Dignity and its related factors among older adults in long-term care facilities:A cross-sectional study
2021-12-11DieDongQianCaiQiongZhiZhangZhiNanZhouJiaNingDaiTingYuMuJiaYiXuCuiZhenShen
Die Dong,Qian Cai,Qiong-Zhi Zhang,Zhi-Nan Zhou,Jia-Ning Dai,Ting-Yu Mu,Jia-Yi Xu,Cui-Zhen Shen
School of Nursing,Zhejiang Chinese Medical University,Hangzhou,China
Keywords:Aged Health Long-term care Respect Skilled nursing facilities Sociological factors
ABSTRACT Objectives:This study aimed to explore the dignity and related factors among older adults in long-term care facilities.Methods:Cross-sectional data were obtained from a sample of 253 Chinese older adults dwelling in long-term care facilities.Dignity among older adults was measured using the Dignity Scale,and its potential correlates were explored using multiple linear regressions.Results:Results showed that the total score of the Dignity Scale is 151.95 ± 11.75.From high to low,the different factors of dignity among older adults in long-term care facilities were as follows:caring factors(4.83 ± 0.33),social factors (4.73 ± 0.41),psychological factors (4.66 ± 0.71),value factors (4.56 ± 0.53),autonomous factors (4.50 ± 0.57),and physical factors (4.38 ± 0.55).A higher score of the Dignity Scale was associated with higher economic status,fewer chronic diseases,less medication,better daily living ability and long-time lived in cities.Conclusion:Older adults with low economic status,more chronic diseases,and poor daily living ability,taking more medications,or the previous residence in rural areas seem to be most at low-level dignity in long-term care facilities and thus require more attention than their peers.
What is known?
· Lack of guarantees for the dignity of older adults in long-term care facilities can lead to depression and even accelerate death.
What is new?
· Dignity is challenged most by physical and autonomy factors.
· Older adults with low economic status,more chronic diseases,more medications,poor daily living ability,or previous residence in rural areas seem to be most at risk of losing dignity in long-term care facilities.
1.Introduction
With the progress of society and the acceleration of the aging process,support for the elderly has attracted more and more attention,and long-term care facilities have gradually entered the scene as the elderly’s choice.Compared with living in the community,long-term care facilities can provide more professional medical care services and organize more abundant recreational activities,thereby earning wide recognition from the public [1,2].With their rich life experience,the elderly tend to pay more attention to dignity [3].However,at present,the care services provided by some long-term care facilities could not fully meet the actual needs of the elderly,and the dignity of the elderly is vulnerable to neglect [4,5].
Personal dignity is a type of dignity that relates to a sense of worthiness,individualistic,tied to personal goals and social circumstances,and can be taken away or enhanced by circumstances or acts from others [6].It should be distinguished from basic dignity,which is the inherent dignity of each human being and can be regarded as a universal and inalienable moral quality [7].Personal dignity is important to understand,assess and preserve within the context of health care.The dignity we mention in this paper is the concept of personal dignity.
For the elderly,dignity is almost equal to the quality of life in old age,and some older adults even pay more attention to dignity than to life [8].The lack of guarantees for the dignity of older adults in long-term care facilities can lead to depression and even accelerate death[9].Nurses in long-term care facilities should be aware of the importance of dignity and maintain the dignity of the elderly in practical work.A key step to help older adults maintain their dignity is to identify factors related to its impairment.Oosterveld-Vlug[10] interviewed 30 older people in long-term care facilities and found that disease was the direct cause of the elderly’s loss of dignity,and it would affect dignity by threatening all aspects of their private and social lives.Later in a quantitative survey,she also found that pessimism,gender,and heavy dependence influenced the sense of dignity among the elderly [11].Franklin [12] summarized 14 studies about views on dignity of elderly nursing home residents and pointed out that the way of dignity existence was treating any sick elderly as an independent individual,by letting them decide their own behavior,understand,judge and choose the surrounding environment or things by themselves.Besides considering the factors related to disease and individuals,Naden[13]interviewed 28 nurses in long-term care facilities and learned the main reasons for the loss of dignity of the elderly from a social perspective,including the feeling of being abandoned,lack of sense of belonging,the omission of nurses,the feeling of being despised and violence against the elderly.However,research on the dignity among older adults dwelling in long-term care facilities in China was infrequent.
Compared with Western culture,traditional Chinese culture has certain unique traits.Chinese elderly value family and‘face-saving’more and have weakness in communication and self-expression,all of which lead to a culture-specific meaning of dignity and its influencing factors.This study aimed to elucidate the dignity status of older adults in long-term care facilities in China and identify its potentially related factors.Understanding these two aspects can assist caregivers in identifying individuals who are at risk of impaired dignity and provide guidance for effective interventions.
Fig.1 shows an overview of the theoretical basis,which is the framework of the study,guiding our research design and data analysis.The theoretical basis is the result of combining literature review and previous clinical practice by our research group.
Maslow’s hierarchy of needs depicted hierarchical levels from the bottom upwards:physiological needs,safety,love and belonging,esteem,and self-actualization,with the belief that when a low level of need is met,needs higher up should be attended[14].Based on Maslow’s theory,in the development of geriatric nursing,multi-level needs of the elderly should be paid attention to;thus,a pension model is required that meets their economic and material needs and concerns for their social and spiritual needs.Respecting the rights and personalities of older adults and preserving the dignity of older adults in long-term care facilities is an important aim and the central principle of geriatric nursing.Continuity theory emphasizes the need for people to maintain the connection between the past and the present,with people only needing to maintain their required level of social participation in order to achieve their maximum happiness and dignity [15].According to continuity theory,caregivers should do as much as possible to help the elderly live and maintain their previous human needs and required level of social participation.They should also assist the elderly in achieving full dignity,whether they live in the community or a long-term care facility.
2.Methods
2.1.Participants
A total of 260 participants were recruited from three long-term care facilities in Hangzhou,a city in Southeast China.These longterm care facilities provide a full range of elderly care services,from daily care to medical rehabilitation.We used a convenience sampling method and collected data from July to September 2018.All the 260 participants met the inclusion criteria,but 7 of them did not agree to participate in the study.Finally,253 older adults were included in the study.Participants were excluded if they 1) were≤60 years of age;2) were palliative care or terminal cancer patients;3) had dwelt in long-term care facilities for less than half a year;4)had impaired hearing,vision,or cognition that may inhibit them from giving consent and answering the questionnaires;and 5)had a history of mental illness or disorder.The date of admission and history of mental illness or disorder of each participant were acquired from their responsible physicians and nurses.
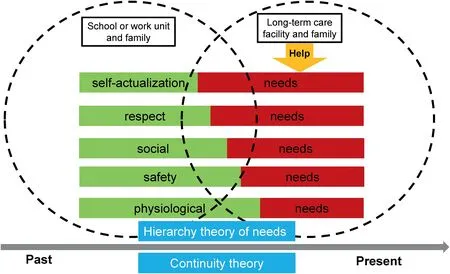
Fig.1.Overview of the theoretical basis.
2.2.Sample size
Before the study,we wanted to achieve 80% power in the analysis with 20 independent variables (k=20),indicating a 20%probability of committing a type II error.We conservatively estimated a medium effect size (R2=0.165) of the relationship between the dignity and older adults correlates according to a study[16].For k=20 and 80% power at dfres(the number of residual degrees of freedom)=20,we found λ=38.5[17].Using the formula,a minimum of 195 participants were required.
2.3.Measures
Dignity was assessed using a self-developed scale,the Dignity Scale for older adults in long-term care facilities (unpublished),which was mainly developed on the basis of the literature review[18,19]and a previous qualitative interview in three long-term care facilities in Hangzhou by our research group[20].The scale aims to examine Chinese older adults dwelling in long-term care facilities.It consists of 32 items(symptoms or experiences)categorized into 6 dimensions:physical factors,autonomous factors,social factors,value factors,psychological factors and caring factors.For each item in the Dignity Scale,respondents were asked to what extent it influenced their sense of dignity on a five-point scale (1=very serious,2=serious,3=moderate,4=mild,5=none at all).The total score of the Dignity Scale was the sum of the scores from the six dimensions.The scale results presented a total score ranging from 32 to 160,with a higher score indicating a higher level of dignity.
The newly developed questionnaire was reviewed for relevance,clarity and linguistic appropriateness by 10 nursing experts (5 academics,3 nurse managers and 2 experts in clinical nursing).We tested the reliability and validity of the questionnaire on 296 elderly people from the abovementioned long-term care facilities and then selected 50 people for the test-retest reliability test.The Item Content Validity Index was over 0.78 and the Scale Content Validity Index was 0.98,indicating that the Dignity Scale had good content validity.Reliability analysis was conducted before the Dignity Scale was distributed.Test-retest reliability of the Dignity Scale was calculated at a 14-day interval.Internal consistency was calculated using Cronbach’s α coefficient.The test-retest reliability was 0.828,and Cronbach’s α coefficient was 0.908.Construct validity was examined using a principal component analysis with varimax rotation.Six factors were extracted,and the total percentage of variance was 73.121%,which suggests that the Dignity Scale has good validity.
Sociodemographic data included gender,age,previous residence,religion,marital status,educational level,pre-retirement occupation,economic status,and type of health insurance.Disease-related data included chronic diseases,medications,and daily living ability.The chronic diseases and medications of each participant were acquired from their respective physicians and nurses.Economic status was determined from the subjective assessment of the participants.At present,two main types of health insurance are available in China:Urban Employee Insurance (UEI)for all employed residents and Urban and Rural Resident Medical Insurance (URRMI) [21].URRMI covers all unemployed residents,including Urban Resident Insurance and New Rural Cooperative Medical Scheme [21].
Daily living ability was measured using the Chinese version of the 10-item Banhel Index[22],which showed satisfactory internal consistency (Cronbach’s α=0.916) and construct validity [23,24].The results presented a total score range of 0-100,with high scores indicating high daily living ability [22].1) ≤20:The activity is discontinued because the person stopped performing or is unable to perform the activity;2) 25-40:The activity is carried out with complete dependence on and continuous help from others;3)45-55:The activity is carried out independently but with occasional help from others and with moderate limitations;4) 60-95:The activity is carried out completely independently without help but with mild limitations;and 5) 100:The activity is carried out completely independently without help and with no limitations.
2.4.Ethical considerations
This study was approved by the Zhejiang Chinese Medical University Human Research Ethics Committee (approval number 2018KY544).Our research group also obtain the written consent of the three long-term care facilities,which agreed that the doctors and nurses provide the patient’s data while the data did not contain identifiable personal information.Prior to the data collection,all participants signed a consent form and were assured of the confidentiality of their responses.
2.5.Data collection
Four postgraduate students received special training before they conducted data collection to make sure they understood the questionnaire’s structure and content,the purpose and significance of the survey,the key points of communicating with the elderly,and how to fill in the questionnaire in a standard way.Data were collected face to face.For the elderly with poor eyesight or who are not comfortable filling in the questionnaires by themselves,the investigators read the answers one by one,then the elderly answered the questions orally,and then the investigators recorded the answers.All the questionnaires were checked on the spot to ensure the accuracy and authenticity of the results.
2.6.Statistical analyses
Statistical analyses were carried out using the IBM SPSS version 22.0.Descriptive statistics were used for the participant characteristics.The total score was the sum of the scores from the 32 examined items.Dimension scores,average scores for each dimension,and item scores were calculated.Furthermore,we analyzed which of the abovementioned characteristics considerably influencing dignity were related to the total score of the Dignity Scale.To analyze all these relationships,we entered 20 variables into the multiple linear regression models with a stepwise selection mode to retain the significant ones in the final regression model.The significance level α was set at 0.05,and all comparisons were two-tailed.
3.Results
3.1.Participant characteristics
No data were missing.The descriptive characteristics of the participants are summarized in Table 1.The sample was mostly composed of women(59.3%)and well advanced in age,specifically 80-89 years (68.8%).Among the participants,over 80% indicated that they once lived in the city and followed no religion.More than 60% were married and attained junior high school or high school education.More than 50%indicated being a professional technician or civil servant as their pre-retirement occupation,having a surplus economic status,and having over two chronic diseases.Approximately 85% indicated that their medical payment method was covered by the UEI,and over 75% were taking medication.Almost 50% stated a reduced ability to perform daily activities.
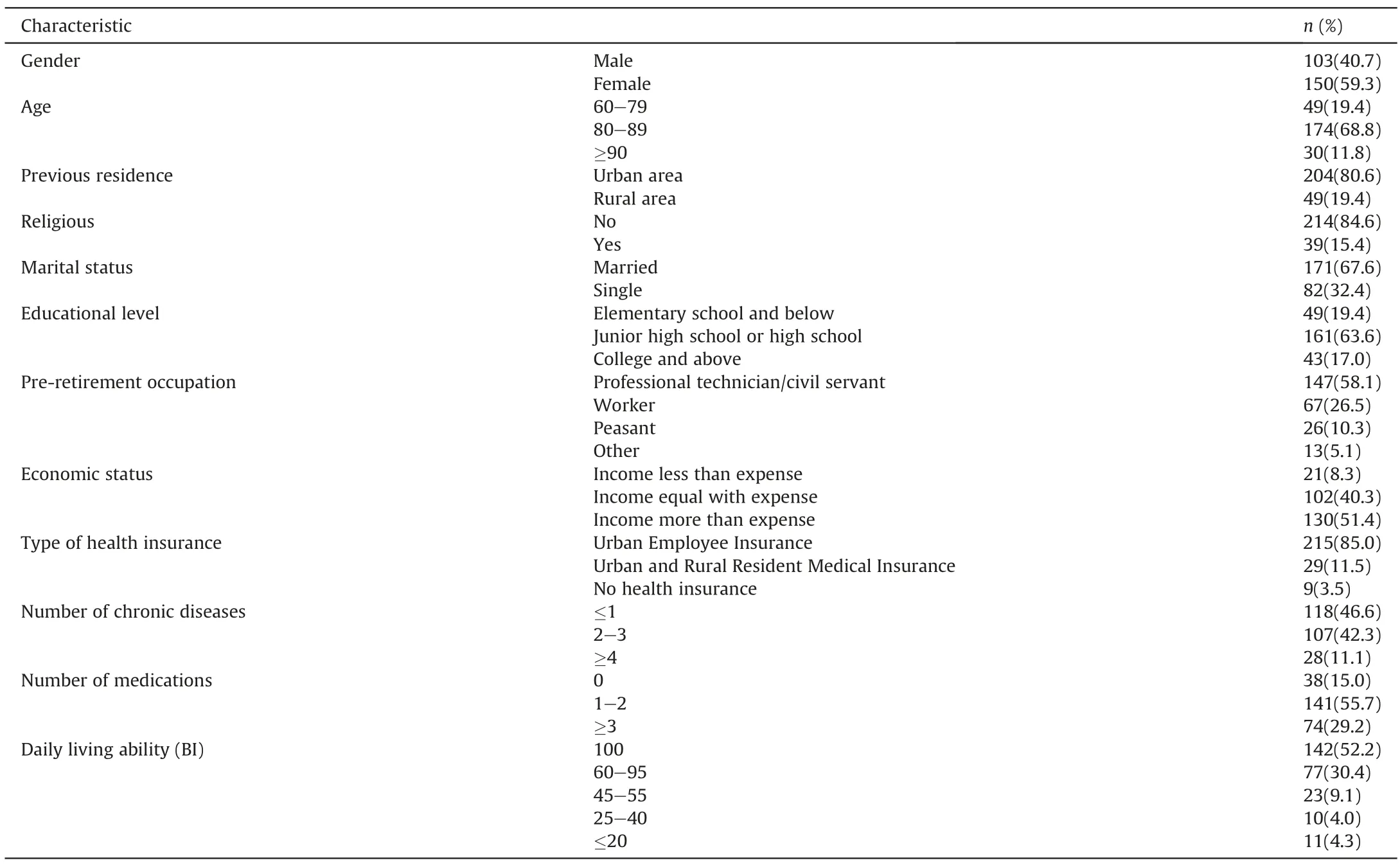
Table 1 Characteristics of the participants (n=253).
3.2.Dignity score of older adults in long-term care facilities
The Dignity Scale total score was 151.95±11.75.The dimension scores are summarized in Table 2.
3.3.Multivariate linear analysis of the dignity score of older adults in long-term care facilities
The final regression model,which was derived from the stepwise multiple linear regression analysis,revealed that five variables,including economic status,numbers of chronic diseases and medications,previous residence and daily living ability,significantly affected the dignity among older adults in long-term care facilities (Table 3).The independent variables,economic status,number of chronic disease,number of medications and daily living ability,are taken as hierarchical variables.Economic status:“Income less than expense”=1;“Income equal with expense”=2;“Income more than expense”=3.The number of chronic disease:“≤1”=1;“2-3”=2;“≥4”=3.The number of medication:“0”=1;“1-2”=2;“≥3”=3.Daily living ability:“100”=1;“60-95”=2;“45-55”=3;“25-40”=4;“≤20”=5.Previous residence is taken as categorical variable:“urban area”=0,“rural area”=1.The final model significantly accounted for 39.2% of the variance of the dignity score (F=23.201,P <0.001).A high score of the Dignity Scale correlated significantly with high economic status,fewer chronic diseases,less medication,better daily living ability,andlong-time lived in cities before.As for the other variables,namely gender,age,religion,marital status,educational level,preretirement occupation,and type of health insurance,the Dignity Scale score did not differ among different groups.
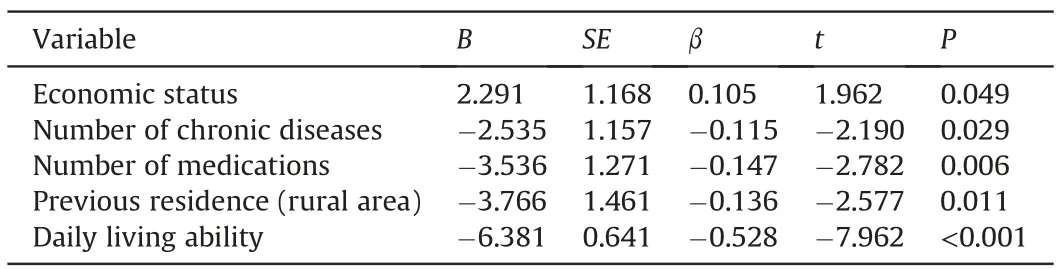
Table 3 Multiple regression of factors associated with dignity of older adults in long-term care facilities (n=253).

Table 2 Total score and dimension score of the Dignity Scale (n=253).
4.Discussion
4.1.Dignity is challenged most by physical and autonomy factors
This study was carried out in a city of China to examine the dignity status and its related factors among older adults in longterm care facilities.Previous studies showed that dignity is challenged most by the threat of illness and autonomy,a finding similar to the present study’s result.Pleschberger [25] explored the meaning of dignity regarding end-of-life issues from the perspective of older nursing home residents through a qualitative study.The results showed that dignity is challenged most by the threat of illness and having care needs.Rodríguez-Prat [26] found that dignity is generally equated with the person’s sense of autonomy and control for patients with advanced disease.Caspari [27] interviewed the residents who were living in nursing homes to study whether they felt that their dignity was maintained,and results showed that the residents emphasized freedom as very important.
4.2.Dignity is associated with disease-related factors
With more chronic diseases,more medications and poorer daily living ability of older adults in long-term care facilities significantly correlated with a low level of dignity,which concurred with the mentioned above statement that physical and autonomy factors influence dignity.More chronic diseases and more medications indicated more inferior physical function,which is closely related to daily living ability [28].Unhealthy physical conditions limited the daily living ability of older adults and led to their high dependence on others.In this study,nearly half of the participants indicated a reduced ability to perform daily living activities.Therefore,to ensure that older adults can live with dignity in long-term care facilities,we should focus on improving their physical function and daily living ability by encouraging them to carry out physical exercises and rehabilitation.
4.3.Dignity is associated with socioeconomic factors
The findings suggested that dignity among older adults dwelling in long-term care facilities is associated with disease-related factors and socioeconomic factors,which refer to economic status and previous residence in this study.However,no significant association was found with age,gender,religion,marital status,educational level,occupation,and type of health insurance.The results of association with economic status concurred with those of a previous study [29].When the material needs became a problem,the spiritual needs were no longer pursued [30].Economic status also influenced physical and psychological conditions [31].Thus,the importance of economic status for older adults and as a factor affecting their dignity was confirmed [32].
Previous studies showed no relation between previous residence and dignity.In China,people who lived in rural areas were more affected by traditional values and attached greater importance to the concept of family than those who lived in cities [33].Older adults in rural areas showed a traditional notion that they will be cared for at home by their children and living in a long-term care facility meant experiencing poor living conditions or having an unfilial family[34].Thus,we hypothesized that this negative notion among older adults who lived in rural areas could considerably affect their dignity.Interestingly,in this study,the previous residence indeed correlated with dignity.Thus,maintaining relationships with families is highly important because of the strong Chinese cultural norms.Caregivers should attach importance to the role of the family in the support system and encourage the offspring to take as much time as possible to visit and communicate with older adults dwelling in long-term care facilities [35].Older adults with more family visits experienced happiness and dignity rather than abandonment [36].
The present findings on age and occupation differed from those from previous studies [29,35,37].A possible explanation for this contradictory finding is that the eligible participants in other studies were young and middle-aged patients.These cohorts are the‘core force’in Chinese society and the‘backbone’of a family.If these individuals are unable to perform their previous jobs,it will place substantial pressures on the family,leading to considerable psychological and financial distress and,accordingly,impaired dignity.The other sociodemographic factors (gender,religion,educational level,marital status,and type of health insurance)demonstrated no relation with dignity.These variables are correlated to dignity in several studies [9,29] but not in others [35,38],possibly due to the variation in evaluation methods,sample size and characteristics.
4.4.Implications for nursing practice
Understanding the dignity of older adults in long-term care facilities and its potentially related factors is of great value for implementing comprehensive geriatric nursing in China.We need to continue maintaining dignity among older adults,especially by improving their autonomous and physical factors.Facilitating dignity from the dimension of autonomous factors requires personcentered care rather than task-or regulation-oriented care to be implemented in long-term care facilities [39].We can provide several choices in many small things so they can regain control and maintain their dignity.To facilitate dignity from the dimension of physical factors among older adults,caregivers should place older adults under a state of physical comfort.Caregivers in long-term care facilities should also tailor the activities to each elderly to enable active participation as well as support and encourage older adults to achieve a goal or action within their power [40].
In terms of the influencing factors on dignity,economic status showed a strong correlation with dignity.Thus,in terms of pension financing,comprehensive measures should be implemented to increase economic security,including old-age and medical security,for older adults,especially those with low income,to reduce the financial burden and thus preserve their dignity.Furthermore,older adults with low economic status,more chronic diseases and more medications,poor daily living ability,or previous residence in rural areas seemed to be most at risk of losing dignity in long-term care facilities and thus require more attention than their peers.The results showed that care for older adults is not simply physical but requires meeting their needs and maintaining their dignity.As for caregivers,busy schedules are an additional problem [41].Thus,more people should be encouraged to join geriatric nursing.
4.5.Limitations
Similar to any other research,this study encountered several limitations.Firstly,this study only carried out convenient sample surveys among older adults dwelling in long-term care facilities in Hangzhou.Thus,the representativeness of the participants and the sample coverage presented certain limitations.Secondly,the factors influencing dignity in this study were not comprehensive and only included sociodemographic and disease-related factors.Thirdly,the regression model showed that only 39.2% of the variables were explained.Finally,the concept of dignity is complex,abstract,and difficult to measure.The self-developed dignity scale used in this study can only detect whether a certain symptom or experience undermines dignity and not what preserves dignity.However,an instrument measuring both undermining and preservative factors would require a different structure and might be too complex to be understood by the respondents.
5.Conclusion
Dignity of older adults in long-term care facilities is challenged most by physical and autonomy factors.This study shed light on the characteristics that predispose older adults dwelling in long-term care facilities to feel that their dignity is undermined.Older adults with low economic status,more chronic diseases and more medications,poor daily living ability,or living in rural areas before dwelling in long-term care facilities seem to be most at risk of losing dignity in long-term care facilities and thus require more attention than their peers.Further studies are needed to verify the reliability and validity of the dignity scale under different cultural contexts,find potentially related factors influencing dignity,and provide quality nursing service to preserve the dignity of older adults in long-term care facilities.
Funding
This work was supported by the Health Commission of Zhejiang Province (Grant number 2018KY544,2018).
CRediT authorship contribution statement
Die Dong:Conceptualization,Methodology,Formal analysis,Investigation,Resources,Data curation,Writing -original draft,Project administration.Qian Cai:Conceptualization,Methodology,Formal analysis,Investigation,Resources,Data curation,Writingoriginal draft,Project administration.Qiong-Zhi Zhang:Conceptualization,Methodology,Formal analysis,Investigation,Resources,Data curation,Writing-original draft,Project administration.Zhi-Nan Zhou:Formal analysis,Investigation,Data curation,Writingoriginal draft.Jia-Ning Dai:Formal analysis,Investigation,Data curation,Writing -original draft.Ting-Yu Mu:Formal analysis,Investigation,Data curation,Writing -original draft.Jia-Yi Xu:Formal analysis,Investigation,Data curation,Writing -original draft.Cui-Zhen Shen:Conceptualization,Methodology,Formal analysis,Investigation,Data curation,Writing -original draft,Writing -review&editing,Funding acquisition.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
We would like to express our gratitude to all participants in long-term care facilities for their good collaboration.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2021.08.003.
杂志排行

International Journal of Nursing Sciences的其它文章
- Second-order problem solving:Nurses’ perspectives on learning from near misses
- Exploring the employment readiness and return to work status of breast cancer patients and related factors
- Resilience of nurses at the epicenter of the COVID-19 pandemic in Lebanon
- A study of the relationship between nurses’ experience,structural empowerment,and attitudes toward computer use
- Mobile health applications for the care of patients with breast cancer:A scoping review
- Nursing students’ attitudes toward mobile learning:An integrative review