Self-care:A concept analysis
2021-12-11NicoleMartnezCynthiaConnellyAlexaerezPatriciaCalero
Nicole Martínez ,Cynthia D.Connelly,Alexa P′erez,Patricia Calero
Hahn School of Nursing and Health Science,Beyster Institute for Nursing Research,University of San Diego,USA
Keywords:Concept analysis Chronic disease Delivery of health care Nursing theory Self care Self-control
ABSTRACT Objectives:There is extensive literature from various disciplines on self-care,an important aspect of nursing intervention via evaluation and education,but its meaning remains unprecise due to the difficulty integrating the diverse definitions developed over time across disciplines.Therefore,it is vital to clarify the meaning of self-care and formulate the defining attributes,antecedents,and consequences to self-care.Methods:Walker and Avant’s concept analysis approach was used to analyze the concept of self-care.A search of the literature was completed using the databases CINAHL,PubMed,and EBSCOhost for years 1975-2020;literature search included peer-review articles,full-text publications,and available in English.A total of 31 articles were reviewed,and saturation was reached.Results:An extensive review of the literature revealed salient characteristics that reflected the most frequently used terms associated with the concept.Guided by Walker and Avant’s method,three defining attributes emerged as common themes:awareness,self-control,and self-reliance.Conclusions:A clarified definition was identified:the ability to care for oneself through awareness,selfcontrol,and self-reliance in order to achieve,maintain,or promote optimal health and well-being.
What is known?
· The concept of self-care remains unprecise due to the difficulty integrating the diverse definitions developed over time across disciplines.
· Never has the concept of self-care been more relevant than in the context of an escalation of chronic and communicable diseases,with a massive impact on healthcare systems worldwide.
· It is crucial to formulate the defining attributes,antecedents,and consequences of self-care in order to provide clinicians,researchers,and patients with the ability to communicate clearly with one another and establish well-defined lines of responsibility.
What is new?
· This analysis identified a clarified definition of self-care:The ability to care for oneself through awareness,self-control,and self-reliance in order to achieve,maintain,or promote optimal health and well-being.
· The complexity of self-care,within the context of increasing chronic and communicable diseases,is evidenced by its dynamic ability to transcend multiple disciplines.
· Current and future definitions of self-care would benefit by being multifaceted and addressing a holistic view of the chronic disease patient within a global health context.
1.Introduction
“Since the beginning of humankind,people have taken action to ensure personal safety and have developed strategies to address illness and other health challenges.” [1] Rituals performed by primitive cultures,consumption of special foods to promote health,and knowledge sharing from generation to generation are reflective of self-care strategies [2,3].Despite this realization,self-care was not clearly defined until the late 20th century,when the ability to provide care for oneself gained recognition and started to take precedence as chronic disease increased.
Over time,multiple and often imprecise definitions of self-care resulted in various descriptions across several disciplines.The elusive and complex phenomenon of self-care is reflective of the confusion around the integration of the terms:symptom management,self-efficacy,self-management,and self-monitoring [4,5].The concept of self-care has also been related to broader notions of autonomy,responsibility,and self-direction[5].For this reason,an in-depth analysis of the current knowledge regarding the concept of self-care is required.
McCormack [1] noted self-care is not a new idea [6].Rather,applications of self-care have been present in communities before the healthcare system was formally established;and in some cases,people only rely on self-care due to the lack of healthcare access[7].Despite the belief self-care is inherently human,its utilization became less valued during the scientific era [8].Notably,with the proliferation of nursing and medical schools,people sought care primarily in the acute setting.As technological advances strengthened the knowledge and authority of health care providers,self-care further diminished [8].Not until the latter half of the 20th century did a notable shift in disease patterns from acute to chronic disease facilitate the expansion and necessity of self-care[1,9].At this time,not only was chronic disease management exploding,but support groups,particularly the inception of Alcoholic Anonymous in 1935,strove to define the gaps in their care.This gap echoed the inevitable need for self-care[1].
As previously inferred,the origin of the concept of self-care evolved within various social movements,including women’s and wellness movements.These movements created a societal context that fostered the development of the concept[10].In addition,selfcare intervention also gained attention because of the increased focus of improving the intrinsic capacity of older people to manage their chronic diseases[7].Society embraced autonomy,sparked the inception of support groups,and motivated self participation in health care [11].The acceptance and awareness of a new facet to healthcare continued to gain momentum as the population and chronic diseases increased [4,5,12].
Never has the concept of self-care been more relevant than in the context of the COVID-19 pandemic.This epidemic outbreak has had a massive impact on healthcare systems worldwide,including on primary care settings [13].In many countries,as the pandemic spread,health care services became overloaded,non-urgent services were drastically reduced [14-19],and staff responsible for self-management support of chronic patients was put on hold[20].In order to remain connected to patients,primary care was restructured from in-person to virtual care using Telehealth[21,22].This profound transformation of healthcare delivery has evidenced the importance of patients’self-care behaviors to decrease the risk of contagion and remain healthy [23];as well as healthcare professionals’ education and support of patients amid the ongoing COVID-19 pandemic [24].
The objective of this concept analysis is to synthesize the extensive literature obtained from various disciplines to formulate the defining attributes,antecedents,and consequences to self-care.Clarity is needed to differentiate between the numerous characteristics that are present and used.It is essential the concept of selfcare is defined in order to provide clinicians,researchers,and patients with the ability to communicate clearly with one another and to establish well-defined lines of responsibility [25,26].
2.Selection and aims of the concept analysis
Researchers should select a complex concept that plays a significant role in nursing[27].Therefore,the concept of self-care was selected since it is considered a focal point of nursing practice as an intervention nurses provide via evaluation and education to enable patients to restore health,independent living,and well-being [5].
Considering the various unprecise descriptions of self-care across disciplines,clarity is needed to provide clinicians,researchers,and patients with the ability to communicate clearly with one another and establish well-defined lines of responsibility[25,26].Thus,the researchers performed an in-depth analysis of the current knowledge regarding the concept of self-care.
3.Methods
3.1.The concept analysis approach
The Walker and Avant’s method of analysis was used to examine the concept of self-care [15].These iterative steps include as follows:1) selecting a concept;2) determining the aims of the analysis;3) identifying all possible uses of the concept in nursing;4)defining concept attributes;5) constructing a model case;6) constructing borderline,related and contrary cases;7) identifying antecedents and consequences of the concept;and 8) defining empirical referents of the model.Careful examination of the implications of this concept provides an understanding of the phenomena.The Standards for Reporting Qualitative Research (SRQR)guideline has been utilized to improve transparency[28].
3.2.Data sources
A comprehensive and broad search for the term self-care was entered in three online databases (National Library of Medicine PubMed,CINAHL,and EBSCOhost).This search included peerreview articles published between January 1975 and October 2020.To further refine the search process and capture pertinent literature,the terms,self-efficacy,self-control,and resilience,were included in the search;the search generated 535 hits.Inclusion criteria included English,full-text publications,and academic journals.Exclusion criteria included non-English language articles,limited text publications,non-academic journals,and articles that did not address the key terms self-efficacy,self-control,or resilience.Utilizing the exclusion criteria narrowed the search,and a final total of 31 articles were reviewed to identify self-care attribute common themes.The reference lists of all identified papers were searched for relevant cited articles,and saturation was reached.
Utilizing the Walker and Avant process,all 31 articles were read in their entirety,and a data extraction table was constructed to include the reference and attributes(Table 1).Representation from multiple disciplines,including nursing,medicine,psychiatry,pharmacy,social work,and business,was demonstrated in the review.Articles were retrieved from various countries,including Canada,China,England,South Korea,and the United States.An Excel spreadsheet was created to document the key terms that were included in each of the final 31 articles,including self-care,self-efficacy,self-control,and resilience.This concept analysis was exempt from Institutional Review Board (IRB) approval;the research did not involve human subjects.
4.Results
4.1.Identifying all possible uses of the concept in nursing
Reflective of the diverse wealth of literature,the concept of selfcare can be implemented in a variety of settings,including nursing and nursing theory,medicine,psychology,business,and lifestyle.Throughout these disciplines,a myriad of interpretations of the concept is delineated from the rich variety of perspectives;consequently,the information is fragmented.Despite this array of information,Dictionary.com[54]and the American Heritage Science Dictionary [55] define self-care as the care of oneself withoutmedical or other professional consultation,assistance,or oversight.The WHO compounded this definition:including the individual,family,and community,who in turn,promotes,prevents,maintains health,and copes with illness and disability [56].In addition,the WHO identified fundamental principles of self-care,which include autonomy,self-efficacy,empowerment,community involvement,and community empowerment [57].
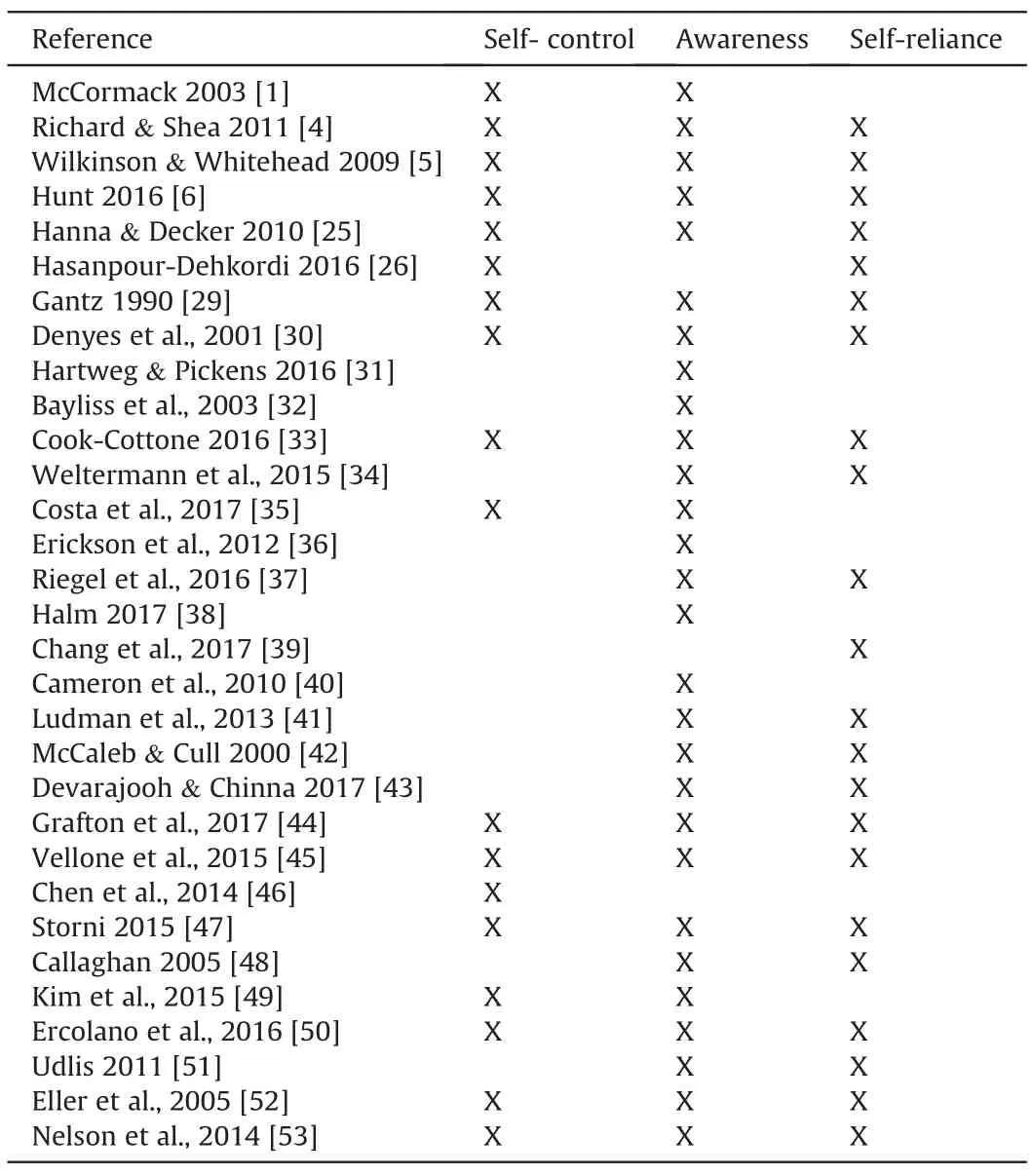
Table 1 Self-care attributes.
Within modern medicine,this definition is most commonly reflected in preventative health and chronic disease management.Gantz further defines this perspective with a discussion of the two parallel paradigms of self-care:a health care model that consists of the health care delivery systems and the lay model based in selfhelp groups,family practices,supplemental therapies,and the media [29].Four levels of self-care performance have emerged:responsible,formally guided,independent,and abandoned [4].Thus,the multidimensional concept of self-care reflects a fluid component to the overall care of a person.
According to Denyes and colleagues,the trailblazer of self-care in nursing theory,Dorothea Orem,defined self-care as the learned and deliberately performed action utilized to regulate development and functioning [30];her Self-Care Deficit Theory(SCDT) exemplified this [12].Within this theory,the self was not only the agent of action,but also the object of action.Orem discussed self-care as a developmental process suggestive of health,life,and well-being [12,31].This dynamic process reflected the reciprocity between humans and their environment,and it has transcended nursing since Orems initial analysis in 1956.SCDT has significantly influenced nursing knowledge and has provided a conceptual framework to guide practice[1].Orem’s framework also suggests that every person has the capacity to become a self-care agent and practice self-care activities,and nurses can help the patients achieve their self-care goals [58].
Others have expanded Orem’s description of self-care.Chambers argued the self-care continuum flows from individual responsibility to self-management of illness to shared care with a provider [59].Within nursing practice,self-care emerges as an intervention nurses provide via evaluation and education to enable patients to restore health,independent living,and well-being.As nurses practice ethically,persons with chronic disease will be more effectively managed with the utilization of self-care[5].
Similarly,medical providers incorporate self-care when encouraging patient communication regarding relevant observations and symptoms.This assists the provider with therapeutic and diagnostic decision making[32,57].The direct communication lays the foundation for the patient to achieve optimal therapeutic outcomes.The literature supports self-care functions as one of the primary forms of care for chronic disease patients when they are expected to make day-to-day decisions about self-management and administration [60].
Within the discipline of psychology,practitioners incorporate self-care into their practice when determining what precipitates a behavior or emotional process.Self-care in this context is evaluated as health belief,clarification of values,decision making skills,and the component of self [29].In addition,Barnett and colleagues attest self-care is also necessary for health care providers themselves [61].Not only will this care decrease burnout,distress,and impaired professional competence,but it also creates a supportive and healthy professional climate[61].Self-care activities practiced by health care providers have helped to reduce occupational stress and have shown an increase in resilience,which is a crucial ability a person develops to recover from challenges and stress faced in the workplace [57].This self-care manifests via a myriad of measures from physical exercise to psychological therapy and is incorporated by all persons.
In addition to the health-related disciplines,self-care transcends all avenues,including leadership,business,and lifestyle.It thrives as a relevant business from the standpoint of reducing health care costs,as well as product line enhancement [29].Furthermore,national executives and leaders have integrated self-care as a part of their employee development workplace regimen[62,63].Self-care application in the context of daily life includes activities such as exercise,meditation,yoga,complementary and alternative therapies.
4.2.Defining concept attributes
Walker and Avant suggest the“heart of the concept analysis”is the process of defining the attributes [27].An extensive review of the literature revealed salient characteristics reflecting the most frequently used terms associated with the concept [27].These terms include awareness,self-control,self-reliance,health literacy,self-efficacy,social support,resources,cognitive level,and readiness.Notably,three defining attributes emerged as common themes:awareness,self-control,and self-reliance (Table 1).
4.2.1.Awareness
Cook-Cottone and colleagues suggest that when development and health is normal,individuals do not consider health concerns[33].Instead,an awareness is eminent for the person to attend to their needs.This awareness coupled with knowledge and skill adds to the empowerment of the individual to motivate their own behavior and quality of life[34,35,64].Self-monitoring depends on awareness,measurement,and interpretation of the symptoms[65].Symptom recognition and evaluation then triggers self-care[36,37].
4.2.2.Self-control
According to Denyes and colleagues,self-care is a product of a person acting as a unitary being and engaging in regulation and control of their self and emotions [12,30,33].Cook-Cottone and colleagues support this contention that regulation and control of the self are essential to achieve cognitive approaches to prevention,regulation,and self-care[33,38,64].Furthermore,the WHO argues that control and prevention of a disease reflect self-care practices[34,56].This self-control is reinforced with awareness and selfreliance.
4.2.3.Self-reliance
In order to successfully perform self-care,the individual must maintain self-reliance.The concept of self-reliance is deeply embedded in our thinking of chronic disease management and is reflected in medication administration and adherence to health care plans[66].Self-reliance directly influences the inclusion of the patient and their family into self-care,and it mirrors the person’s resilience and perseverance [39,67].
4.3.Constructing cases
Constructed cases illustrate the concept by incorporating the attributes,antecedents,and consequences.A model case includes all the defining attributes,a related case represents a connection to the concept,and a contrary case is a clear example of when the concept is absent [27].
4.3.1.Model case
Last week while hiking Mount Whitney with his wife,Carl,a 45-year-old male,slipped on a slick rock and sustained a 4-cm superficial wound to his right leg.He attended to the wound by cleaning it daily with soap and water and providing adequate dressing changes.The wound healed completely within one week,and Carl was able to resume hiking with his wife.
The above case is an effective representation of a model case because Carl has demonstrated the defining attributes of awareness,self-control,and self-reliance.When he became aware of the injury,he was in control and had enough self-reliance to provide adequate care for himself and appropriately attended to his wound.His self-care was supported by his previously present self-efficacy,cognition,self-agency,adequate resources,and a supportive cultural and social network.
4.3.2.Related case
Ned,a homeless 54-year-old male with schizophrenia and type 2 diabetes mellitus,sustained a wound to his right leg when he slipped in a canyon.He has not been able to take his medications as prescribed for two months due to the fact that his belongings,including his medications,were stolen from him.Though Ned was aware of the injury,he did not treat the wound,and his entire leg became swollen,red,and hot.Two weeks after the initial injury,his friend called 911 because Ned appeared to become febrile with an altered mental state.Ned was transported to the emergency department (ED).
This is a related case because although Ned lived independently and was aware,he did not have the defining attributes of selfcontrol and self-reliance.Thus,he did not provide self-care to his wound.This lack of reliance and control resulted in a poor outcome.
4.3.3.Contrary case
David,a 79-year-old male,sustained a mechanical fall in his home bathroom when he was exiting the shower.He was found by his wife unconscious on the bathroom floor with a laceration to his forehead and to his right leg.He was transported to the ED via ambulance.Upon arrival to the ED,David quickly decompensated and inevitably needed to be intubated.Computed tomography(CT)of his head revealed an extensive subdural hematoma.He was admitted to the ICU and received full care from the medical and nursing staff who attended to all his needs.
In this contrary case,David does not have the defining attributes of awareness,self-control,and self-reliance in order to self-care for his wounds.This deficit is secondary to his impaired cognitive level,ineffective self-agency,lack of self-efficacy,and critical medical state.Though this may be a sudden change in person and situation,David is presently unable to provide self-care.
4.4.Identifying antecedents and consequences of the concept
The iterative process of concept analysis defines antecedents as incidents that must occur prior to the occurrence of the concept[27].An individual’s ability to carry out self-care is directly related to his or her knowledge,motivation,skill,and confidence which in turn has been influenced by the physical,psychological,social,and cognitive context [35,40-42].Thus,the antecedents derived from the literature were categorized into patient-related and systemrelated (Fig.1).
4.4.1.Patient-related antecedents
Patient-related antecedents include self-efficacy,cognition,a triggering event,and self-care agency [43-45].A strong body of evidence supports a direct correlation between self-efficacy and self-care [41,44,45,68].This relationship reinforces the connection between confidence and self-care maintenance and management[44].Similarily,cognition is essential for effective self-care [40].Though a patient’s knowledge and expertise are critical to implementing and understanding chronic self-care,Chen and colleagues demonstrate that self-efficacy is more closely interconnected to self-care than health literacy[46,47].Self-agency is a broad concept that encompasses foundational capabilities,self-care operation,resources,and power components [30,47,48].Thus,it progresses along the physical and cognitive continuum.Self-agency is built upon the developmental levels of a person and their needs and desires to practice self-care[65].
4.4.2.System-related antecedents
System-related antecedents include cultural factors,social support,and access to adequate resources [4,32,49].According to Benbow and Deacon,people should be provided with instructions,supplies,and all the necessary resources that enable them to perform self-care [69].This establishes a supportive cultural and social network and facilitates access to self-care via a systemrelated foundation [32].Kim and colleagues contend social support is comprised of three categories:social connectedness,perceived support,and actual social support [49].
4.4.3.Consequences
Walker and Avant argue that consequences result secondary to the occurrence of a concept [27].These consequences reflect both psychological and physical goals[50].The literature depicts several consequences resulting from self-care,including the achievement of desired outcomes,decreased risk for complications,symptom control,decreased health services utilization,and increased patient satisfaction [4,6,51,70];thus,enhanced coping,improved sense of control,deepening sense of meaning,well-being,and quality of life are optimal consequences of self-care.
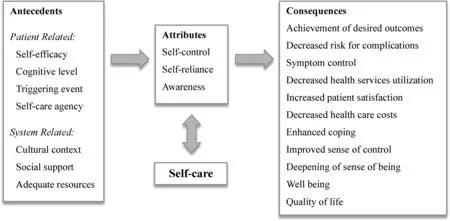
Fig.1.Antecedents,attributes,and consequences of self-care.
Potential negative outcomes may arise when a person does not desire to ask for help or delays help due to their beliefs that they can provide adequate self-care.This may be secondary to low health literacy,decreased cognition,and/or a mental health history.Selfcare can also potentially result in self-harm if the person does not have the appropriate means to provide care or if they have received inappropriate information from sources such as the internet [1].Self-care interventions play an important role in situations where people have no access to health promoting interventions or have some distrust in the health care system.This is why it is crucial to promote high quality self-care,so people can receive appropriate information regarding the self-care intervention,as well as supporting people in acquiring the skills and resources needed to practice self-care [7].Furthermore,self-care is thought of as an opportunity by most patients and health care providers,but to others it may be considered to be a threat.
4.5.Defining empirical referents of the model
The measurement of self-care involves the utilization of diverse empirical referents.Though several instruments exist,a lack of a single comprehensive measure creates a gap in knowledge.In particular,one single measure does not address the person’s spiritual health,psychiatric well-being,race,ethnicity,in addition to the already established criteria.Instead,most assessments focus on cognition,self-efficacy,and self-agency [41,43,52].It would behoove an evaluator to assess the patient’s perspective of the positive or negative involvement of the medical provider.As such,an integrative model is needed.
Empirical referents within the nursing realm most frequently utilize instruments that measure self-care agency and self-care practice [48,71,72].Specific pediatric instruments are also available [42,73,74].Another example includes the Health-Promoting Lifestyle Profile II (HPLPII) scale,which measures self-care behaviors focusing on health promotion and preventative measures[75].Becker and colleagues developed the Self-Rated Abilities for Health Practices (SRAHP) scale to measure self-care and self-efficacy through the evaluation of a person’s performance in healthpromoting behaviors [76].Additionally,the Exercise of Self-Care Agency(ESCA)evaluates the person’s ability to care for oneself[77].
Even more standardized measures exist within the discipline of psychology,including the Self-care Behavior Inventory,Perception of Competence Scale,Flourishing Measure,Contributor to Distress Measure,and Maslach Burnout Inventory-Human Services Survey[78-82].Similar to the beforementioned instruments,these instruments assess self-determination,confidence,capability,competence,and engagement.Despite a plethora of instruments to measure self-care,a comprehensive and integrative instrument is not available.
5.Operational definition
The results of the literature search outlined the concept and its defining attributes.Consequently,self-care is further defined as the ability to care for oneself through awareness,self-control,and selfreliance in order to achieve,maintain,or promote optimal health and well-being.Three attributes were identified:awareness,selfcontrol,and self-reliance.Self-efficacy,self-agency,a triggering event,access to adequate resources,and both cultural and social support preceded as the antecedents.
6.Discussion
As a major driver in the development of self-care knowledge,the growing costs of health care can be interpreted as an indication for need [83].Nelson and colleagues predict self-care will evolve into the principal source of care.As chronic disease proliferates,the need for people to take more responsibility for being the principal provider of their own care will surge [53].The pendulum,in turn,sways from the expensive,specialized care towards high-value selfcare [53].This will also transcend into the medical provider’s understanding of patient education as it is incorporated into their academic curriculum.Self-care interventions allow the individual the opportunity of making informed decisions about their health by having more choices of care which are more accessible and affordable [7].Eventually,the driving force of shared decisionmaking,coproduction,and competent self-management will echo self-care methodology reinforced within patient education and instructions [84-86].
The COVID-19 pandemic has highlighted the vital role self-care interventions play in lessening the effects of disease and saving lives.Personal self-care behaviors such as wearing masks and social distancing,and healthcare systems transformations,for instance,the prioritization of self-care interventions with different patients have been an asset during lockdown periods[87].The expansion of self-care is not exclusive to the current pandemic,but has been the focal point of healthcare systems worldwide,as evidenced by the development and expansion of self-care programs and policies regarding a variety of chronic and infectious diseases [88,89] and mental health [90].Cultural health beliefs and values heavily influence lifestyle choices and health-promoting practices [91];fatalism,collectivism,familism,gender roles and cultural norms have been known to play a critical role in dietary and medication adherence,and the use of alternative medicine [91,92].Significant differences have been found in patients’ self-care regarding receiving an annual flue-shot,adhering to a low-sodium diet,or weighting themselves regularly by country and continent [88].Thus,the relevance of a culture-and country-specific approach to understand self-care,and design effective,targeted interventions.
The synthesis of this information highlights the intricacy involved with self-care within the context of chronic disease,and it exemplifies its dynamic ability to transcend multiple disciplines.The findings suggest a multifaceted definition of self-care addressing a holistic view of the chronic disease patient within the present literature.
7.Conclusion
The analysis of self-care identified a clarified definition:the ability to care for oneself through awareness,self-control,and selfreliance in order to achieve,maintain,or promote optimal health and well-being.Chronic disease patients ultimately spend more time managing their conditions and providing self-care than they spend with their providers.Legitimizing this realization as an equal aspect of medical care within the context of chronic disease reinforces the importance of disseminating this information to both professional and lay audiences [1].Self-care is an active decisionmaking process that enables people to effectively engage in their care.
Funding
This work was supported in part by the Achievement Rewards for College Scientists (ARCS) Foundation.
Ethical considerations
This concept analysis was exempt from Institutional Review Board(IRB) approval;research did not involve human subjects.
CRediT authorship contribution statement
Nicole Martínez:Conceptualization,Methodology,Formal analysis,Investigation,Data curation,Writing -original draft,Project administration,Funding acquisition.Cynthia D.Connelly:Conceptualization,Methodology,Validation,Writing -review &editing,Supervision.Alexa P′erez:Methodology,Formal analysis,Investigation,Validation,Writing -review &editing.Patricia Calero:Methodology,Investigation,Validation,Writing-review&editing.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgements
A special thank you to Dr.Eileen Fry-Bowers,PhD,JD,RN,CPNP,FAAN for her research guidance and support in this study.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2021.08.007.
杂志排行

International Journal of Nursing Sciences的其它文章
- Second-order problem solving:Nurses’ perspectives on learning from near misses
- Exploring the employment readiness and return to work status of breast cancer patients and related factors
- Resilience of nurses at the epicenter of the COVID-19 pandemic in Lebanon
- A study of the relationship between nurses’ experience,structural empowerment,and attitudes toward computer use
- Mobile health applications for the care of patients with breast cancer:A scoping review
- Nursing students’ attitudes toward mobile learning:An integrative review