Rare primary mature teratoma of the liver: A case report
2022-01-05YuryKovalenkoYuryZharikovYanaKiselevaAntonGoncharovTatyanaShevchenkoBeslanGurmikovDmitryKalininAlexeyZhao
Yury A Kovalenko, Yury O Zharikov, Yana V Kiseleva, Anton B Goncharov, Tatyana V Shevchenko, Beslan N Gurmikov, Dmitry V Kalinin, Alexey V Zhao
Yury A Kovalenko, Anton B Goncharov, Tatyana V Shevchenko, Beslan N Gurmikov, Alexey V Zhao, Department of Surgical Oncology and Chemotherapy, A.V.Vishnevsky National Medical Research Center of Surgery of the Russian Ministry of Healthcare, Moscow 115093, Russia
Yury O Zharikov, Department of Human Anatomy, Sechenov First Moscow State Medical University (Sechenov University), Moscow 119048, Russia
Yana V Kiseleva, International School “Medicine of the Future”, Sechenov First Moscow State Medical University (Sechenov University), Moscow 119048, Russia
Dmitry V Kalinin, Pathology Department, A.V.Vishnevsky National Medical Research Center of Surgery of the Russian Ministry of Healthcare, Moscow 115093, Russia
Abstract BACKGROUND Primary liver teratoma is an extremely rare tumor usually affecting children under the age of 3 years.Specific signs of teratoma on ultrasound, computed tomography (CT) or magnetic resonance imaging are lacking, which makes morphology the only diagnostic tool.Misdiagnosis of a mature teratoma may lead to excessive liver resection, whereas misdiagnosis of an immature teratoma may result in spread, causing a life-threatening condition.Consequently, a careful tumor examination is important, and the rarest types of tumors must be accounted for.CASE SUMMARY We describe a 52 years old female who presented with a solid mass in the left liver lobe.Contrast-enhanced CT and magnetic resonance imaging (MRI) revealed a round, heterogeneous lesion containing a number of fluid areas and areas of calcification in the middle, and the provisional diagnosis was cholangiocarcinoma.The patient underwent resection of liver segment I.Immunohistochemistry analysis of the resected lesion indicated thyroid follicular epithelium; however, the thyroid gland was intact.10 years prior to presentation the patient underwent a surgery due to mature teratoma of the right ovary, nevertheless the tumor was benign and could not spread to the liver, in addition teratoma of the liver was also benign.This led to the final diagnosis of primary mature liver teratoma.CONCLUSION Primary hepatic teratoma, including heterotopia of the thyroid gland in the liver, is an extremely rare condition in adults that needs to be considered in the differential diagnosis of solid-cystic neoplasms in the liver and cholangiocarcinoma.This case adds to the limited literature on the patient presentation, clinical workup and management of liver teratomas.
Key Words: Case report; Primary liver teratoma; Ectopic thyroid gland tissue; Mature teratoma; Epidermoi cyst
INTRODUCTION
Teratoma is a rare germ cell tumor (GCT) that comprises at least two of three germ cell layers, the ectoderm, mesoderm and endoderm, and affects both children and adults.Teratomas primarily affect gonadal tissues, as the origin of these tumors is primordial germ cells, which migrate from the allantois to the fetal gonads during the first week of fetal life[1].Thus, teratomas may also occur along the migration path of primordial germ cells, which can remain in midline extragonadal sites[2].Consequently, the liver is an extremely rare site for primary teratomas, with an incidence of approximately 1% of all teratomas.Most patients with hepatic teratoma are children under the age of 3 years[3].Nevertheless, primary or secondary teratomas of the liver can lead to serious health issues and can be a life-threatening condition that claims a comprehensive diagnosis and well-timed therapy.Therefore, our case report and review aim to collect scarce information about hepatic teratomas.
Classification of teratomas
Depending on the differentiation degree of their components, teratomas are classified as mature and immature[1].Immature teratomas have a tendency for rapid growth, malignant transformation, and metastasis within adults; therefore, the prognosis is very poor[2].
Mature teratomas can be cystic, solid and mixed.According to the reported cases, cystic teratomas of the liver are the most common within mature teratomas.Mature cystic teratomas of the liver represent a mostly unilocular cystic cavity that may have septation and/or calcification and comprise mature elements derived from 3 cell layers, such as thyroid tissue, tooth enamel, hairs, skin, bone, fat, cartilage, neural tissue, or epithelium.The most commonly mature cystic teratomas affect the ovaries; however, approximately 1% of these lesions are found in the liver, usually within females in the right liver lobe[4-6].The shape and size of mature cystic teratomas on gross appearance are not unique and vary significantly; thus, the largest reported lesion dimensions were 21 cm× 18 cm× 12 cm, and the weight was 1837 g[7].The symptoms of mature cystic liver teratoma are nonspecific and conditioned by mechanical pressure of the growing tumor, including abdominal distension, constipation, fever, loss of appetite, abdominal pain, a sense of fullness in the right upper quadrant, vomiting,etc.[3,8].Cases of asymptomatic mature teratoma have also been reported[9,10].Rahmatet al[11] described a 46 years old male who presented with cholangitis caused by a primary benign teratoma of the liver measuring 5.0 cm x 6.5 cm x 8.0 cm and compressing a common bile duct.Despite their high degree of differentiation, cystic teratomas can transform to malignant tumors and harbor other neoplasms; therefore, complete surgical removal is an optimal treatment that can be followed by chemotherapy if necessary[5,12].Recently, Ramkumaret al[13] reported a case of a primary mature teratoma rupture accompanied by acute abdominal pain in a 65 years old female.Surgical removal of the tumor was performed after liquid and antibiotic therapy, and areas of necrosis and hemorrhage were found on histopathology[13].
The differentiation degree of the components of immature teratomas is low, and these tumors may involve any type of tissue, although neurogenic elements are the most common.On histopathology, these teratomas can also be divided into predominantly cystic, solid, and solid with multiple cysts and may contain areas of necrosis and hemorrhage.Immature teratomas tend to show rapid growth with liver capsule invasion and metastasis[2].Primary immature hepatic teratomas are extremely rare.To the best of our knowledge, only 3 case reports have been published in the English literature up to 2021.The liver is also a rare site of teratoma metastasis; however, secondary immature teratomas are more frequent[14,15].The symptoms of immature liver teratoma have been described in a few case reports and include pain and sensation of fullness in the right upper quadrant, fatigue, sweating, nausea, vomiting, and weight loss[2,16].Malek-Hosseiniet al[16] reported the largest immature liver teratoma, measuring 27 cm in diameter, and the patient recovered completely through surgery with a good follow-up.Immature liver teratomas lead to an elevation in AFP levels, whereas mature teratomas cannot produce AFP; thus, AFP is usually utilized for the differential diagnosis; nevertheless, AFP elevation does not necessarily occur[14,17].The treatment of immature teratomas includes adjuvant chemotherapy and complete resection of the primary tumor and every metastasis whenever possible[18].Nonresectable hepatic teratomas require liver transplantation[19].
Diagnosis of hepatic teratomas
The main diagnostic tools for liver teratoma detection are contrast-enhanced CT and MRI, which can show the size, shape, and structure of the tumor and its position related to adjacent elements and organs.CT scans can reveal areas of calcification in teratomas, whereas MRI scans are not sensitive to calcium[3].Choet al[20] revealed the high sensitivity of attenuation correction CT (AC-CT) acquired during18F-FDG PETCT in the diagnosis of immature ovarian teratomas, as their components show significant18F-FDG uptake.Thus,18F-FDG PET-CT may be a useful diagnostic tool[20].Serum AFP, LDH, hCG, CEA, and liver enzymes may be elevated in some patients[2].However, the final diagnosis of teratoma can be made based only on the histopathology of the tumor samples[9].
Growing teratoma syndrome
Teratomas are usually treated with surgery and chemotherapy.However, metastatic teratomas of nonseminomatous germ cell tumors (NSGCTs) may not respond to chemotherapy and become significantly enlarged even after the original tumor is removed and serum tumor markers (AFP, beta-HCG) and LDH return to normal.This condition is known asgrowing teratoma syndrome(GTS).This syndrome is uncommon, and its etiology and pathogenesis are still unclear; consequently, the diagnosis may be delayed, and the patient's prognosis may become poor[21].There are two dominant theories on the pathogenesis of GTS: (1) Chemotherapy leads to the survival and subsequent thriving of mature components, whereas immature components are highly sensible; and (2) Chemotherapy results in DNA damage and transformation of the immature teratoma to a mature teratoma[22].Hiesteret al[23] suggested a model of GTS development, according to which these tumors comprise meroclones derived from holoclones under chemotherapy.The authors termed these cells “teratomaforming transit-amplifying cells (TF-TACs)”[23].
GTS should be suspected in every patient with a growing tumor and normal tumor marker levels after chemotherapy of the original NSGCT[21].The most common sites of original NSGCTs are the ovaries and testis, whereas metastasis usually affects the retroperitoneum; nevertheless, cases of GTS from liver metastasis have also been reported.The common features of the described patients included young age (22 and 24 years old), multiple metastatic deposits among the entire liver, retroperitoneal lymph nodes and kidney from testicular tumors, and elevated AFP levels.Interestingly, the liver teratomas were mature, and there was no evidence of malignancy.Both patients underwent radical orchiectomy, nephrectomy, retroperitoneal lymphadenectomy and chemotherapy, and AFP levels returned to normal.However, the liver teratomas continued to grow, confirming the GTS diagnosis, and patients were accepted for liver transplantation (LT).After LT, there was no evidence of teratoma recurrence[24,25].O’Reillyet al[22] presented the first case of GTS in a primary liver teratoma in a 22 years old female.AFP levels were elevated (over 18000 cm before chemotherapy) and significantly decreased thereafter, whereas the tumor continued to enlarge up to 31.4 cm x 25.4 cm x 42.1 cm, and GTS was suspected.The patient was discharged after right hepatectomy and resection of the right mediastinal and diaphragmatic metastases, and there was no evidence of teratoma recurrence after 18 mo[22].Growing teratomas of the liver may cause a disturbance in vital function either by the mechanical compression of contiguous organs and vessels or by hepatic failure; moreover, the incidence of GTS-related malignancy is 2%-8%.As these tumors do not respond to chemo- or radiotherapy, such patients should undergo complete surgical removal of the teratomas, as incomplete resection has a higher rate of tumor recurrence[23].
CASE PRESENTATION
Chief complaints
A 52 years old woman was referred to our hospital by a specialist at the diagnostic center after a solid tumor was detected in the left lobe of the liver with ultrasound (US).
History of present illness
US revealed that the lesion measured 118 mm x 93 mm in size with sharp edges, a heterogeneous and hyperechoic parenchyma and areas of calcification.The patient did not have any complaints associated with this lesion.
History of past illness
The patient underwent right oophorectomy 10 years prior to presentation due to an epidermoid cyst (mature teratoma), and no chemo- or radiotherapy was assigned because the tumor was benign.Apart from that, the medical and family histories were unremarkable.
Personal and family history
Personal and family history is not burdened.
Physical examination
During the general examination, no abnormalities were detected.
Laboratory examinations
The laboratory assessment also did not reveal any pathological findings.The tumor markers CA 19-9 and AFP were not elevated (< 2.5 U/mL and 4.61 U/mL, respectively).
Imaging examinations
Subsequent US with color flow mapping (CFM) revealed moderate vascularization of the lesion and compression of the left portal vein, left hepatic artery and left hepatic vein.Subsequent CT and MRI revealed a heterogeneous lesion 111 mm x 109 mm x 97 mm in size with a round shape containing a number of fluid areas sized from 5 to 12 mm and areas of calcification in the middle of the tumor.The distal intrahepatic bile ducts were dilated, and the inferior vena cava was compressed (Figures 1 and 2).With reference to the CT and MRI scans, the provisional diagnosis was formulated as cholangiocarcinoma of the left hepatic lobe.
MULTIDISCIPLINARY EXPERT CONSULTATION
The histological examination suggested biliary hamartoma, but the lack of bilirubin in the cells lining the cavity did not allow us to exclude lymphangioma or follicular cancer (Figure 3).To reveal the true nature of the tumor and exclude a malignancy, immunohistochemical tests were performed.They demonstrated focal positive expression of thyroglobulin (clone 2H11+6 E1), TTF-1 (clone 8G7G3/1), and galectin-3 (clone 9C4), overexpression of cytokeratin 8 and 18 (clones B22.1 + B23.1) and negative expression of CD34 (clone QBEnd/10).The immunophenotype corresponded to the thyroid follicular epithelium.In the postoperative period, we performed ultrasonography, which did not show thyroid gland malignancy and the patient had no endocrine problems.
FINAL DIAGNOSIS
According to the gross appearing, histology and immunohistophenotype the ectopic thyroid gland in the liver (mature teratoma) was finally evident in the patient.
TREATMENT
The patient underwent resection of segment I with the surrounding tumor hepatic parenchyma, D1 Lymphadenectomy and cholecystectomy.The intraoperative inspection revealed an increase in the left liver lobe due to the well-defined encapsulated inhomogeneous tumor in the first segment of the liver (14 cm х 13 cm х 13 cm), crushing atrophied segments 2 and 3 (Figures 4 and 5).The consistency of the tumor was soft, and on its surface, there were twisted veins.
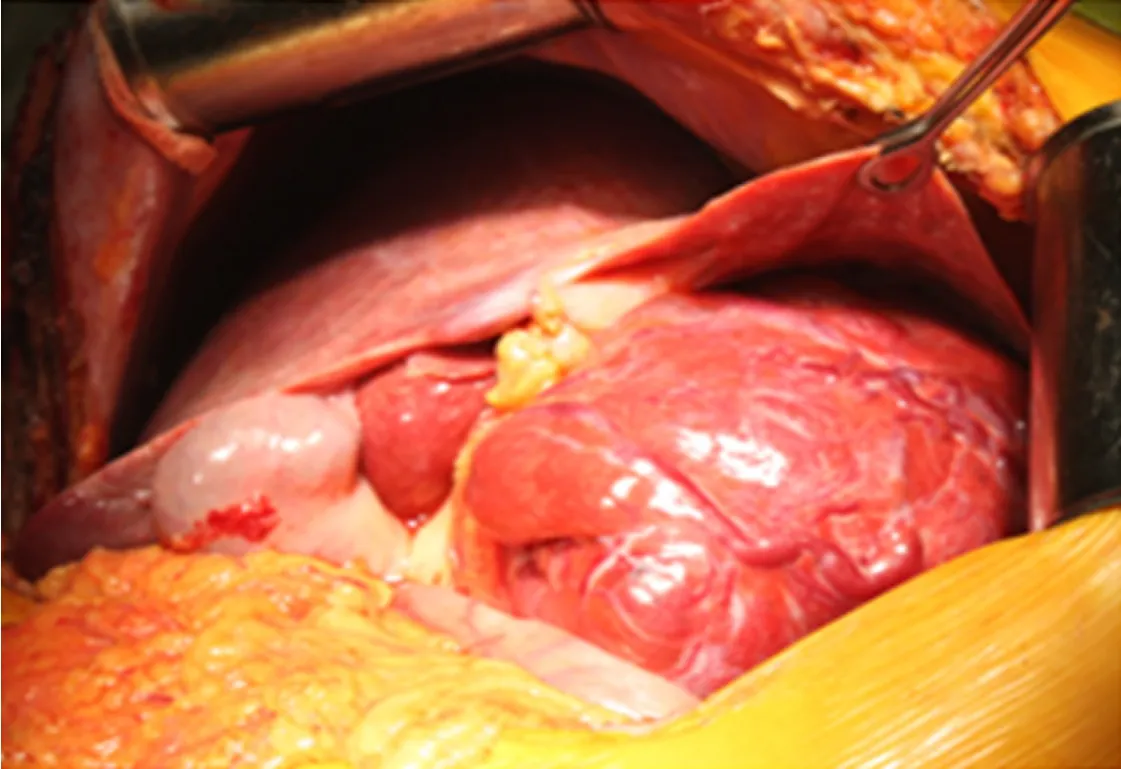
Figure 4 Intraoperative image.

Figure 5 Macroscopic appearance - on the sections, a liver node with areas of reddish-yellow and brown color, with many cavities filled with a brown gelatinous liquid.
OUTCOME AND FOLLOW-UP
The postoperative period was uneventful.Considering the benign nature of teratoma no complementary treatment was indicated.The patient was discharged from the hospital on the 8th day after the operation.Eight years after operation the patient has no complaints, no evidence of teratoma recurrence nor newly formed teratomas were revealed during CT examination in 2021.
DISCUSSION
Hepatic teratoma is rare; to the best of our knowledge, only a small number of case reports exist in the literature (Table 1), and no liver-specific treatment guidelines have been established[5].The successful treatment of an ectopic thyroid gland in the liver, confirmed by morphological and immunohistochemical tests, described herein was very difficult to correctly diagnose preoperatively due to the highly variable instrumental visualization of the tumor and clinical manifestations of this disease.We managed to find only one similar case of hepatic teratoma in the reviewed literature[26].
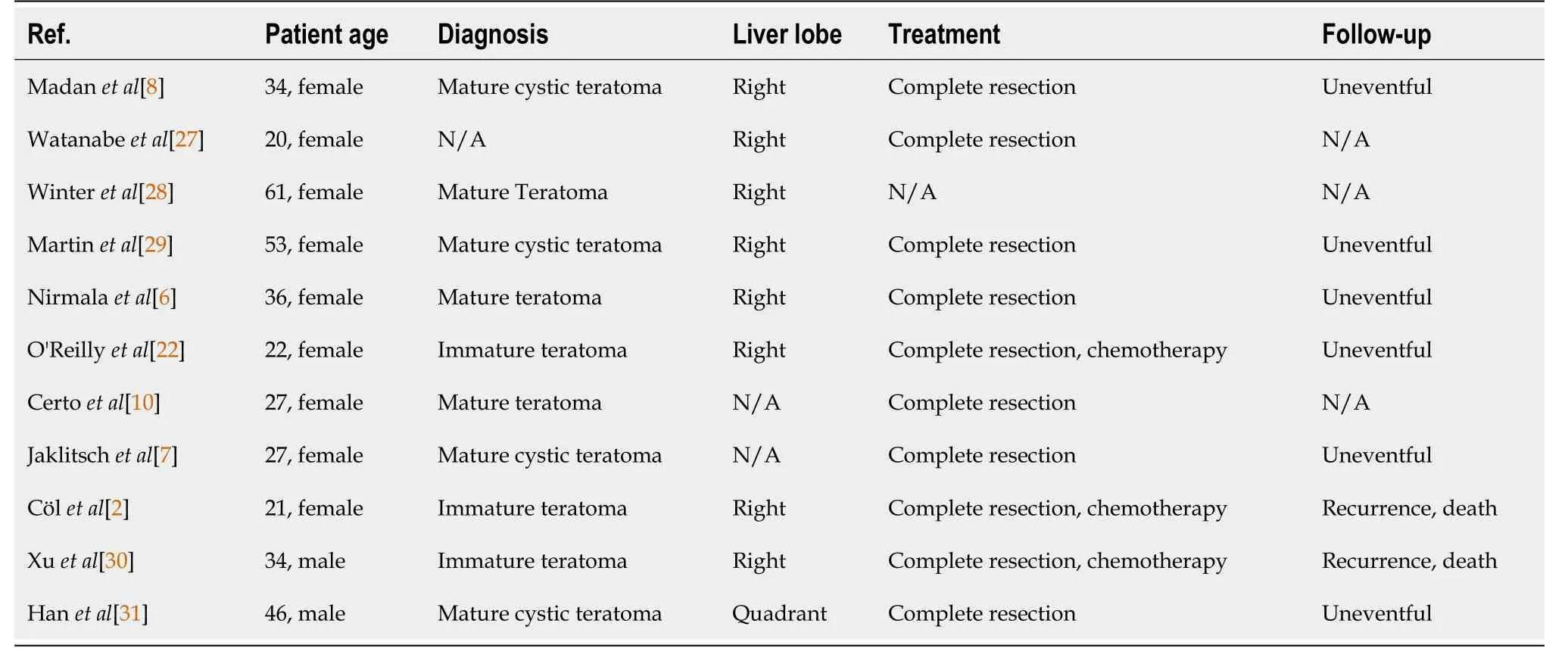
Table 1 Primary liver teratoma case reports
The patient’s medical history provided no evidence of teratoma in thyroid gland tissue.Before the results of the morphological and immunohistochemical tests became available, the patient was considered to have perihilar cholangiocarcinoma.Bearing inmind the state of our patient, we initially planned hepatectomy with a reconstruction biliary tract live-saving procedure.
The immunohistochemical test results demonstrated thyroid follicular epithelium as a result of the focal positive expression of thyroglobulin (clone 2H11+6 E1), TTF-1 (clone 8G7G3/1), and galectin-3 (clone 9C4), overexpression of cytokeratin 8 and 18 (clones B22.1 + B23.1) and negative expression of CD34 (clone QBEnd/10).This clinical case clearly demonstrates the diagnostic challenge of patients presenting with heterotopia of the thyroid gland in the liver simulating perihilar cholangiocarcinoma.Only a comprehensive examination by clinical, biochemical, and radiological methods makes tumor detection possible and allows the identification of such rare conditions.The diagnostic challenges of this condition can be met with the mass-forming type of cholangiocarcinoma.A proper preoperative evaluation, surgical treatment and preparation facilitate positive treatment outcomes.
The patient underwent ovariectomy due to an epidermoid cyst (mature teratoma) of the right ovary 10 years prior to the detection of the hepatic tumor.Unfortunately, micrographs of the lesion were not available.The ovarian teratoma had no signs of malignancy; therefore, no chemotherapy or radiotherapy was indicated.Nevertheless, hepatic teratomas are not metastases from ovarian teratomas, as mature ovarian teratomas cannot spread.Hepatic teratoma is sometimes misdiagnosed as an immature ovarian teratoma if malignant; however, in the current case, the lesion had no signs of malignancy.Consequently, the patient was diagnosed with metachronous teratomas of the right ovary and liver.
In summary, we present an exceedingly rare clinical presentation of heterotopia of the thyroid gland in the liver in an adult patient who underwent surgical resection.The clinical workup included a CT scan, with confirmation of the diagnosis of hepatic teratoma on histopathology.Resection remains the mainstay of treatment.
CONCLUSION
Heterotopia of the thyroid gland in the liver is an extremely rare condition in adults that needs to be considered in the differential diagnosis of solid-cystic neoplasms in the liver and cholangiocarcinoma.Surgical resection remains the mainstay of management, and risk stratification based on histology should determine postoperative surveillance.This case adds to the limited literature on the patient presentation, clinical workup, and management of liver teratomas.
杂志排行
World Journal of Hepatology的其它文章
- Non-alcoholic steatohepatitis in liver transplant recipients diagnosed by serum cytokeratin 18 and transient elastography: A prospective study
- Accuracy of virtual chromoendoscopy in differentiating gastric antral vascular ectasia from portal hypertensive gastropathy: A proof of concept study
- Managing liver transplantation during the COVID-19 pandemic: A survey among transplant centers in the Southeast United States
- Determination of “indeterminate score” measurements in lean nonalcoholic fatty liver disease patients from western Saudi Arabia
- New stem cell autophagy surrogate diagnostic biomarkers in earlystage hepatocellular carcinoma in Egypt: A pilot study
- Trends of alcoholic liver cirrhosis readmissions from 2010 to 2018:Rates and healthcare burden associated with readmissions