Exploring the employment readiness and return to work status of breast cancer patients and related factors
2021-12-11WenminHouQiopingLiXingyuLiuYinghunZengAnySKCheng
Wenmin Hou ,Qioping Li ,Xingyu Liu ,Yinghun Zeng ,Any SK.Cheng
a Intensive Care Unit,The Third Affiliated Hospital of Guangzhou University of Chinese Medicine,Guangzhou,China
b Nursing Department,The Third Affiliated Hospital of Guangzhou University of Chinese Medicine,Guangzhou,China
c Department of Health Service Center,The Affiliated Cancer Hospital of Xiangya School of Medicine,Central South University/Hunan Cancer Hospital,Changsha,China
d Department of Rehabilitation Sciences,The Hong Kong Polytechnic University,Hong Kong,China
Keywords:Breast neoplasms Employment readiness Mental health Patients Return to work Work ability
ABSTRACT Objective:To investigate the employment status,employment readiness,and other factors affecting the ease or difficulty with which breast cancer patients effect their return to work (RTW).Methods:This study adopted a mixed-method design,recruiting participants from among breast cancer patients in a cancer hospital in Hunan from December 2018 to June 2019.We approached 300 individuals,192 of whom ultimately participated in this study.The quantitative part of the study involved several scales:the Patient Health Questionnaire-9 (PHQ-9),the Brief Fatigue Inventory (BFI),the Work Ability Index (WAI),and the Lam Assessment of Employment Readiness (LASER).The qualitative part involved a set of open-ended questions and written responses collected from 41 participants who had already returned to work at the time of data collection.Their written responses mainly concerned factors influencing RTW.Results:Forty-one breast cancer patients had returned to work.The results reported a median total Cognitive Symptom Checklist score of 9.00 (6.00,15.25),a median WAI score of 5.00 (3.50,9.75),a median BFI score of 26.00 (14.75,42.00),a median total PHQ-9 score of 8.00 (5.25,17.00),and a LASER score of 50.35±11.90.Multiple regression analysis showed that the participants’cancer stage,cognitive limitations,depression,fatigue,and work ability were significant predictors of employment readiness(P <0.05).Exploring the qualitative data,we found that higher skill levels,better social support,and a flexible work schedule facilitated RTW;stress,lack of confidence in one’s work skills,depression,and fatigue are all possible barriers to RTW.Conclusion:The findings indicate that breast cancer patients have a low level of employment readiness.Nurses and other healthcare providers can develop relevant interventions to promote employment readiness and ultimately achieve RTW in this study population.
What is known?
· Cancer patients experience a higher risk of unemployment,which increases burdens associated with suffering from and surviving breast cancer.
· The support necessary for breast cancer patients to return to work is essential,so that healthcare professionals,particularly occupational therapists,should address this issue.
What is new?
· This study found that Chinese breast cancer patients experience a lower level of employment readiness and relatively low reemployment rates.
· The combined quantitative and qualitative findings provide important implications for cancer rehabilitation and oncology nursing.
1.Introduction
There were an estimated 19.3 million new cancer cases worldwide in 2020 [1],24% of them in China [2].In 2020,breast cancer was the most common type of cancer[2],and approximately 70%of diagnosed cases were working-age adults[3].With improvements in early detection and advanced cancer therapies,the overall fiveyear survival rate for all cancers rose to 67%[1].The five-year survival rate is now over 90% for patients at all stages of the disease,even advanced ones [4].The mortality rate for breast cancer patients dropped significantly in China in 2020,and the estimated total number of new breast cancer cases was 172,570[2].With the rise in cases and improved survival rates,the burden of breast cancer treatment in China and the total number of breast cancer patients have increased rapidly.
As more working-age women are surviving breast cancer,supporting these women in their return to work(RTW)is becoming an essential aspect of cancer survivorship care [5].As cancer patients experience a higher risk of unemployment,previous research has reported that chances of unemployment among cancer survivors is 37%higher than working-age adults without a history of cancer[6].Numerous research studies have prioritized issues concerning the transition back to work and finding sustainable employment for cancer patients [6-9].Factors that commonly impact cancer patients’ ability to work include physical limitations,psychosocial difficulties such as fatigue and depression,and the side effects of treatment[5,8].Research has also found that a critical determinant of cancer patients’RTW is their employment readiness.Thus,there is a great need to explore the predictors and indicators of employment readiness so that healthcare providers understand how to promote cancer patients’ employment readiness and the ability to return to work.
Nurses-who account for approximately 59% of healthcare providers [10]-work on the front lines of patient care and play a key role in promoting rehabilitation.They are critical allies in facilitating breast cancer patients’ RTW [3].The association between cancer survivorship and work outcomes is well documented in Western countries [6,8,11-13],but only a limited number of studies have been conducted in Asian countries,such as China[14].Therefore,this study aimed to investigate the employment status of breast cancer patients and other factors associated with their employment readiness and to explore the facilitators and barriers of RTW in breast cancer patients.
2.Methods
2.1.Study design
This is a mixed-method study.The first stage involved a quantitative survey via a set of validated questionnaires to investigate breast cancer patients’employment status,employment readiness,and other factors affecting the ease or difficulty of RTW.The second stage was a qualitative study which collected written responses from those participants who had returned to work at the time of data collection.Their written responses mainly concerned factors influencing RTW.
2.2.Ethical considerations
This study obtained approval from the Ethics and Research Committee of the hospital (ELS180124).All participants signed a written consent form.An information sheet about the process of data collection and the purpose of the study was provided to all participants.In the second phase,the researcher further explained the qualitative study process,and a code number of each participant was applied to ensure the anonymity.
2.3.The quantitative phase
2.3.1.Participants
Eligible participants were Chinese women diagnosed with breast cancer who had completed primary cancer treatment in hopes of a cure(stages I-III).The participants were over 18 years old and under 50,and all participated voluntarily in this study.Exclusion criteria were participants who had a breast cancer recurrence,those at advanced stages of the disease,those receiving palliative care,and those with a severe mental illness or cognitive impairment.
2.3.2.Measures
2.3.2.1.A general information sheet.This sheet was used to collect participants’ age,level of education,employment status,marital status,stage of the disease,type(s)of treatment,and the amount of time elapsed since patients had completed their primary cancer treatment.
2.3.2.2.Cognitive symptom checklist.Participants’ cognitive limitations in returning to work were measured using the Cognitive Symptom Checklist(CSC).The Chinese version of the CSC comprises 21 items and a two-factor structure that combines these items to assess task completion and executive function [15].It has strong content validity(>0.8),and internal consistency ranging from 0.84 to 0.95.The test also has a high test-retest reliability (with intraclass correlations between 0.80 and 0.96 [15]).Higher scores indicate more symptoms of cognitive limitations and,therefore,greater work-related limitations [16].Each item has two responses:“yes,”scored as 1,indicating cognitive symptoms,and “no,” scored as 0,indicating no cognitive symptoms.
2.3.2.3.Patient Health Questionnaire.The nine-item Patient Health Questionnaire (PHQ-9) was used to assess participants’ symptoms of depression during the two weeks before they participated in the study.Each item of this questionnaire is scored from 0 to 3,with s combined score of all items ranging from 0 to 27.Higher scores indicate more symptoms of depression.According to Cameron et al.[17],a score of 10 or above on the PHQ-9 indicates that a participant has symptoms of depression,lower than 10 indicates no depression[18].In this study,the internal consistency of the Chinese version of PHQ-9 was 0.82 by Cronbach’s α coefficient.
2.3.2.4.Brief Fatigue Inventory.The Chinese version of the Brief Fatigue Inventory(BFI)was used to assess the severity and impact of fatigue on breast cancer patients.The BFI consists of ten items.The first item asks,“Have you experienced unusual fatigue or tiredness in the last week?”,but not scoring;three items assess the severity of fatigue;and the remaining six items assess the impact of fatigue on cancer patients’daily activities,mood,and relationships[19].Item responses range from 0 to 10.Higher scores indicate greater fatigue.In this study,the Cronbach’s α coefficient for the BFI’s internal consistency was 0.92.
2.3.2.5.Work Ability Index.The Work Ability Index (WAI) was developed by the Finnish Institute of Occupational Health [20].It has been translated into 25 languages,including a test version in simplified Chinese.The single item of the WAI uses the Likert scoring method,ranging from 0 (indicating that a participant is utterly incapable of working) to 10 (which indicates an excellent ability to work).Previous research has shown that the WAI is a reliable,valid,and universal measurement of work ability [21].
2.3.2.6.Lam Assessment of Employment Readiness.The Chinese version of the Lam Assessment of Employment Readiness (LASER)was used to measure participants’ work readiness trajectory.This scale consists of 18 items,using a five-point Likert scale.Higher scores indicate higher levels of work readiness.The internal consistency of the Chinese version of LASER has been measured as 0.79[22].
2.3.3.Data collection
Using the measurement scales listed above,a trained research nurse collected the quantitative data for this study in an outpatient clinic between December 2018 and June 2019 at the cancer hospital,Changsha,China.
2.3.4.Data analysis
Quantitative data analysis was performed using SPSS 21.0 software.Descriptive analyses were presented as mean and standard deviation (SD) or as number and frequency.Comparison of categorical variables was measured using the t-test and ANOVA,and the comparison of continuous variables with employment readiness was measured using Pearson’s correlation.Multiple linear regression was subjected to explore the predicting relationship of study variables with employment readiness.All statistical tests were carried out via a two-sided test,and found statistically significant difference,with P <0.05.
2.4.The qualitative phase
2.4.1.Participants
A total of 41 Chinese breast cancer patients who had returned to work during data collection participated in the qualitative part of this study.
2.4.2.Data collection procedure
The qualitative data were collected in the hospital’s meeting room by written responses.The participants were interviewed with the following open-ended questions.1) Why are you returning to work? 2) What motivated you to return to work? 3) What factors facilitated your return to work? 4) What barriers hindered your return to work? 5) What types of strategies do you suggest for others who wish to return to work? Each interview lasted 30 min.The interview guide was framed by the work and cancer model developed by Feuerstein et al.[23].This model comprehensively aids the conceptualization of work issues and cancer survivorship,helping guide the evaluation and management of cancer patients returning to work[23].
2.4.3.Data analysis
We conducted qualitative content analysis to explore what helped or hindered RTW in breast cancer patients following the three steps developed by Elo and Kyng¨as [24]:1) the written responses were organized into meaning units by words,phrases,sentences conveying similar meaning;2) similar meaning units were grouped and developed into a temporary list of categories;3)the final abstraction process was guided by the Work and Cancer Model [23] until themes were identified.Two other authors (WH and CL) conducted and double-checked the qualitative content analysis to ensure accuracy.The third researcher(YZ)then read the transcripts,cross-checking them before translating them into English.
The qualitative part of this study ensured the rigor of this study by following strategies.This qualitative study adopted the “member checking”strategy;that is,checking with the participants with regard to the accuracy of the results[25].The member check sent to two study participants,and both of them agreed with the interpretations and findings,including the categories and subcategories.In addition,this qualitative part of study adopted an audit trail to ensure the confirmability:the third author used the content analysis on the same set of data independently,yielding similar results.Finally,this study used triangulation methods including qualitative and quantitative approaches to enhance both credibility and confirmability.
3.Results
3.1.Quantitative results
This mixed-method study approached 300 participants,but only 192 agreed to join this mixed-methods study.Of these 192 breast cancer patients,all had completed the quantitative study,and 41 women participated in the qualitative study.Of the 192 participants,21.35%(n=41)had returned to work at the time of the data collection.The mean age of all respondents was 45.36±3.78.Nearly 40% (n=74) had a college-level education or above.More than half(n=105)were married.Approximately 50%of the women(n=95) had an early stage of the disease and sought surgery combined with chemotherapy for treatment.The mean time since they completed their primary cancer treatment was over a year with a mean of 16.28 ± 8.34 months.The detailed sociodemographic characteristics of the respondents are presented in Table 1.The results reported a median total CSC score of 9.00(6.00,15.25),a median WAI score of 5.00(3.50,9.75),a median BFI score of 26.00 (14.75,42.00),a median total PHQ-9 score of 8.00 (5.25,17.00),and a LASER score of 50.35±11.90.Table 1 shows that only the disease stage was statistically significant (t=-3.27,P <0.01).Table 2 shows the correlation of continuous variables with employment readiness:older age was negatively correlated with employment readiness (r=-0.13),and time since completion of primary cancer treatment was positively correlated with employment readiness (r=0.09),but neither variable was significantly associated with employment readiness;other key study variables were significantly correlated with employment variables and entered into the regression model (all P <0.01).
Since one of the primary objectives of this study was to discover predictors of employment readiness in breast cancer patients,we performed comparison,correlation analysis,and multiple linear regression to explore these predictors.Table 3 presents the results of a comparative study of different categorical variables with employment readiness.Table 3 shows the significant predictors of employment readiness:an advanced stage of the disease,cognitive limitations,more significant symptoms of depression,and higher levels of fatigue all were associated with a lower level of employment readiness (P<0.05).Better work ability was associated with higher levels of employment readiness (P=0.041).
3.2.Qualitative findings
Content analysis and coding the data from the written responses brought out two themes:1)facilitators of RTW,and 2)barriers and potential strategies for promoting RTW.A variety of categories underpinned both of these.Summaries of the qualitative content analysis are listed in Table 4.
3.2.1.Facilitators of RTW
Major categories of the facilitators of RTW include socialsupport,financial need,spiritual dependence,enjoying work,achieving self-value,and family encouragement.Of the 41 respondents,28 participants believed that support from family and colleagues helped their RTW.Nearly half of the participants reported that their RTW was motivated by financial strain.
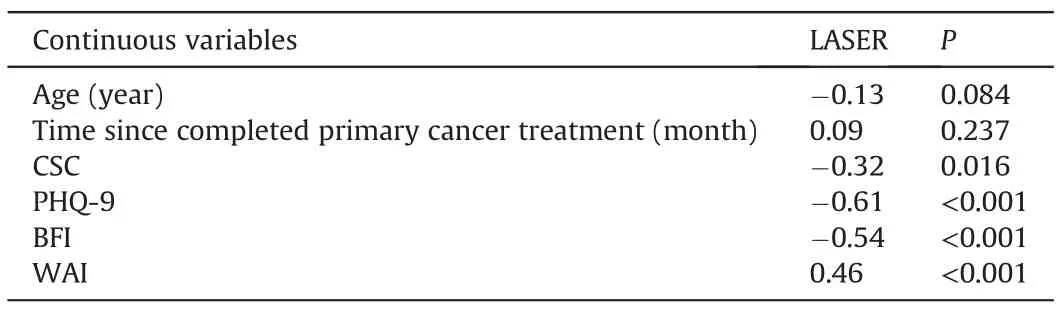
Table 2 Correlation analysis of employment readiness scores with continuous variables (r).
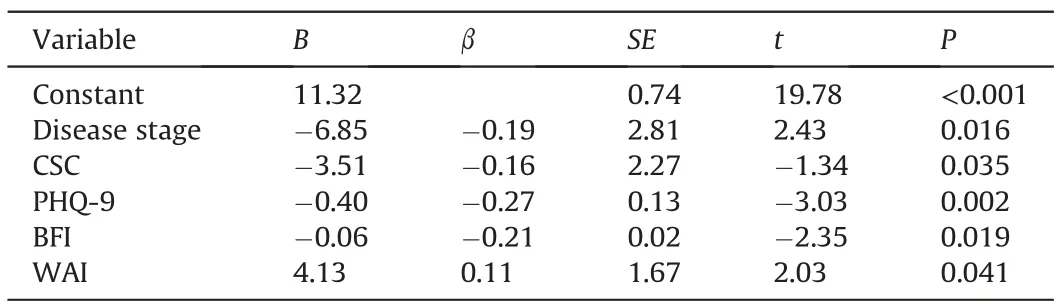
Table 3 Predictors of employment readiness by linear regression (n=192).
“My family’s support (such as from my husband and my son) and my colleagues’support were key facilitators in my return to work;for example,my colleagues help a lot by managing the lab,sometimes helping me with my teaching as well.” (P3,P17,P32)
“My kids are still in primary school,and my cancer treatment used up all my family’s savings so that I had to go back to work to reduce our family’s financial burden.” (P9,P24)
Many women returned to work with the motivations to achieve self-value,meet spiritual needs,and maintain a social network.
“I love my job,and women have to be independent,not just for financial independence,but forworking for society using my professional skills.” (P15)
“When returning to work,I could encounter different things and different people,which makes me happy every day.Being back at work also makes me forget that I am a patient.” (P1)
3.2.2.Barriers and potential strategies for promoting the return to work
The participants identified possible obstacles to their RTW,including psychological difficulties such as self-worry,lack of energy,frequent need to follow up treatment,a lack of confidence in their ability to work,and concerns about aging out of the workforce.
“I think that the major barrier was coming from myself:I was worried that I could not do my job as well as I had before cancer…”(P23,P35)
“Recently I got back to work,and the atmosphere is not as good as before.This year I should have been promoted to a higher-level professional title,but my boss said that sick leave for more than three months meant that I could not be promoted.” (P8)
Strategies for improving the employment readiness of cancer patients include reducing physical and mental demands,setting flexible schedules for cancer patients,adjusting the workload to fit each cancer survivor’s actual health status,and providing continuous training for employees to improve their skills.All of this would be helpful for cancer patients adapting to new work roles.
“Workplaces could promote employment readiness for cancer patients in many ways;after cancer treatment,we still need followup care.If the leaders of each workplace could adjust patients’workload according to their health status,this would help many cancer patients return to work.” (P2,P11,P39)
In addition,many cancer patients hoped that nurses and doctorswould provide instructions on the time frame and information about RTW:
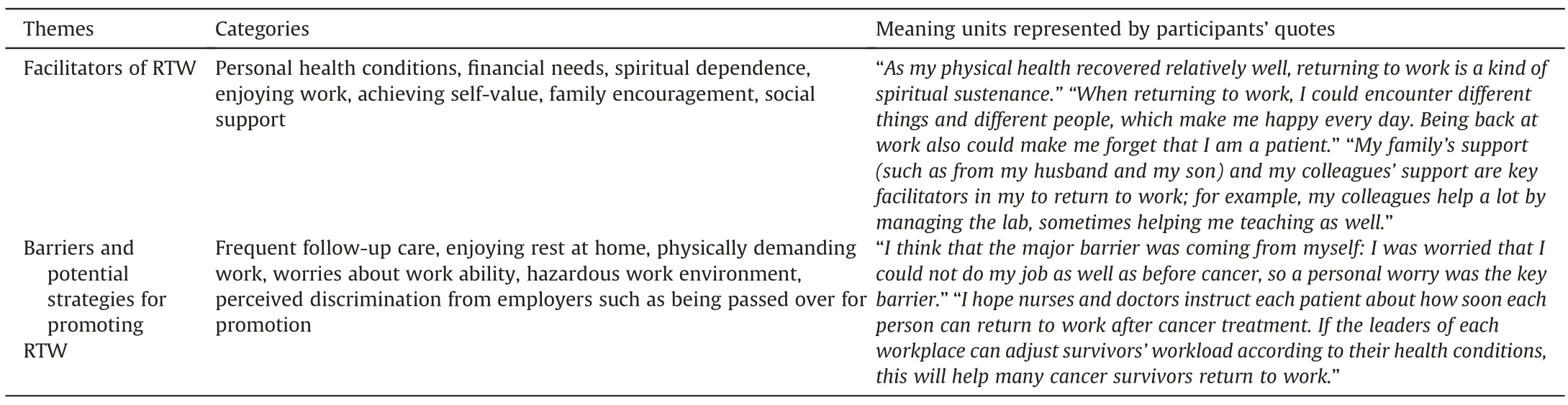
Table 4 Summaries of the qualitative content analysis.
“I wish nurses and doctors would inform each patient about how soon each person can return to work after cancer treatment.”(P5,P21)
4.Discussion
4.1.The prevalence of employment status among Chinese women after breast cancer
As women with breast cancer have a higher survival rate than those with any other type of cancer,RTW is an essential aspect of recovery for these patients.This study found that only 21.35% of Chinese breast cancer patients returned to work after their primary cancer treatment.According to Luo et al.[7],Chinese women diagnosed with breast cancer at a younger age are more likely to return to the workforce upon reaching adulthood.Hence,the RTW of Chinese breast cancer patients is an essential part their care after their recovery.A systematic review reported that 26%-53% of cancer patients globally lose their jobs following the treatment process[9].In the current study,nearly 80%of Chinese women did not return to work following their bout with breast cancer.As this data shows,Chinese women have a far lower employment rate after breast cancer than their Western counterparts.
4.2.Associated factors of employment readiness
This lower employment rate may partially be caused by a lack of employment readiness after breast cancer among Chinese women.An important factor in cancer patients’ RTW is their employment readiness[6].Associated factors include functional difficulties such as cognitive limitations,psychological distress such as higher levels of fatigue,and symptoms of depression[5,8,14,26].Consistent with previous studies[27],those treated at an earlier stage of the disease had better RTW rates here.In addition,more advanced skill levels were positively correlated with higher employment readiness [8].
4.3.Facilitators and barriers of RTW among breast cancer patients
RTW offers a means for cancer patients to reclaim a sense of normalcy,which can be therapeutic[28].The qualitative findings of this study are consistent with previous studies [27-29].They demonstrate that facilitators of RTW include personal,social,and environmental factors such as better physical,psychological,and cognitive health status,financial need,a sense of responsibility and accomplishment,job loyalty,good social support,and,finally,flexible working environment.In contrast,critical barriers to RTW include psychological distress,unsupportive employers,and a lack of information from healthcare providers about RTW after primary cancer treatment.From their workplace,study participants needed practical and psychological support such as flexible working hours to accommodate their health status,and their workplace requiring an RTW timeline from the patient’s healthcare providers.
4.4.Limitations of this study
This study has several limitations.As it is a cross-sectional study,the data could not show how long the breast cancer patients interviewed had been back at work.Future research should use a longitudinal study design to differentiate the various time frames of RTW among cancer patients.In addition,this study investigated employment status but lacked the tools to measure patients’ performance status and the quality of their RTW experiences.Furthermore,this study was only conducted in a single hospital.Future research should complete a similar survey in multiple medical centers.Finally,this study only included patients with breast cancer:future research should explore the impact of RTW on patients with other cancers with high survival rates (such as cervical cancer).
4.5.Implications for nursing practice
While this study has several limitations,its findings indicate the importance of managing patients’ physical,psychological,and cognitive symptoms to improve their employment readiness and work ability.As shown by previous research [6],employment readiness has a positive correlation with RTW in cancer patients,and the fact that oncology nurses are continually actively involved in the ongoing support of cancer patients[30]means that they are perfectly placed to assess the risk factors of employment readiness,and also to develop relevant interventions for promoting RTW in cancer patients.This study’s findings can also inform nurses and other healthcare providers who facilitate and promote RTW among breast cancer patients.Future research should develop rehabilitation strategies to help cancer patients overcome any obstacles in the way of RTW.
5.Conclusion
This study found that fewer than a quarter of Chinese breast cancer patients return to work after treatment in a hospital.The level of employment readiness among participants in this study population is also relatively low.The quantitative results show that factors associated with low employment readiness include suffering from an advanced stage of the disease,cognitive limitations,symptoms of depression,severe fatigue,and poor work skills.The qualitative findings indicate that higher skill levels,more excellent social support,and a flexible work schedule facilitate RTW;stress,lack of confidence in one's work skills,depression,and fatigue are all possible barriers for RTW.Returning to work after breast cancer is essential,not only for patients'financial well-being and sense of self-worth,but also to facilitate their complete recovery.Thus,relevant nursing educational interventions should be developed to address barriers to RTW,which will,in turn,promote rates of RTW among breast cancer patients.
Funding
This research was funded by the National Natural Science Foundation of China (Grant#:72004039).
Data availability statement
Data supporting the findings of this study are available within the article.
CRediT authorship contribution statement
Wenmin Hou:Conceptualization,Methodology,Software,Supervision,Validation,Revision.Qiaoping Li:Conceptualization,Methodology,Software.Xiangyu Liu:Data curation,Visualization,Investigation.Yingchun Zeng:Writing-original draft,Supervision,Software,Validation.Andy SK.Cheng:Writing-reviewing and editing.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
Thanks to all participants who joined this study.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2021.09.001.
杂志排行

International Journal of Nursing Sciences的其它文章
- Second-order problem solving:Nurses’ perspectives on learning from near misses
- Self-care:A concept analysis
- Resilience of nurses at the epicenter of the COVID-19 pandemic in Lebanon
- A study of the relationship between nurses’ experience,structural empowerment,and attitudes toward computer use
- Mobile health applications for the care of patients with breast cancer:A scoping review
- Nursing students’ attitudes toward mobile learning:An integrative review