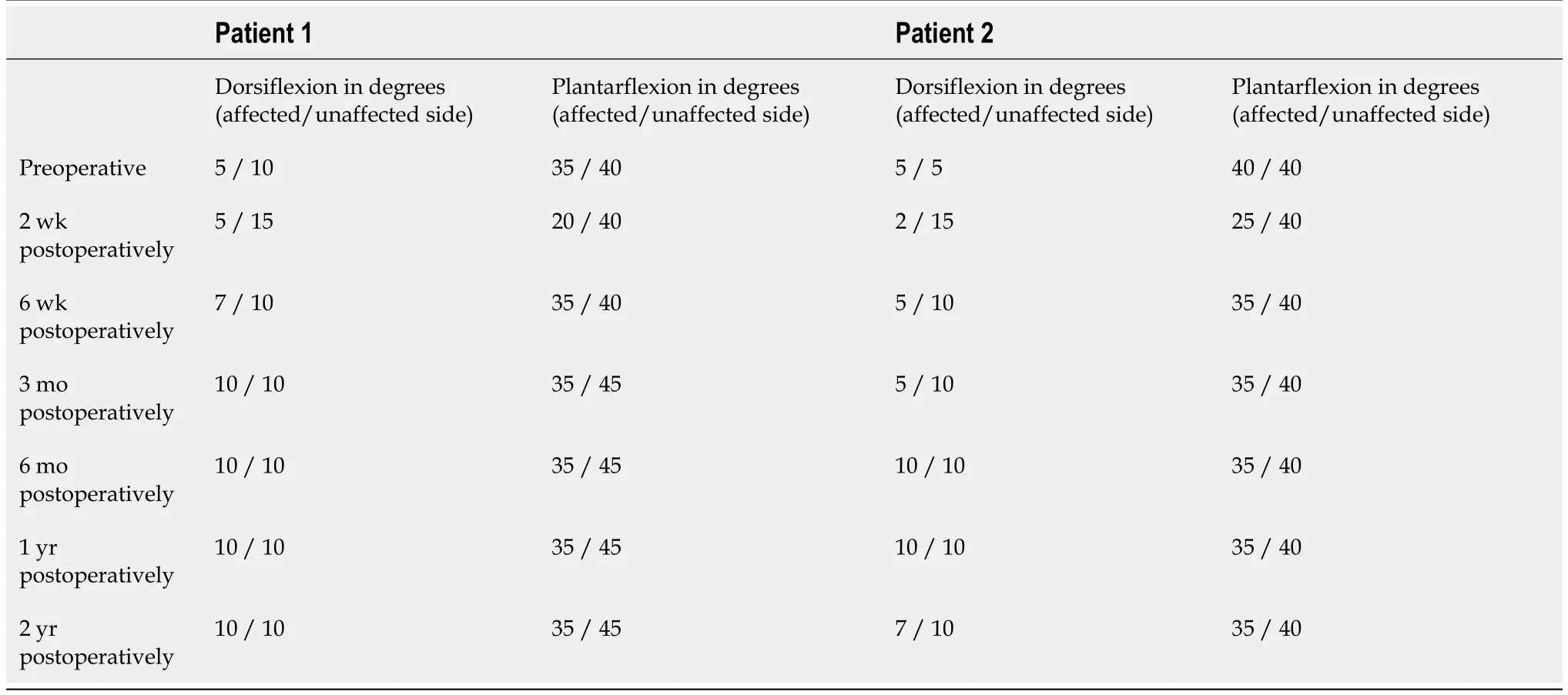
The other PROMs can be appreciated in Table 3.There were no complications and no reoperations.Radiologically,for all postoperative radiographs and CT-scans it was concluded that there were no indications of loosening of the implant,no implant migration,and no subsidence was noted(Figure 8).The ROM assessments were described in Table 4.
RESULTS
Primary outcome
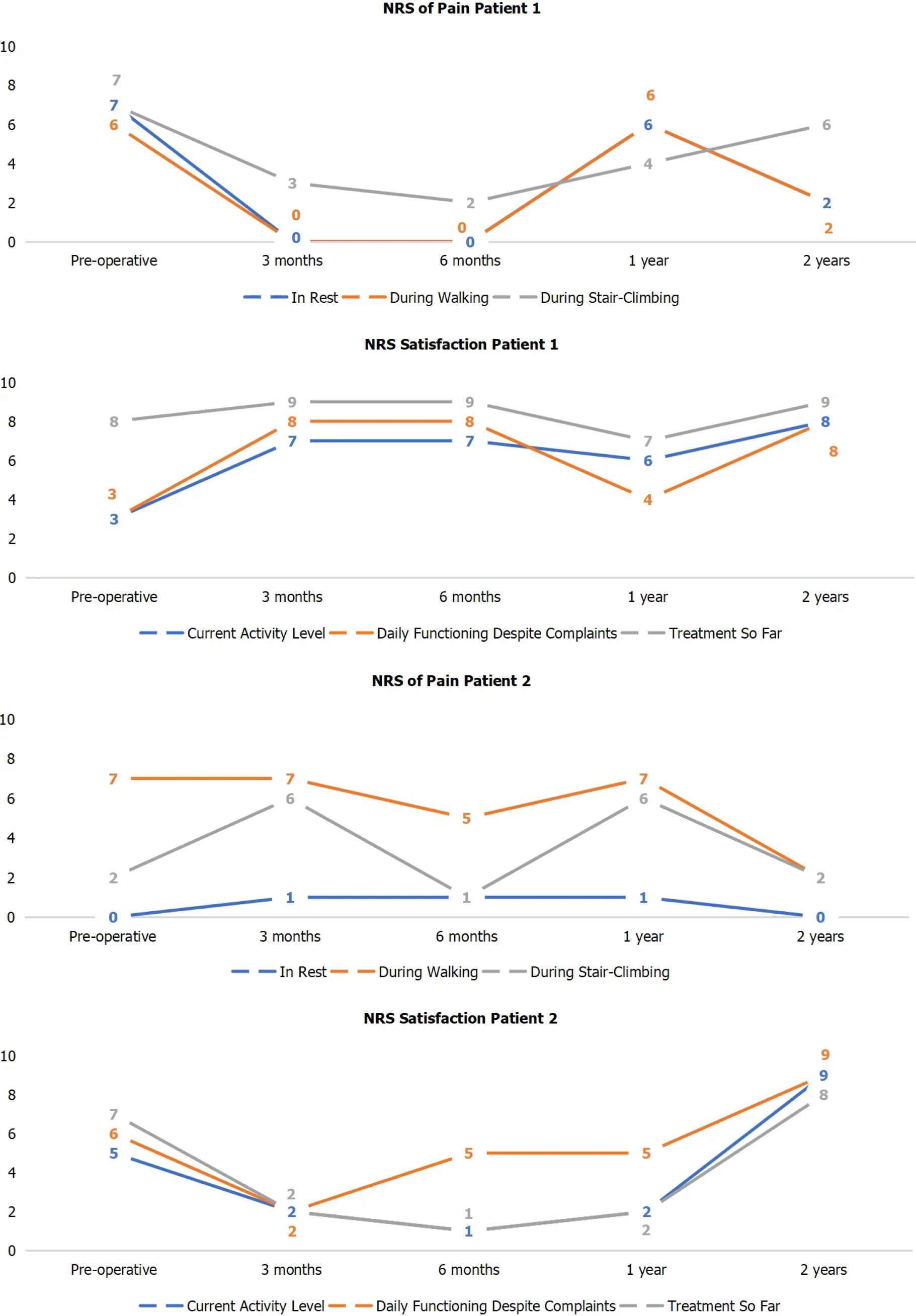
The primary outcome measure,the NRS of pain during walking improved from 6 preoperatively to 2 points at 2 years follow-up in patient 1,and from 7 preoperatively to 2 points postoperatively at 2 years follow-up in patient 2.This entails an improvement of 4 points and 5 points in patient 1 and 2,respectively(Figure 7).
Secondary outcomes
All statistical analyses were performed by means of SPSS version 20.0(SPSS Inc.,Chicago,IL,United States).Data will be presented as descriptive analyses through qualitative comparisons in the different patients.Consequently,data will be presented per patient,aiming at presenting changes in scores preoperativelypostoperatively.
As I read this message, a wave of sadness ran through me and I realized that she must have thought she was writing to her father the whole time. She and I would never have openly exchanged such words of affection. Feeling guilty for not clarifying, yet not wanting to embarrass her, I simply responded, Love you too! Have a good sleep!
DlSCUSSlON
This is the first study describing the results of the newly developed Ankle Spacer.The Ankle Spacer is a one-piece implant system that replaces the talar side of the tibiotalar joint,and can therefore be considered a hemi-arthroplasty procedure.The implant had been designed in order to overcome a number of downsides that are associated with the current treatment options for large,cystic,or multiple osteochondral lesions of the talus that have failed prior operative intervention(s).One of these treatment option being applied in the younger patient population is an arthroscopic ankle arthrodesis which results in highly satisfactory clinical outcomes mostly concerning pain outcomes[10-12].The downside of this operative intervention is that it results in functional limitations due to loss of ROM of the ankle[13].Furthermore,an ankle arthrodesis increases the long-term risk of(radiographic)osteoarthritis in adjacent hindfoot joints,particularly in the subtalar joint[14,21].An alternative option is the placement of a total ankle prosthesis,for which a substantial amount of bone needs to be resected[15,22].In order to tackle the downsides of these treatment options,develop a bone-sparing procedure and resurfacingthe talar dome to preserve ROM and potentially optimize physical functioning,the Ankle Spacer,a novel bone-sparing hemi-prosthesis,has been developed.The outcomes of treatment with the Ankle Spacer were described in the present article.Potential advantages include preservation of ankle motion,decreased stress on the midfoot and subtalar joints,and the possibility to perform an ankle fusion after failed hemi-arthroplasty.
I look at it like this, said the old man. Please a customer with one article, and he will come back when he needs another. Even if it is more costly9. He will save up for it, if necessary.
It is therefore clear that the Ankle Spacer is a new and innovative device.The current study is the first clinical trial performed investigating the efficacy of the Ankle Spacer,and therefore there is no clinical literature on this particular prosthetic device at this time to compare our clinical results to.Our current clinical results must therefore be compared to similar devices having been researched over the past decade.An articular and subchondral bone resurfacing implant procedure on one side of the joint(hemi-arthroplasty)can be considered a relatively novel operative intervention.Promising clinical results have been reported for similar treatment in the femoral and humeral head,as well as the first metatarsal and patellar surface.[16,23-27].Van Bergen[17,18,28]showed that a focal resurfacing implant is a promising treatment for talar OLTs that have failed prior operative treatment[28].They concluded that in a patient series including 38 patients the clinical results at a mean follow-up of three years were satisfactory.A different study by Holton[29]demonstrated that the use of a different resurfacing implant in the form of an articular resurfacing component maintained a good clinical improvement for patients at mid-term follow-up.A study by Brunner[30]which is less clinically comparable as it replaces the whole entity of the ankle,as opposed to the resurfacing of the talar surface as done by the Ankle Spacer or as opposed to the resurfacing implant as used by van Bergen[4,6,31],showed that short-term to mid-term results for patients treated with the Scandinavian Total Ankle Replacement(STAR)prosthesis have been encouraging.The long-term results were clinically inferior compared to the short-term and mid-term results.Additionally,studies on the Total Ankle Replacement(TAR),which is,to a certain though limited extent,comparable to the Ankle Spacer,have shown that long-term results demonstrated improved pain scores as it was observed to be a viable and durable operative implantation option[32,33].Another implantation technique in the form of a Tornier Salto Talaris Anatomic Ankle has been described in the literature.Mid-term results showed that the survivorship of this implant was calculated to be around 95%[34,35].A study by Queen[36]found that at a follow-up of 2 years investigating 51 patients after a fixed-bearing Total Ankle Replacement significant improvements in gait mechanics,pain reduction and functioning were observed.
As an objective conclusive remark on the evidence found on similar operative techniques,one can state that similar operative techniques yielded favorable clinical,radiological and safety outcomes.When comparing these three aspects to our results it can be concluded that in our treated patients,similar outcomes were found.Postoperative improvement was especially clear in the observed primary outcome measure which was the NRS pain during walking.This outcome measures typically describes the state and magnitude of pain in patients with OLTs of the talus as these patients experience pain especially when performing weight bearing activities,but often are unable to participate in sports due to complaints[4].It was shown that this primary outcome measure improved from 6 and 7 preoperativelyto 2 and 2 postoperatively at 2 years,in patient 1 and 2,respectively.As a result,we can conclude that for both patients a minimal clinically important difference was reached when comparing the preoperative state of pain to the postoperative state of pain at 2 years after the surgery.As an improvement of at least-1.0 on the NRS scale of 0 to 10 points is significantly associated with the concept of a “better improvement”,and an improvement of-2.0 on this scale is associated with a “much better improvement”[31].The improvement was also reflected in the radiological outcomes and the subjective satisfaction scores that were taken both preoperatively and postoperatively at the different follow-up moments in which it was clear that the patients stated that they were satisfied with their level of activity.Moreover,this was also reflected in the postoperative AOFAS Hindfoot Scale,which ranged from 88 to 100,scores that can be considered to represent a successful surgery.
Their sharp eyes soon discovered the form of a man crouching18 behind the bundles of sticks, and at first they felt a little frightened, and started as if they would run away
Furthermore,it was observed that there were no complications,no reoperations nor revisions,which implicates that,when extrapolating these results for a larger population based on our experience,the insertion of the Ankle Spacer can be regarded a safe procedure.This outcome should be interpreted in the light of the high re-intervention rates that are associated with Total Talar Prostheses,as some studies report that up to 38% of the patients need revision surgery within the first year after total ankle arthroplasty[37].With regards to ROM,it was shown that the ROM did not decrease in the patients,potentially due to the fact that patients received adequate postoperative physiotherapy and because of the fact that the Ankle Spacer was inserted just below the level of the subchondral bone plater not affecting joint congruency.This is clinically relevant to take into account when comparing ROM outcomes after placement of the Ankle Spacer to outcomes after an ankle arthrodesis procedure[38].
This study should be interpreted in light of its strengths and weaknesses.Strengths of this study include its prospective and thorough methodology,completeness of follow-up,and the use of various validated outcome measures in the assessment of a not yet studied resurfacing implant.Limitationsinclude the absence of a controlled group,lack of long-term follow-up outcomes ranging past the two years follow-up,and the small series of patients.However,we have found in our tertiary referral clinic that operates in an academic setting with the status of an official(inter)national expertise center for the treatment of OLTs in the ankle that the indication for an Ankle Spacer implantation is highly rare,even though we receive a high number of patients on a yearly basis.As a result,it was therefore noted that the Ankle Spacer has been removed from the market due to limited indications and strict regulatory
requirements.
The clinical relevance of the present study can be interpreted in the light of the highly specific indication for the implantation of the Ankle Spacer.This device is particularly suited for patients with multiple OLTs of the talar dome having failed prior operative intervention(s)with an unaffected distal tibial part of the ankle joint.This study shows that the Ankle Spacer is effective for this particular and rare patient group,thereby functioning as a joint-sparing alternative to more invasive operative interventions,such as an ankle arthrodesis or total ankle arthroplasty.
CONCLUSlON
On closer inspection3, though, the layer of dirt on Ronny’s face, the crusty nose, and the packed grime under his fingernails told me he didn’t get dirty at school. He arrived that way.
ARTlCLE HlGHLlGHTS
Research background
Osteochondral lesions of the Talus(OLT)are pathologic lesions of the talar cartilage and the subchondral bone.These lesions can occur in up to 50% of acute ankle fractures and sprains.For OLTs of larger size(..,above 10 or 15 mm in diameter)and of non-fragmentous morphology,the ‘standard’operative treatment options such as autologous chondrocyte implantation,osteochondral autograft transfer systems,and a Talar OsteoPeriostic grafting from the Iliac Crest procedure may result in satisfactory clinical outcomes.However,in some patients,there are multiple secondary lesions present of large and cystic nature.For these lesions,it is not always possible to harvest an osteo(chondral)autograft that is large enough to replace all the diseased osteochondral tissue of the talus without damaging the donor site or compromising the congruency of the ankle joint.Allograft treatment could be considered for the treatment of these type of lesions.However,these contain the disadvantages of loss of viability and stability in one-third of the grafts,and possibly clinically fail due to immunological reactions.However,when there are multiple secondary(..,failed prior surgery)lesions present on the talar articular surface in combination with a large and cystic nature,the above-described operative interventions are to be expected to result in relatively inferior outcomes.
Research motivation
Currently,it is difficult to treat patients with osteochondral lesions of the ankle that are of multiple,cystic and secondary nature.This is because the lesions are considered relatively large and difficult to treat.For this indication,it was usually performed to fuse the ankle joint.However,in the past 2 to 5 years,novel innovative surgical options have been developed,such as the Ankle Spacer,in order to overcome an ankle fusion or ankle prosthesis.
Research objectives
To describe the operative technique and the clinical efficacy of the Ankle Spacer for the treatment of multiple,cystic OLTs in patients with failed prior operative treatment.
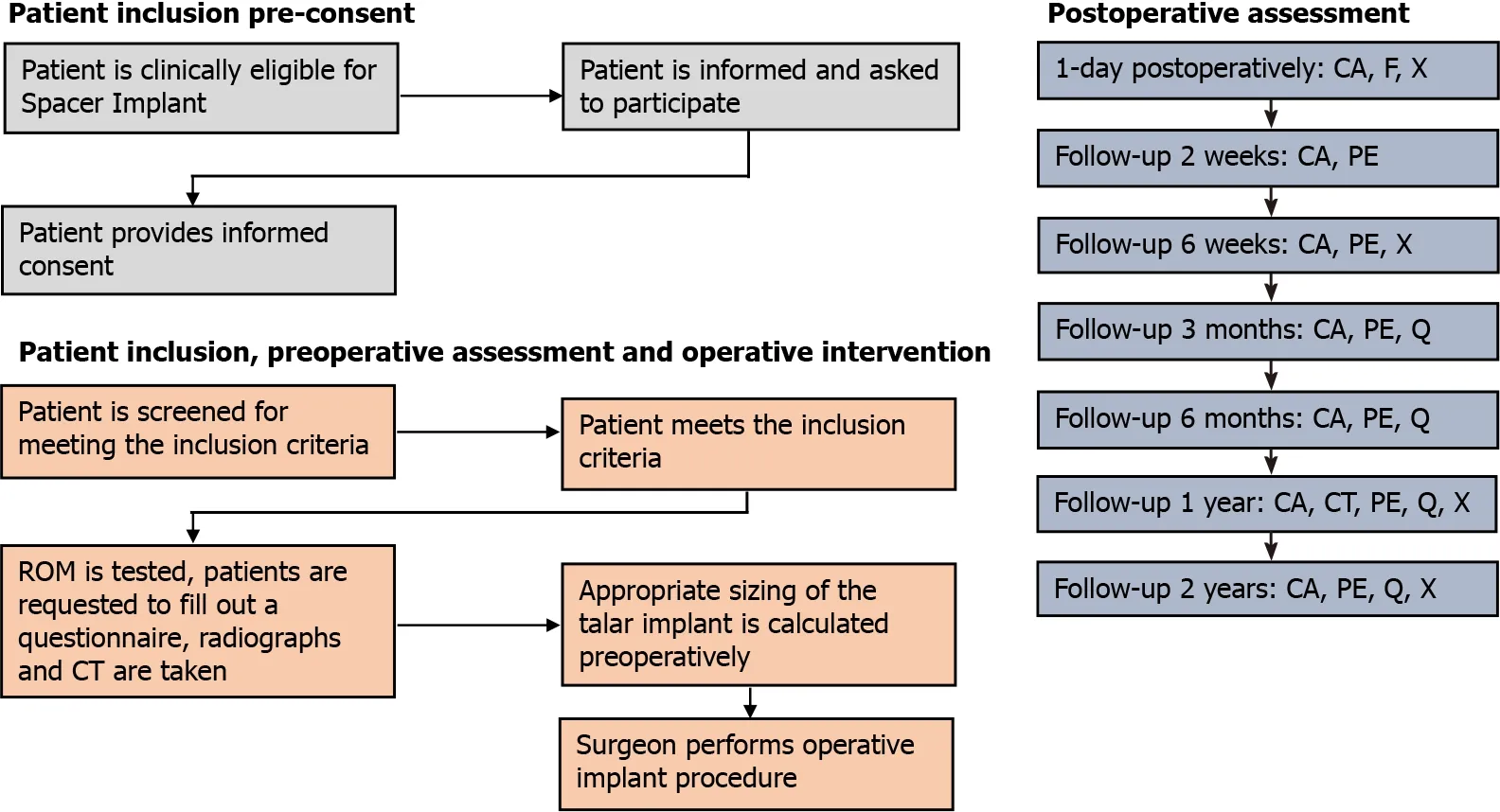
Preoperatively,standing weight bearing conventional radiographs and a computed tomography scan(CT)were taken.Preoperative patient-reported outcome measures(PROMs)consisted of the Numeric Rating Scale(NRS)of pain(during walking,in rest and during stairclimbing),patient satisfaction regarding complaints,activity and treatment,the American Orthopaedic Foot and Ankle Society(AOFAS)Hindfoot Score,Foot and Ankle Outcome Score(FAOS)and the Short-Form 36(SF-36 physical and mental component scale).The AOFAS score physician subscale and ROM were assessed by an independent researcher who was not involved in the operative procedure[19,20].Follow-up assessment was performed at two and six weeks,three and six months,one-year and two years postoperatively.At these follow-up moments the patients were requested to fill out a questionnaire consisting of the abovementioned PROMs and a physical examination was performed to test the ROM(expect for the postoperative visits at 2 wk and 6 wk after the surgery).Radiographs were taken one day,6 wk,one year and two years postoperatively.At one-year of follow-up,a CT-scan was made(Figure 1 describes the flow-chart outlining the study procedures).In addition,postoperative complications were recorded.Demographic data were also collected.The primary outcome measure in question was the NRS of pain during walking at 2-years follow-up and implant survival.All other outcome measures described above were secondary outcomes.
Research methods
In a prospective study including patients with multiple,cystic or large osteochondral lesions of the talus were included who failed previous surgical treatment.We looked at the numeric rating scale(NRS)for pain during walking at 2 years after implantation of the Ankle Spacer and we also assessed the NRS in rest and during stair-climbing,the American Orthopaedic Foot and Ankle Outcome Score,the Foot and Ankle Outcome Score,the Short-Form 36 and the range of motion of the ankles both pre-operatively as well as post-operatively.Radiographic evaluations were conducted to evaluate prosthetic loosening and subsidence.Revision rates and complications were also assessed.
Research results
In this prospective study,two patients underwent the implantation of an Ankle Spacer for osteochondral damage on the talar dome.We found that there were clinically relevant pain reductions during walking as well as important improvements in clinical outcomes as assessed with the patientreported outcome measures.Furthermore,it was found that there were no complications nor reoperations.
Research conclusions
The Ankle Spacer showed good clinical outcomes and clinically relevant pain reduction during walking,improvement in clinical outcomes as assessed with PROMs,and no complications or re-operations.This treatment option may therefore evolve as a joint-sparing alternative to an ankle arthrodesis,a total talar implant or a total ankle arthroplasty/resurfacing.
Research perspectives
Future research should be focused at the development of a prospective,self-learning algorithm taking into account the individual patient factors influencing outcomes after conservative and surgical treatment so that we can assess which patients would benefit most from which treatment options.
FOOTNOTES
Dahmen J,Altink JN,Vuurberg G,Wijdicks C,Stufkens S and Kerkhoffs G have made substantial contributions to conception and design,acquisition of data,analysis and interpretation of data,and have been involved in drafting the manuscript;Dahmen J and Altink JN have been involved in the acquisition of data;all authors have been involved in revising the manuscript,critically for important intellectual content,and have given final approval of the version to be published.
One day she escaped from the princess s notice and went to the prince, and laid her head on his feet and said: Heaven has bestowed62 on you beauty and charm
The study was approved by the local Medical Ethics Committee(Internal Review Board,IRB)of the Amsterdam University Medical Centre with reference number MEC 2017_175 and was performed in accordance with the principles of the Declaration of Helsinki and the medical Research Involving Human Subjects Act(WMO).
All patients provided informed consent prior to the participation in the study.
The study was sponsored by Arthrex as a post market study with reference number EMEA-17037.
No additional data available.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
Netherlands
But no one appeared, and even after another long sleep, from which he awoke completely refreshed, there was no sign of anybody, though a fresh meal of dainty cakes and fruit was prepared upon the little table at his elbow
Jari Dahmen 0000-0002-6849-1008;J Nienke Altink 0000-0001-9823-4611;Gwendolyn Vuurberg 0000-0001-5008-890X;Coen A Wijdicks 0000-0003-1831-6161;Sjoerd AS Stufkens 0000-0001-8791-3387;Gino MMJ Kerkhoffs 0000-0001-7910-7123.
Wang LL
A
Yuan YY
杂志排行

World Journal of Orthopedics的其它文章
- Assessing the academic achievement of United States orthopaedic departments
- COVlD-19 pandemic:An update on the reaction attitude of the spine societies and their members worldwide
- Liverpool carpal tunnel scoring system to predict nerve conduction study results:A prospective correlation study
- Bone mineral density in fracture neck of femur patients:What's the significance?
- Periprosthetic joint infections in femoral neck fracture patients treated with hemiarthroplasty-should we use antibiotic-loaded bone cement?
- Femoroacetabular offset restoration in total hip arthroplasty;Digital templating a short stem vs a conventional stem