Comparative analysis of the clinical outcomes between wavefront-guided and conventional femtosecond LASlK in myopia and myopia astigmatism
2021-11-08XiaoGuiRuiZhangShaLiNaZhaoHaoRuiZhangYuKunZhouChenYangHuanChunYanZhaoHongYingWangHongYuanSongWeiShenJianHuaZhang
Xiao Gui, Rui Zhang, Sha Li, Na Zhao, Hao-Rui Zhang, Yu-Kun Zhou, Chen-Yang Huan,Chun-Yan Zhao, Hong-Ying Wang, Hong-Yuan Song,2, Wei Shen, Jian-Hua Zhang
1Department of Ophthalmology, the First Affiliated Hospital of Naval Medical University, Shanghai 200433, China
2Department of Ophthalmology, Shanghai General Hospital,Shanghai Jiao Tong University School of Medicine, Shanghai 200080, China
Abstract
● KEYWORDS: refractive surgery; high order aberration;visual quality; wavefront-guided femtosecond LASIK
INTRODUCTION
The incidence of myopia increases significantly these years because of the extensive usage of electronic devices and the over-loaded schoolwork[1-3]. Refractive surgery has been one of the major approaches to improve the optical outcomes[4]. Among them, laser-assistedin situkeratomileusis(LASIK), implantable collamer lens (ICL) and small incision lenticule extraction (SMILE) are the most commonly performed operations in recent years[5]. For the LASIK surgery,the femtosecond laser assisted LASIK (FS-LASIK) is known to obtain better clinical outcomes than common LASIK[6-7].
There are two major types of FS-LASIK, knowing as topography-guided FS-LASIK and wavefront-guided (WFG)FS-LASIK, which can modify surgical parameters to get better optical quality[8-10]. Topography-guided FS-LASIK aims to improve corneal irregularities thus maintaining the aspheric shape of the cornea[11]. Recent investigations show that topography-guided FS-LASIK gives promising clinical outcomes in irregular cornea[12]. However, topography-guided FS-LASIK could not improve the high order aberrations(HOAs) effectively[13]. The induction of HOAs often lead to complaints of patients for glare, halo, starbursts and decreased visual sharpness[14]. Ablation algorithm, wound healing, optical role of the flap and reflection losses of the cornea are the major reasons for the induction of HOAs[15]. WFG FS-LASIK is able to improve the induction of spherical aberrationviastrengthening peripheral pulses, which could maintain proper shape of the cornea[16].
Although it is known that WFG FS-LASIK could improve the visual quality of patients than the common FS-LASIK[17]. The effect of high myopia on the induction of HOAs using WFG FS-LASIK is largely not clear. Therefore, we conducted this retrospective study to further clarify the clinical outcomes between WFG FS-LASIK and conventional FS-LASIK(NWFG FS-LASIK) among patients with low & moderate and high myopia.
SUBJECTS AND METHODS
Ethical Approval The present study adhered to the Declaration of Helsinki. The present study was approved by the Ethics Committee of Shanghai Changhai Hospital, Naval Medical University. Meanwhile, informed consent was signed by all subjects before their inclusion in the research.
Patients Two hundred and thirty-six eyes of 122 patients with myopia and myopia astigmatism had been performed FS-LASIK at Shanghai Changhai Hospital from July 2018 to June 2020 were enrolled in this study. The inclusion criteria included that older than 18y, refractive stability for at least 1y and stopping using soft contact lenses for more than 1wk.Exclusion criteria included corneal scar, pregnancy, history of herpetic eye disease, active ocular infection and other inflammatory disorders.
Preoperative Examinations The evaluation of slit-lamp biomicroscopy, manifest refraction, uncorrected distance visual acuity (UDVA), corrected distance visual acuity(CDVA), dilated fundus evaluation, intraocular pressure (IOP),ocular axis length, central corneal thickness (CCT), corneal tomography and corneal aberration were performed.
Surgical Procedures All surgeries were carried out and follow-up was done by two skilled refractive surgeons at Changhai Ophthalmic Refractive Surgery Centre. Patient follow-up examinations were completed in the same center.The surgery was performed under topical anesthesia. The iFS femtosecond laser system was used to create corneal flap with the thickness of 100 μm. The diameter of the flap ranged from 8.0 to 8.5 mm with superior-hinged flap. After flap lifting, the VISX S4IR excimer laser system was used for the laser ablation,assuming a refractive target of emmetropia. Then the flap was repositioned, and the interface was washed using the balanced saline buffer.
WFG LASIK surgeries calculated according to the newgeneration aberrometer measurement (iDesign Advanced WaveScan). All surgeries were operated with the optical zone of 6-7 mm and the ablation zone of 8-9 mm according to patients’ pupil size, refraction, and corneal depth, with transition zone of 1 mm. During the laser ablation period,iris registration and eye tracker were activated automatically.Conventional LASIK surgeries were operated in all cases with 6 mm optical zone and total ablation zone of 8 mm. The transition zone was 1 mm. During the laser ablation period, the eye tracker was activated automatically.
Postoperative Care and Follow-Up In both groups, standard topical postoperative treatment consist of a combination of 0.1% dexamethasone and 0.3% ofloxacin eye drops, which were instilled 4 times a day for a week. Dexamethasone tapering the frequency for 3 additional weeks (3 times, then 2 times, and finally once a day). Also, patients were asked to use artificial tear solution 6 times a day during 2mo. Patients made appointment of further consultation at 1d, 1wk, 1, 3, 6mo, 1,and 2y.
Statistical Analysis Data were analyzed using GraphPad Prism 9.0 (GraphPad Software, San Diego, CA, USA).Kolmogorov-Smirnov test was used to assess the normality of distribution of data. Unpairedt-test was used to compare normally distributed data and the data were represented as mean±standard error of mean (SEM). Non-normally distributed data was analyzed using Mann-Whitney test, and the data were represented as median. AP-value was considered statistically significant when it was lower than 0.05.
RESULTS
Table 1 presents the preoperative demographics of the eyes.Total 97 eyes of 50 patients (23 males and 27 females) were performed WFG FS-LASIK. Total 139 eyes of 72 patients (29 males and 43 females) were performed NWFG FS-LASIK.The mean age of WFG group was 23.44±5.41y and the mean age of NWFG group was 25.49±5.85y. There is no significant difference of ages between WFG group and NWFG group(P=0.058). The mean CCT of WFG group was 537.8±20.67 μm,and the median CCT of NWFG group was 538.7±31.65 μm.There is no apparent difference of CCT between WFG group and NWFG group (P=0.82). IOP of WFG group was 15.68±3.07 mm Hg, and NWFG group was 15.38±3.13 mm Hg.There is no significant difference of IOP between WFG group and NWFG group (P=0.48). The preoperative sphere of WFG group was -4.83±1.86 D, and NWFG group was -5.32±2.25 D.There is no significant difference of preoperative sphere between WFG group and NWFG group (P=0.08). The preoperative cylinder of WFG group was -1.18±1.23 D, and NWFG group was -0.72±0.67 D. There is significant difference of preoperative cylinder between WFG group and NWFG group (P<0.05).
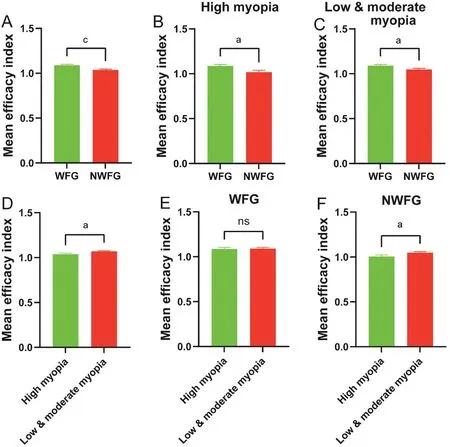
Figure 1 Changes in MEI after WFG and NWFG FS-LASIK A: WFG group showed better MEI than NWFG group; B: WFG group showed better MEI than NWFG group in patients with high myopia; C: WFG group showed better MEI than NWFG group in patients with low& moderate myopia; D: High myopia group showed worse MEI than low & moderate myopia group; E: WFG FS-LASIK led to same MEI in myopia group and low & moderate myopia group; F: Low & moderate myopia group showed better MEI than high myopia group in patients using NWFG surgery. Means±SEM (aP<0.05, bP<0.01, cP<0.001, dP<0.0001, ns: None).
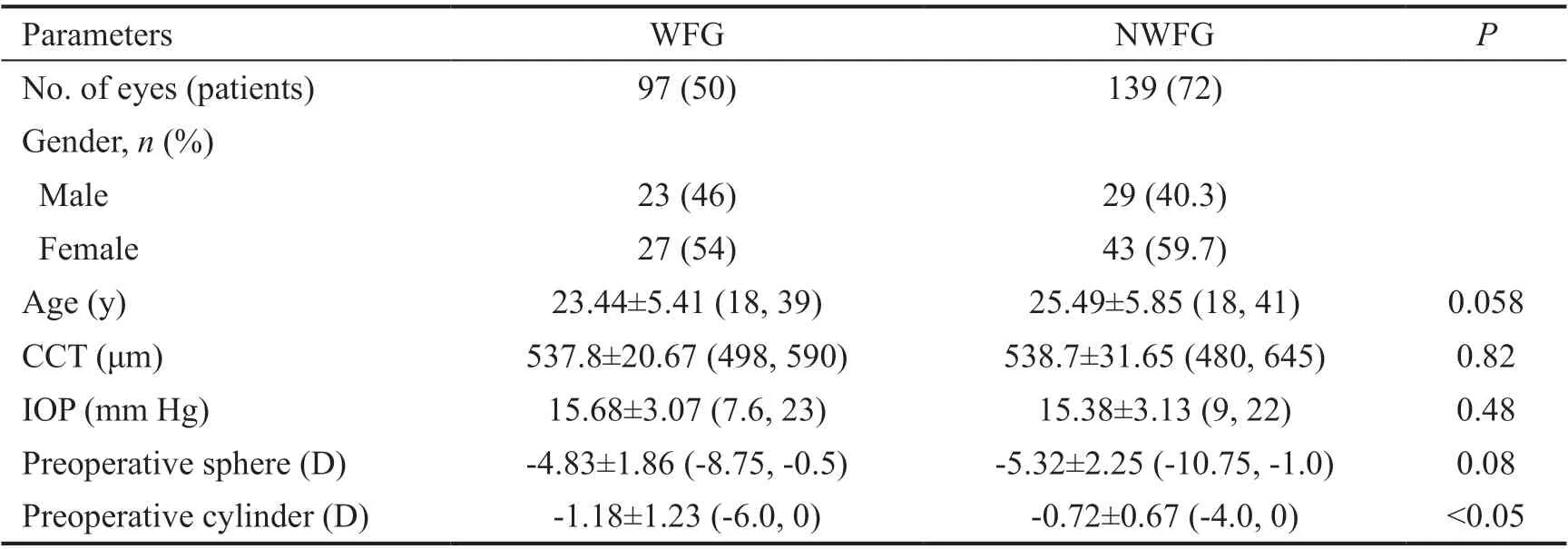
Table 1 Preoperative demographics mean±SD, range
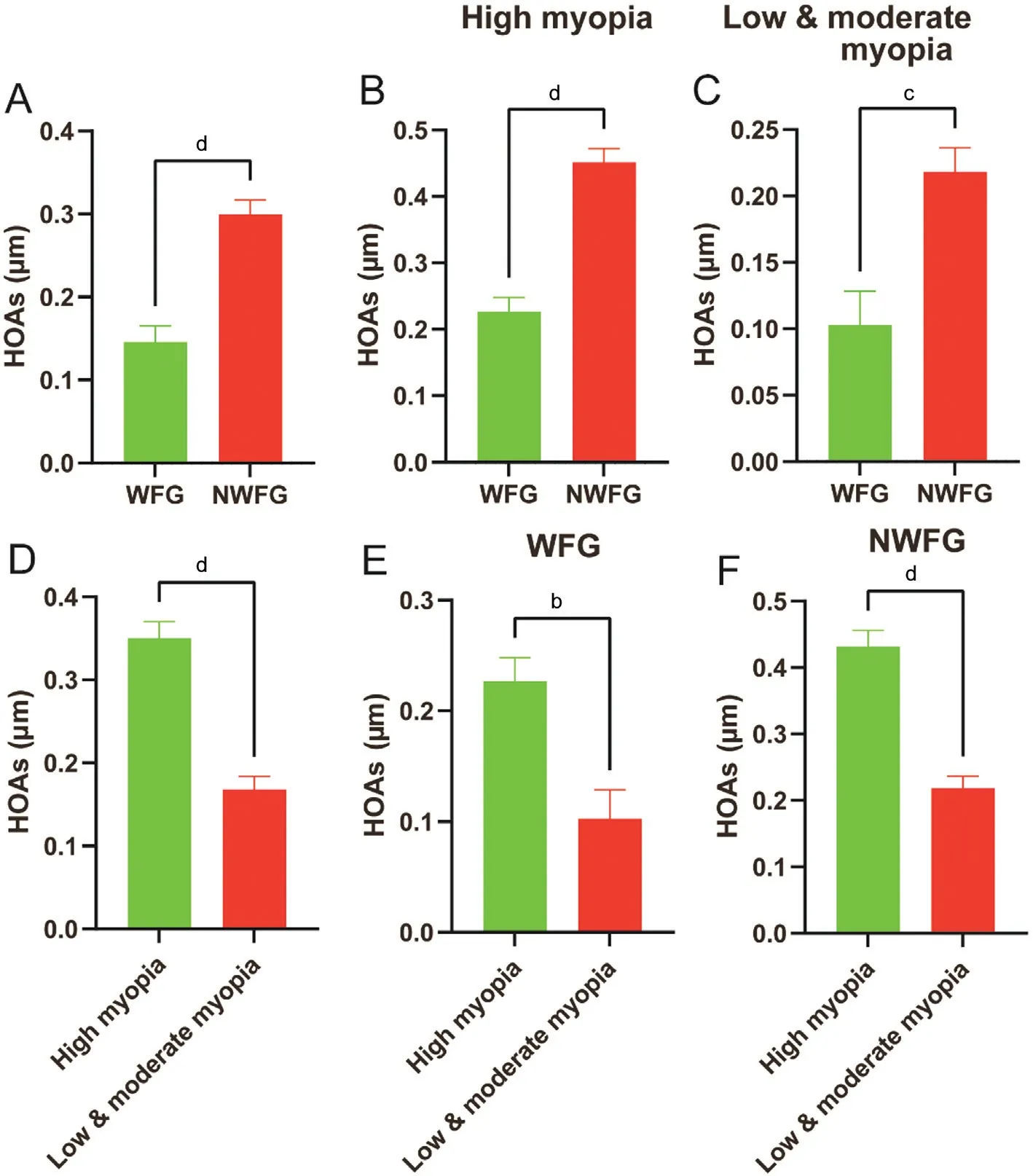
Figure 2 Changes in HOAs after WFG and NWFG FS-LASIK A: WFG group showed lower HOAs than NWFG group; B: WFG group showed lower HOAs than NWFG group in patients with high myopia; C: WFG group showed lower HOAs than NWFG group in low &moderate myopia group; D: Higher HOAs were observed in patients with high myopia; E: High myopia group showed worse HOAs in patients using WFG surgery. F: High myopia group showed worse HOAs in patients using NWFG surgery. Means±SEM (aP<0.05, bP<0.01, cP<0.001,dP<0.0001, ns: None).
Mean Efficacy Index The ratio between postoperative UDVA and preoperative CDVA assessed using Snellen decimal was known as efficacy index[18]. The mean efficacy index (MEI)can be an efficient indicator to evaluate the change of distance visual acuity. There was no difference between WFG group(-0.054±0.049) and NWFG group (-0.040±0.056) in UDVA after surgery. The data showed that the MEI of WFG group was 1.090±0.106 and the MEI of NWFG was 1.036±0.124(Figure 1A). The MEI of both groups was higher than 1,indicating that these two surgical methods were effective and safe procedures. WFG group had higher MEI than NWFG group (P<0.001). Meanwhile, we assessed the MEI of WFG and NWFG in high myopia group and low & moderate myopia group separately. The MEI of WFG in high myopia group was 1.086±0.103, and MEI of NWFG in high myopia group was 1.018±0.147 (Figure 1B). The MEI of WFG in low &moderate myopia group was 1.091±0.109, and MEI of NWFG in low & moderate myopia group was 1.048±0.108 (Figure 1C). Furthermore, we evaluated the differences of MEI in high myopia group and low & moderate myopia group. The data indicated that the MEI of high myopia group was 1.037±0.117 and the MEI of low & moderate myopia was 1.068±0.109(Figure 1D). Patients with low & moderate myopia showed better MEI than patients with high myopia (P<0.05). However,there was no difference between high myopia group and low& moderate myopia group using WFG methods (Figure 1E).Patients underwent NWFG surgery showed better MEI in low& moderate myopia group than that in high myopia group(Figure 1F).
High Order Aberrations The data showed that the HOAs of WFG group was 0.146±0.188 and the HOAs of NWFG was 0.300±0.196 (Figure 2A). NWFG group had higher HOAs than WFG group (P<0.001). Meanwhile, we assessed the HOAs of WFG and NWFG with high myopia and low & moderate myopia. The HOAs of WFG combined with high myopia group was 0.227±0.123, and HOAs of NWFG combined with high myopia group was 0.451±0.146 (Figure 2B). The HOAs of WFG combined with low & moderate myopia group was 0.103±0.203, and HOAs of NWFG combined with low& moderate myopia group was 0.218±0.163 (Figure 2C).Furthermore, we evaluated the differences of HOAs between patients with high myopia and low & moderate myopia.The data showed that the HOAs of high myopia group was 0.350±0.185 and the HOAs of low & moderate myopia was 0.168±0.190 (Figure 2D). Patients with low & moderate myopia showed better HOAs than patients with high myopia(P<0.001). Patients underwent WFG or NWFG surgery showed better HOAs in low & moderate myopia group.
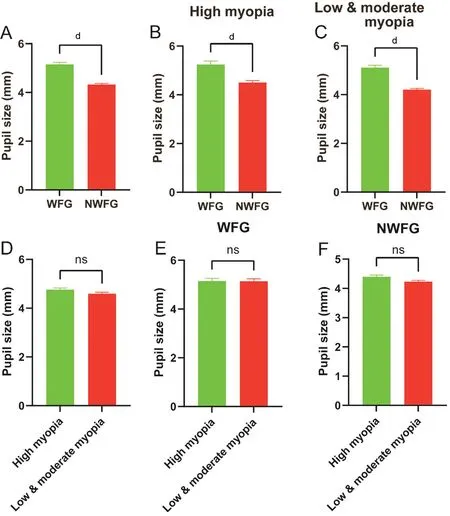
Figure 3 Pupil size in WFG and NWFG FS-LASIK A: Patients performed WFG FS-LASIK had larger pupil size; B: WFG group had larger pupil size in patients with high myopia; C: WFG group showed larger pupil size in patients with low & moderate myopia; D: Patients with high myopia and patients with low & moderate myopia had equal size of pupil; E: Patients with high myopia and patients with low & moderate myopia had equal pupil size in WFG group. F: Patients with high myopia and patients with low & moderate myopia had equal pupil size in NWFG group. Means±SEM (aP<0.05, bP<0.01, cP<0.001, dP<0.0001, ns: None).
Pupil Size The data showed that the pupil size of WFG group was 5.15±0.76 mm and the pupil size of NWFG was 4.32±0.52 mm(Figure 3A). Patients in NWFG group had larger pupil size than that in NWFG group (P<0.001). Meanwhile, we assessed the pupil size of WFG and NWFG with high myopia and low& moderate myopia. The pupil size of WFG in patients with high myopia was 5.25±0.74 mm, and pupil size of NWFG in patients with high myopia was 4.51±0.55 mm (Figure 3B). The pupil size of WFG in patients with low & moderate myopia was 5.11±0.77 mm, and pupil size of NWFG in patients with low & moderate myopia was 4.20±0.46 mm (Figure 3C). Furthermore, we evaluated the differences of pupil size between high and low & moderate myopia group. The pupil size in high myopia group and low & moderate myopia group showed no significant difference (Figure 3D-3F).
Patient Satisfaction A total of 116 patients finally completed the subjective questionnaire assessing the satisfaction of surgery and the quality of vision. Both surgical groups were satisfied with the operations, and there was no difference between WFG (9.33) and NWFG (9.253) group in satisfaction questionnaire (Figure 4A). For the quality of vision, the data showed that WFG group (1.59) had better visual quality than that in NWFG group (2.78, Figure 4B). Patients with high myopia (9.06) got lower satisfaction scores than patients with low & moderate myopia (9.42, Figure 4C). Meanwhile,the data indicated that patients in high myopia group (3.73)had worse visual quality than patients with low & moderate myopia (1.33, Figure 4D).
DISCUSSION
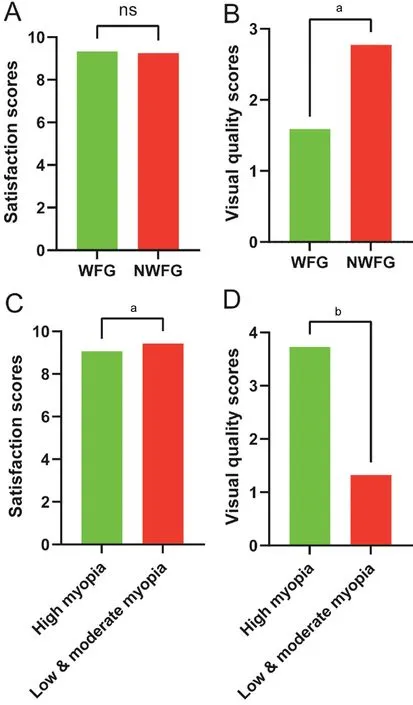
Figure 4 Patients satisfaction after WFG and NWFG FSLASIK A: The patients in WFG and NWFG group were satisfied with refractive surgery; B: WFG group showed better visual quality than NWFG group; C: Patients with high myopia showed worse satisfaction than patients with low & moderate myopia; D: Visual quality in patients with high myopia was worse than patients with low & moderate myopia. Means±SEM (aP<0.05, bP<0.01, cP<0.001,dP<0.0001, ns: None).
In the current investigation, we revealed that both WFG FSLASIK and NWFG FS-LASIK were safe and efficient for the treatment of myopia. Compared with NWFG group, the data of WFG group showed better MEI, HOAs and visual quality.Meanwhile, the investigation indicated that high myopia would result in worse MEI, HOAs and visual quality compared with low & moderate myopia.
The preoperative demographics of the eyes showed that there was no apparent difference in age, CCT, IOP and preoperative sphere between these two groups. However, preoperative cylinder in patients performed WFG FS-LASIK was greater than patients performed NWFG FS-LASIK. This was consistent with surgeon’s preoperative decision as WFG FSLASIK was better in correction of myopia astigmatism[19].Meanwhile, our data also showed that the pupil size was much larger in WFG group than that in NWFG group. It is known that larger pupil size was correlated with worse clinical outcomes, especially night visual symptoms including decreased UDVA, glare, starbursts and haloes[20-22]. Using a new generation aberrometer, WFG FS-LASIK was able to modify the surgical parameters, thus performing specialized refractive surgery with larger optical zone and ablation zone.The results of this study suggested that WFG FS-LASIK was much better than conventional FS-LASIK, as the MEI, HOAs,correction of myopia astigmatism and visual quality of WFG group were better than that in NWFG group even with higher preoperative cylinder and larger pupil size in WFG group.
Myopia astigmatism results from increased cylinder is one of the major factors that affects visual quality[23]. It is reported that the eye ball will rotate up to 15 degree when the patients turn to supine position from sitting position[24].During the process of WFG FS-LASIK, iris registration and eye tracker are activated which give to better correction of myopia astigmatism. In our study, the patients with higher myopia astigmatism were assigned to WFG group and the data confirmed that the cylinder was much higher in WFG group than that in NWFG group. Even though patients in WFG group had worse preoperative refractive conditions, they had better postoperative results. These data suggested that WFG FS-LASIK possessed good power in correction of myopia astigmatism.
The ratio between postoperative UDVA and preoperative CDVA assessed using Snellen decimal was known as efficacy index[7]. Therefore, the MEI can be a good index to assess the efficiency and safety of refractive surgery. The MEI of WFG group, NWFG group, high myopia group and low &moderate myopia group were all greater than 1, indicating that both WFG and NWFG LASIK were good surgical methods in correction of high and low & moderate myopia. Patients in WFG group had better MEI than in NWFG group, indicating that WFG FS-LASIK was more reliable in correction of myopia. Patients in high myopia group got worse MEI than patients in low & moderate myopia, suggesting the importance of preventing the progression of myopia.
HOAs including spherical aberrations, trefoil and coma, are minor optical irregularities of the ocular refractive media[25].They are existed before operation and induced during refractive surgery, and cannot be corrected with glasses or contact lenses[26]. Plenty of studies have proved that HOAs are responsible for the decrease of visual quality[27-29]. Our results showed that the correction of HOAs in WFG group using an iDesign aberrometer was much better than that in NWFG group. Meanwhile, the induction of HOAs in patients with high myopia was much higher than patients with low &moderate myopia. It is reported that the induction of HOAs was higher in high myopia group than that in moderate myopia using SMILE method[30]. Our data further confirmed that the induction of HOAs in high myopia cannot decrease using any refractive surgery. There are also studies showing that HOAs alone cannot provide sufficient image quality[26,31-32]. Here, we combined HOAs with MEI and optical quality questionnaire to assess the superiority of WFG FS-LASIK. The data showed that WFG group had better MEI, HOAs and visual quality than that in NWFG group. Meanwhile, the results showed that high myopia group had worse MEI, HOAs and visual quality than that in low & moderate group.
In conclusion, this investigation indicated that using iDesign aberrometer to perform WFG FS-LASIK could improve the induction of HOAs, which gave better distance vision acuity and visual quality than conventional FS-LASIK. No matter in high myopia group or low & moderate myopia group, WFG FS-LASIK showed better clinical outcomes than conventional FS-LASIK. The data suggested that WFG FS-LASIK was a better choice for patients with myopia when their biological parameters meet the criteria. Since high myopia would lead to worse clinical outcomes in either group, the prevention of high myopia is of vital importance for patients to get better visual quality.
Being a retrospective study, there is some limitations of the present study: 1) This is not a contralateral eye study, therefore we cannot collect the data of biomechanics and healing index.2) There is no comparation of clinical outcomes of each patient in time course, herein we do not know the specific change of ocular parameters at different time.
ACKNOWLEDGEMENTS
Foundations:Supported by National Natural Science Foundation of China (No.81800624; No.81700839;No.82171081); the “Chen Guang” Project Supported by the Shanghai Municipal Education Commission and the Shanghai Education Development Foundation (No.18CG40);234 Mountain Climbing Plan of Changhai Hospital(No.2020YXK048; No.2020YXK058); “Sailing Project”Supported by Naval Medical University.
Conflicts of Interest:Gui X, None; Zhang R, None; Li S,None; Zhao N, None; Zhang HR, None; Zhou YK, None;Huan CY, None; Zhao CY, None; Wang HY, None; Song HY, None; Shen W, None; Zhang JH, None.
杂志排行
International Journal of Ophthalmology的其它文章
- lmpact of intraocular pressure fluctuations on progression of normal tension glaucoma
- Effective treatment for secondary angle-closure glaucoma caused by traumatic lens subluxation:phacoemulsification with capsular-tension-ring implantation combined with ophthalmic endoscopecontrolled goniosynechialysis
- Efficacy and safety of newly developed preservativefree latanoprost 0.005% eye drops versus preserved latanoprost 0.005% in open angle glaucoma and ocular hypertension: 12-week results of a randomized,multicenter, controlled phase III trial
- Progressive restrictive strabismus in an infant
- Association of peripheral anterior synechia, intraocular pressure, and glaucomatous optic neuropathy in primary angle-closure diseases
- Protective effect of LIF-huMSCs on the retina of diabetic model rats