Liverpool carpal tunnel scoring system to predict nerve conduction study results:A prospective correlation study
2022-03-05YuenChanVeeneshSelvaratnamTharjanManickavasagarVishwanathShettyVishalSahni
lNTRODUCTlON
Carpal tunnel syndrome(CTS)is one of the most common peripheral nerve compressive neuropathies.The prevalence of CTS in the United Kingdom is 7%-16%.A General Practice Research Database found that 88 men and 193 women present as new cases per 100000 population per year[1].The clinical symptoms and physical examinations are widely recognised,however there is still debate around what is the best approach for the assessment of carpal tunnel syndrome.Clinical assessment is considered the gold standard;however,controversies exist regarding the need for investigations such as nerve conduction studies(NCS)to aid with management decisions[2].
NCS is the investigation of choice when clinical diagnosis is inconclusive.It is also used to confirm the diagnosis of CTS.NCS have been found to be highly sensitive and specific for the diagnosis of CTS[3].However,NCS can be painful and expensive.The reported false negative rate of NCS is between 1.5% to 16%[4,5].The reported false positive rate is up to 46%[6].The evaluation of NCS for CTS involves the measurement of conduction velocity across the carpal tunnel,as well as determination of the amplitude of sensory and motor responses.Focal demyelination can occur with increased median nerve compression.This results in local conduction block and slowing of motor and sensory conduction across the wrist.The axons of the median nerve can be damaged with even greater compression resulting in reduced amplitudes.
Yes, the boy said harshly, a single blanket s enough for an old man when he s sent away. We ll save the other half, Dad. It ll come in handy later.
The grading of severity of CTS is as follows:Mild-prolonged sensory nerve action potential(SNAP),and/or slightly reduced SNAP amplitude.Moderate-abnormal median SNAP as above,plus prolonged median motor distal latency.Severe-prolonged median motor and sensory distal latencies,plus either an absent SNAP or low amplitude or absent thenar compound muscle action potential.Needle examination often reveal fibrillation,reduced recruitment,and motor unit potential charges[7,8].
There are validated measures such as the Boston Carpal Tunnel Syndrome Questionnaire which quantify symptoms and disability;however,this does not include clinical examinations.One study found that the clinical-neurophysiologic relationships are very strong when they evaluated the clinical picture with the disability scale of the Boston Carpal Tunnel Syndrome Questionnaire as well as clinical examinations findings.Conversely,the clinical-neurophysiologic relationship is not so clear and simple when they compared it with the symptoms only[9].Other scoring systems include use of hand diagrams such as the Katz[10]hand diagram(looking at distribution of symptoms in the hand)and the CTS-6 scale(looking at symptoms and examination)[11].A systematic review found there are limited evidence to support the use of these scoring systems[12].
Numerous patients with CTS have severe symptoms but no NCS changes,therefore we hypothesised that a scoring system combining symptoms,signs and risk factors can help with the diagnosis of CTS.The aim of the study was to correlate the severity of NCS results to a scoring system which included symptoms,signs and risk factors.
MATERlALS AND METHODS
We prospectively collected data for fifty-nine patients who were referred to our hand unit with symptoms of carpal tunnel syndrome.All patients who were referred and diagnosed with CTS clinically were included in the study.Patient with symptoms but diagnosed with other diagnoses were excluded.All patients who clinically showed symptoms of CTS had the ten-point scoring system and NCS carried out.We prospectively collected data for 61 hands(59 patients)over a ten-month period.
Now one day it seemed to her that the sky opened above her, and a great shower of shining gold fell through the window in the roof, and lay glittering in her room
We reviewed existing scoring systems and examination signs to develop a scoring system.We developed a 10-point scoring system which included symptoms,signs and risk factors.We scored our patients using the ten-point scoring system.The scoring system included;four symptoms(2 Katz[10]hand diagram-for tingling and numbness,nocturnal paresthesia and bilateral symptoms),four clinical signs(weak thumb abduction test,Tinel’s sign,Phalen sign and hypoalgesia in median nerve territory)and two risk factors(age more than 40 years and female sex).We classified the NCS to normal,mild,moderate and severe as described above[8].
At this point, the little boy came out running towards his mother with tears in his eyes. He hugged her and felt an overwhelming5 sense of the sacrifice that his mother had made for him. He held her hand tightly6 for the rest of the day.
This study was approved by Southport and Ormskirk NHS Hospital.
The ten-point scoring system included tingling and numbness on a Katz hand diagram.Nocturnal paresthesia is defined as night numbness and tingling or wakening.Bilateral symptoms imply symptoms involving both hands.Signs included weak thumb abduction;Tinel’s sign which is reproduction of the symptoms on tapping over the carpal tunnel;Phalen’s sign which is reproduction of the symptoms for CTS on flexion of the wrist for 60 s.Hypoalgesia is defined as reduced sensitivity to a painful stimulus in the median nerve distribution.
Other data collected were age,sex,laterality of hand affected,NCS results and duration of symptoms.It was our common practice in our hospital to refer a patient for a NCS in suspected cases of CTS prior to surgical intervention.All patients in this study were from a single upper limb surgeon’s practice.Statistical analysis was done using SPSS.Eta value was used to determine the association between NCS category and CTS score.Eta of 0 is no association and Eta of 1 is perfect association.One way ANOVA test was used to test difference between the groups.The partial Eta squared was used to test how much variability of the scores was accounted for by the NCS severity.Post hoc analysis was carried out to determine which NCS groups have differences between each other.The post hoc analysis used in this study was Scheffe.
RESULTS
No conflict of interest.
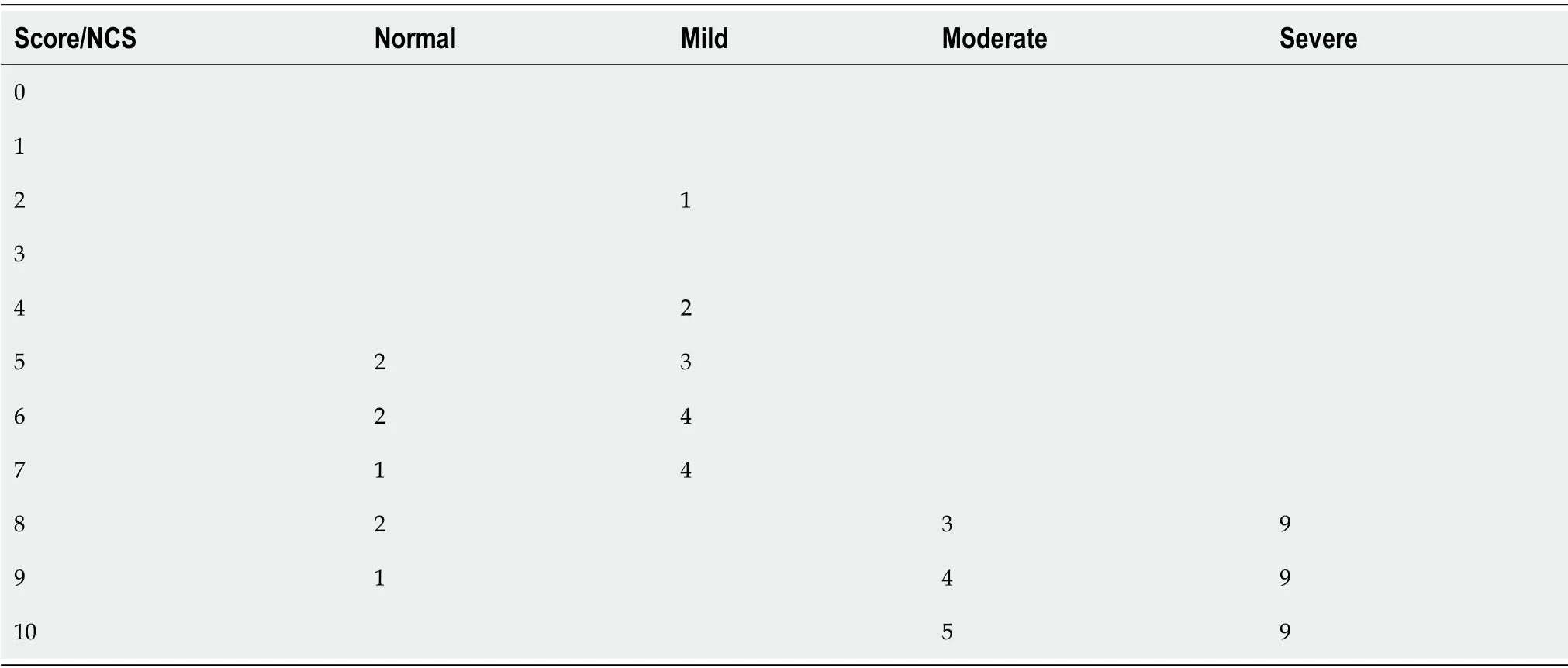
The mean score for the categories were as follows:6.75 for normal NCS,5.50 for mild NCS,9.17 for moderate NCS and 9 for severe NCS.All scores of 8 or more matched with NCS of moderate and severe intensity apart from three scores which were greater than seven that were normal on NCS(Table 2).
A post hoc analysis showed there were statistical significance between the CTS scores of patients with normal NCS and patients with moderate and severe NCS(< 0.001).There was statistical significance between the CTS scores of patients with mild NCS compared with CTS scores of patients with moderate and severe NCS(< 0.001).There was no significant statistical difference between CTS scores of patients with moderate NCS findings compared with severe NCS findings(< 0.979).

One of the three patients who had a score over 7 but had normal NCS was found to have a cervical disc herniation after a magnetic resonance imaging of the cervical spine.This patient underwent cervical disc decompression and had resolution of her symptoms.She did not require a carpal tunnel decompression.The other two patients with a score of 8 and 9 respectively underwent a carpal tunnel decompression despite normal NCS as clinically they were both symptomatic.Both patients reported resolution of symptoms post carpal tunnel decompression.
An Eta coefficient test was performed to determine the strength of correlation between the scores and the NCS categories of normal,mild,moderate and severe.An Eta score was 0.822 for the CTS score being the dependent value and the NCS category being the independent variable shows a strong association between the score and the NCS categories.A one-way ANOVA test showed there were a significant statistical difference between the severity groups(< 0.001).The partial Eta squared was 0.676 meaning that 67.6% of the variability of the CTS score is accounted for by the severity of their CTS.
The snow fell. For the next few hours, they read and talked. Sometimes she caught his hand and put it on her belly to feel the baby move. From time to time he got up to feed the fire, glancing out the window to see three inches on the ground, then five or six. The streets were softened50 and quiet, and there were few cars.
DlSCUSSlON
An appropriate diagnosis of carpal tunnel syndrome is important as it is a common condition.There is no consensus on whether to base treatment decisions on clinical history and assessment only,or NCS should be done in every case.Within the UK,different areas have different rules on diagnosis and treatment.The British Orthopaedic Association guidelines states NCS is not routinely needed and should only be used if clinical examination and history are equivocal,if there is persistent or recurrent carpal tunnel syndrome or if there is an unclear diagnosis suggesting peripheral neuropathy[13].
NCS may not always be positive in patients who are symptomatic.Not every clinician request NCS because of the costs and delays associated with NCS[14].One study looking at just history and examination findings concluded that the majority of patients who have CTS on the basis of their scoring system,further NCS studies did not change the probability of diagnosing the condition[11].Another study looked at using a web-based CTS questionnaire prior to the patient’s appointment and found that it provided a sufficiently accurate prediction of the likelihood of CTS to help in the initial planning,investigation and treatment of CTS[15].
From the very beginning, the girl s family objected strongly to her dating this guy, saying that it had got to do with family background and that the girl would have to suffer for the rest of her life if she were to be with him.
A CTS scoring can help in planning and streamlining of services which is of significant importance especially in light of the current pandemic.We should aim to get the right diagnosis as effectively and as efficiently as possible and to use resources such as NCS in a cost-effective way.
The reported sensitivity and specificity for each of our sign and symptoms are as follows;classic or probable Katz hand diagram pattern(0.64,0.73 respectively),nocturnal paraesthesia(0.51,0.68 respectively),bilateral symptoms(0.61,0.58 respectively),weak thumb abduction test(0.66,0.66 respectively),Tinel sign(0.60,0.80 respectively),Phalen sign(0.91,0.86 respectively),hypoalgesia in median nerve(0.51,0.93 respectively),age more than 40 years(0.80,0.41 respectively)[10,16-21].Female sex has an increased risk of developing CTS[22].This may be due to females being over-represented in jobs that have a high risk of developing CTS.When the occupational exposure is truly similar,the risk of developing CTS is similar between both genders.In our cohort,71% of patients were females.We did not obtain job specifications for our patients.
We scored patients’ signs and symptoms using our CTS scoring system.This was then correlated with the findings of the NCS.The scoring system included-four symptoms and four clinical signs and two risk factors.We classified the NCS results to normal,mild,moderate and severe.
In 1965, Chip was drafted, Robbie went on. The next year, he went to Vietnam. He never came back. Twenty years later, Aunt Katie still talks about Chip. This flower is from her to him. She asked me to leave it here.
We did not find a difference between patients with moderate and severe NCS findings or between patients with normal and mild NCS findings.However,clinically we feel both the moderate and severe group would be treated with a carpal tunnel decompression,therefore it is more important to differentiate between patients with normal and mild vs.moderate and severe NCS.In patients with normal and mild NCS,treatment will also depend on their symptoms.If symptoms are severe then they will more likely receive surgical intervention otherwise they would initially undergo a period of conservative management.Surgical intervention would only be undertaken should the patient fail their trial of conservative management.
The strength of our study is having a scoring system that combines signs,symptoms and risk factors.There are limitations to our study.It was a relatively small number of patients and we would need further studies to validate our scoring system.We did not have the co-morbidities or occupation of the patients and we did not re-do the scores after surgical decompression to see if the score can be used to monitor outcome post CTD.Further studies looking to include these factors would be beneficial.
CONCLUSlON
There is still debate around what is the best approach for assessment of Carpal tunnel syndrome(CTS).Controversies do exist regarding the need for investigations such as the need for nerve conduction studies(NCS)to aid with management decisions.
She and her husband had lived in Vienna, Austria, and had opposed the Nazis14 before the Second World War. They decided15 to flee to Switzerland, but her husband said they must go separately. She left first. Later she heard that he had died in a concentration camp.
ARTlCLE HlGHLlGHTS
Research background
We feel that this simple scoring system can be used to predict and correlate the severity of NCS in patients with CTS.Based on our study,we believe that patients who score less than eight may require NCS to confirm the diagnosis of CTS.However,patient who score more than 7 have a 93% chance of having moderate to severe CTS on NCS.Use of our simple scoring methods can help determine patients with moderate and severe CTS.In this group of patients,we recommend not using NCS.Patients scoring less than 8 may have mild or moderate CTS and,in this group of patients,we recommend the use of NCS.Further studies,looking to validate the scoring system clinically would be useful.
Research motivation
We hypothesised that a scoring system combining symptoms,signs and risk factors can help with the diagnosis of carpal tunnel syndrome and whether nerve conduction studies would be required.
Research objectives
The aim of the study was to correlate the severity of nerve conduction study results to a scoring system which included symptoms,signs and risk factors.
Research methods
This study shows our simple ten-point scoring system have a high correlation with the NCS results.Our CTS score differentiated between patients with normal/mild NCS symptoms to patients with moderate/severe NCS findings.The difference is significant between patients with normal/mild NCS findings compared with patients with moderate/severe NCS findings.We have CTS in patients across the range of the CTS scores but the aim of the scoring system is to identify patients who would most likely benefit from NCS prior to carpal tunnel decompression as their clinical findings are equivocal.
Research results
All scores of 8 or more matched with NCS results of moderate and severe intensity apart from three scores which were greater than seven that had normal NCS.Eta score was 0.822 for the CTS score being the dependent value and the NCS category being the independent variable showing a strong association between the scoring system and the NCS group.
Research conclusions
Based on our study,we believe that patients who score less than 8 may require NCS to confirm the diagnosis of CTS.However,patients who score more than 7 have a 93% chance of having moderate to severe CTS on NCS.The use of our simple scoring methods can help determine patients with moderate and severe CTS.In this group of patients,we recommend not using NCS.Patients scoring less than 8 may have mild or moderate CTS and in this group of patients,we recommend the use of NCS.
Research perspectives
The use of our Liverpool carpal tunnel scoring system can have the potential to be used to help determine if NCS is required.Further studies looking into the validation of the scoring system is required.
FOOTNOTES
Chan Y and Selvaratnam V wrote and edited the manuscript and were involved in the analysis of the study;Selvaratnam V,Manickavasagar T,Shetty V,and Sahni V were involved in the collection of data and editing of the manuscript.
This study was conducted prospectively.Local clinical governance approval was obtained.All patients who underwent the ten-point scoring system and had NCS was included.Our ten-point scoring system(Table 1)was applied to patients with symptoms of CTS prior to NCS.The score of the ten-point scoring system was then correlated with the severity results of the NCS.The score was used to correlate with the NCS results but was not used to decide on treatment.As the scoring depended on the signs and symptoms no blinding could be applied to the assessors or the patients.The assessors of clinical signs and symptoms were not involved in the statistical analysis of the results.The data analysis was carried out by a member of authors who were blinded to the patients and tests.
A clinical trial registration was not required.
The informed consent statement is not applicable for this study.
There were 61 scores in 59 patients.There were 43 female and 18 male patients.The mean duration of symptoms was 17 mo(range 2-84 mo).Thirty-two were left hands and twenty-nine were right hands.There were 8 patients in the normal NCS category,14 patients in the mild NCS category,12 patients in the moderate NCS category and 27 patients in the severe NCS category.The mean age was 60 years(range 37-91 years).
No additional data are available.
The authors have read the CONSORT 2010 statement,and the manuscript was prepared and revised according to the CONSORT 2010 statement.
This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial(CC BYNC 4.0)license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See:https://creativecommons.org/Licenses/by-nc/4.0/
United Kingdom
52. Then Hansel sprang like a bird out of a cage when the door is opened: Here we have more bird imagery with this simile123 describing Hansel s release from the stable.
Yuen Chan 0000-0001-8673-7406;Veenesh Selvaratnam 0000-0002-3821-1781;Tharjan Manickavasagar 0000-0002-3725-1415;Vishal Sahni 0000-0003-1117-6530.
When, then, the fatal day came the unhappy Potentilla was led into the great hall between the King and Queen, the latter wild with envy at the murmurs89 of admiration90 which rose on all sides at the loveliness of the Princess
I have served thee in much, Tsarevitch Ivan, said the Gray Wolf, but I will also do thee this service. Listen. When we come near to the Palace, I myself will take the shape of the Tsar s daughter, and thou shalt lead me to Tsar Afron, and shalt take in exchange the Horse with the Golden Mane. Thou shalt mount him and ride far away. Then I will ask leave of Tsar Afron to walk on the open steppe, and when 1 am on the steppe with the Court ladies-in-waiting, thou hast only to think of me, the Gray Wolf, and I shall come once more to thee.
Wang JL
She listened to my reasons why not and simply said, I want to do it. I agreed. And in the next few days, Sonali s repertoire18 of mostly Disney tunes19 expanded to include a beautiful prayer from the Rig Veda that we heard at the Siddha Yoga Meditation20 Ashram in New York where we were staying. Clearly, Let Us Be United was the perfect song for Sonali to sing:
Peter promised faithfully he wouldn t, and the old woman continued: This evening at sunset go to yonder pear-tree which you see growing at the cross roads
A
Wang JL
杂志排行

World Journal of Orthopedics的其它文章
- Assessing the academic achievement of United States orthopaedic departments
- COVlD-19 pandemic:An update on the reaction attitude of the spine societies and their members worldwide
- Clinical efficacy of the Ankle Spacer for the treatment of multiple secondary osteochondral lesions of the talus
- Bone mineral density in fracture neck of femur patients:What's the significance?
- Periprosthetic joint infections in femoral neck fracture patients treated with hemiarthroplasty-should we use antibiotic-loaded bone cement?
- Femoroacetabular offset restoration in total hip arthroplasty;Digital templating a short stem vs a conventional stem