Quality of life after colorectal surgery:A prospective study of patients compared with their spouses
2021-10-09AylazCihangirAkyolAkratKocaayDeryakmenAyBurcuYavuzarslanAyhanlentErkekMehmetAyhanKuzu
Gökçe Aylaz,Cihangir Akyol,Akın Fırat Kocaay,Derya Gökmen,Ayşe Burcu Yavuzarslan,Ayhan Bülent Erkek,Mehmet Ayhan Kuzu
Gökçe Aylaz,Department of Surgery,Sisli Memorial Hospital,Istanbul 34385,Turkey
Cihangir Akyol,Akın Fırat Kocaay,Ayşe Burcu Yavuzarslan,Ayhan Bülent Erkek,Mehmet Ayhan Kuzu,Department of Surgery,Ankara University School of Medicine,Ankara 06100,Turkey
Derya Gökmen,Department of Biostatistics,Ankara University School of Medicine,Ankara 06100,Turkey
Abstract BACKGROUND Although radical surgery for colorectal cancer improves the oncological outcomes,a significant portion of patients suffer from alterations in their quality of life(QoL).There are many studies investigating the QoL of patients who have colorectal cancer but none of these focus on the QoL of spouses.AIM To compare the QoL of patients after colorectal surgery to the QoL of spouses.METHODS This prospective study consisted of patients who were married and who underwent surgery at the University of Ankara,Department of Surgery between March 2006 and November 2010.Patients’ spouses were also enrolled.The study was approved by the Ethics Committee of the Faculty of Medicine,Ankara University,and all patients provided written informed consent.The study included patients who underwent curative surgery for colorectal carcinoma [n =100;abdominoperineal excision (n = 33),low anterior resection (n = 33),left hemicolectomy (n = 34)] and their spouses (n = 100).The patients and spouses completed the Medical Outcome Study 36-item Short Form Survey (SF-36) and the World Health Organization Disability Assessment Schedule II (WHODAS-II)preoperatively and at postoperative months 15 to 18.RESULTS During this 4.5-year study period,273 patients with sigmoid or rectal cancer were admitted to the hospital.Of these patients,119 were eligible and willing to participate.Eleven patients had either systemic or locally inoperable disease,three patients had a severe surgical complication,and five patients were lost to followup.Therefore,a total of 100 patients completed the follow-up period.There was a statistically significant positive correlation between the disability scores of patients and the scores of their spouses for some of the WHODAS-II subscales,such as “self-care,” “life activities,” and “participation in society,” as well as for the total WHODAS-II score.There was also a positive correlation between the QoL of patients and the QoL of their spouses in most of the SF-36 subscales.Statistically significant correlations were observed for the “bodily pain,” “general health,” ”vitality,” “social function,” “emotion,” “mental health,” and mental component summary score subscales of the SF-36.When gender differences were evaluated,the QoL of male patients’ spouses changed more when compared with female patients’ spouses for all of the WHODAS-II subscales.Colorectal cancer surgery has a significant effect on the QoL of both patients and their spouses,these effects were more significant among male patients’ spouses.CONCLUSION Preoperative counseling regarding potential problems should therefore collectively address patient and their spouse as a couple rather than the patient alone,particularly for patients undergoing low anterior resection and abdominoperineal resection procedures.
Key Words:Quality of life;Colorectal surgery;Patients' spouses;Prospective study;Male spouses;Preoperative counseling
INTRODUCTION
There is no doubt that radical colorectal surgery improves the oncological outcomes of patients with cancer.However,the literature has clearly documented that social,physical,sexual,and psychological aspects of life,as well as religious worship,are severely impaired after this treatment[1-5].A significant portion of patients suffer from alterations in their quality of life (QoL),particularly after surgery on distal rectal tumors.Patients who require a stoma or who have low anterior resection (LAR)syndrome may face difficulty adapting to their new anatomy,managing the stoma,defecating,and continuing normal activities in their sociocultural environment.Patients pay an immense price following both sphincter-saving and sphinctersacrificing surgery.Moreover,these psychological and social difficulties,as well as sexual dysfunction,may affect patients’ relationships with their spouses,who are generally the primary informal caregivers for patients with cancer.In addition to caring for their sick partners,the spouses also have to deal with their own anxiety,fatigue,and depression.Previous studies on patients with breast and prostate cancer have also revealed such changes in spouses’ QoL7[6-8].Therefore,both patients’ and spouses’ QoL should be taken into consideration following surgery for colorectal cancer.
Although there are many studies investigating the QoL of patients who have colorectal cancer[1-5,9] none of these focus on the QoL of spouses.Therefore,we hypothesized that radical rectal cancer surgery affects not only patients’ physical,social,and psychological wellbeing but also the QoL of their spouses.The aim of this prospective comparative study was to investigate the QoL of patients and their spouses.To the best of our knowledge,this is the first prospective comparative study to investigate QoL following colorectal cancer surgery in both patients and their spouses during the same time frame.
MATERIALS AND METHODS
Participant selection
This prospective study consisted of patients who were married and who underwent surgery at the University of Ankara,Department of Surgery between March 2006 and November 2010.Patients’ spouses were also enrolled.The study was approved by the Ethics Committee of the Faculty of Medicine,Ankara University,and all patients provided written informed consent.
Inclusion criteria
Patient demographics,surgical details,follow-up data,and disease-related data were recorded.To be eligible,patients had to meet the following inclusion criteria:(1)Curative surgery for colorectal adenocarcinoma;(2) Living with a spouse;(3) No other primary malignant tumors;(4) No additional complicating or disabling disease that necessitated nursing assistance (e.g.,mental illness);(5) No chemo-radiotherapy within 8 wk prior to the interview;(6) No admittance to a hospital except for stoma closure during the study period (no interview during stoma closure);(7) No major morbidity (e.g.,anastomotic leakage,abdominal sepsis,stoma-related problems,and intensive care unit transfer);(8) No evidence of disease recurrence or metastasis,which was determined at the time of follow-up interviews;(9) Aged over 18 years;and (10)Muslim faith.
Groups
Patients and their spouses were grouped by the type of surgery they received:Abdominoperineal resection (APR),sphincter-saving resection with an anastomosis within 6 cm of the anal verge on rigid sigmoidoscopy (LAR),or anterior resection with anastomosis at or above 7 cm,including sigmoid colectomy (AR).
Scales and questionnaires
Medical outcomes (36-item short form health survey):The 36-item short form health survey (SF-36) was used as a measure of health-related QoL because it is an internationally recognized global measure[4,10].It comprises 36 items that measure perceived health on eight scales (i.e.,physical functioning,physical role,bodily pain,general health,vitality,social functioning,emotional role,and mental health) with higher scores (range 0-100) reflecting better perceived health.Additionally,two summary scores can be obtained:The physical component summary score (PCS) and the mental component summary score (MCS).In addition,this tool has been validated in Turkish patients with chronic illnesses,with an internal consistency of 0.92 and a test-retest reliability of 0.94,which are consistent with published work[11].Higher SF-36 scores indicate better health-related QoL.
The World Health Organization disability assessment schedule II
The World Health Organization disability assessment schedule II (WHODAS-II) is an instrument developed by the World Health Organization to assess behavioral limitations and restrictions regarding participation in specific activity domains experienced by an individual independent of their medical diagnosis.The conceptual frame of reference of this instrument is the International Classification of Functioning,Disability,and Health (ICF).Specifically,the instrument is a 36-item,generic,multidimensional questionnaire designed to evaluate the functioning of the individual in six activity domains (i.e.,understanding and communicating,getting around,self-care,getting along with people,life activities,and participation in society)[5].This questionnaire has been validated in Turkish patients with chronic illnesses,with an internal consistency of 0.92 and a test–retest reliability of 0.94,which are consistent with published work[6,7].A higher WHODAS-II score reflects a higher level of disability.
Ankara university life standards questionnaire
To identify how surgery affected the life standards of patients and their spouses,a questionnaire was designed by the Department of Public Health,General Surgery and Psychology,Ankara University (Life Standards Questionnaire)[12,13].It covers the following areas:(1) Employment,including changes in work capability and changes in household chores in daily practice for unemployed women;(2) Social activity;(3)Colostomy care (if applicable);and (4) Religious worship.Religious worship in Muslims was emphasized because their belief structure is particularly affected by the presence of both a stoma and fecal incontinence[13].
Counseling
Surgical details,possible complications,and temporary or permanent stoma formation were explained preoperatively by the surgeon,and ostomy education was given by the stomatherapist.Religious education and counseling were also performed.Patients had direct access to doctors,the stomatherapist,appliance suppliers,and a religious leader(Imam) at the hospital during the study period.
Interviews
Patients and spouses were interviewed at the Department of Surgery of Ibni Sina Hospital.The coauthors of the study were trained to administer the questionnaires in a standard fashion and practiced by using the questionnaires on healthy volunteers before the study began.Patients and spouses were interviewed in a private room by a person of the same gender.The same interviewer was used in the preoperative and postoperative period for each patient and spouse,but the interviewer was not blinded to the type of surgery that the patient had undergone.Patients were first asked to complete a demographic questionnaire designed to determine their age,gender,marital status,educational level,income level,and preoperative employment.The SF-36,WHODAS-II,and Ankara University Life Standards Questionnaire were administered together and consisted of a total of 92 items,which took approximately 35 min to 45 min to complete.Both patients and spouses completed the SF-36,WHODAS-II,and Ankara University Life Standards Questionnaire preoperatively and at postoperative months 15 to 18.
Statistical analysis
Statistical analyses were performed with SPSS for Windows 11.5 (SPSS Inc.,Chicago,IL,United States).Descriptive statistics were given as the mean ± SD [median(minimum-maximum)] for metric variables and frequency (percent) for categorical variables.Data from the questionnaires are expressed as the percent change[(postoperative months 15 to 18 – preoperative)/preoperative × 100].To compare two(or more than two) independent groups in terms of metric variables,the Mann-WhitneyUtest (or Kruskal-Wallis analysis of variance) was used.When the Kruskal-Wallis test revealed a significant difference between the groups,a multiple comparison test was used to determine which groups differed from each other.Bonferroni correction was used for multiple testing.The Wilcoxon signed-rank test was used to evaluate within-group differences between ordinal variables.For categorical variables,independent groups were compared with the chi-squared test,and dependent groups were evaluated using the McNemar test.The degree of association between ordinal variables was evaluated by Spearman’s correlation coefficient.APvalue of <0.05 was considered statistically significant.
RESULTS
During this 4.5-year study period,273 patients with sigmoid or rectal cancer were admitted to the hospital.Of these patients,119 were eligible and willing to participate.Eleven patients had either systemic or locally inoperable disease,three patients had a severe surgical complication,and five patients were lost to follow-up.Therefore,a total of 100 patients completed the follow-up period.The sociodemographic features of patients and their spouses are shown in Table 1.Correlation of the percentagechange in quality of life scores between patients and their spouses are shown in Table 2.The surgery groups were comparable with respect to age,gender,preoperative employment status,tumor–node–metastasis stage,and length of postoperative follow-up.
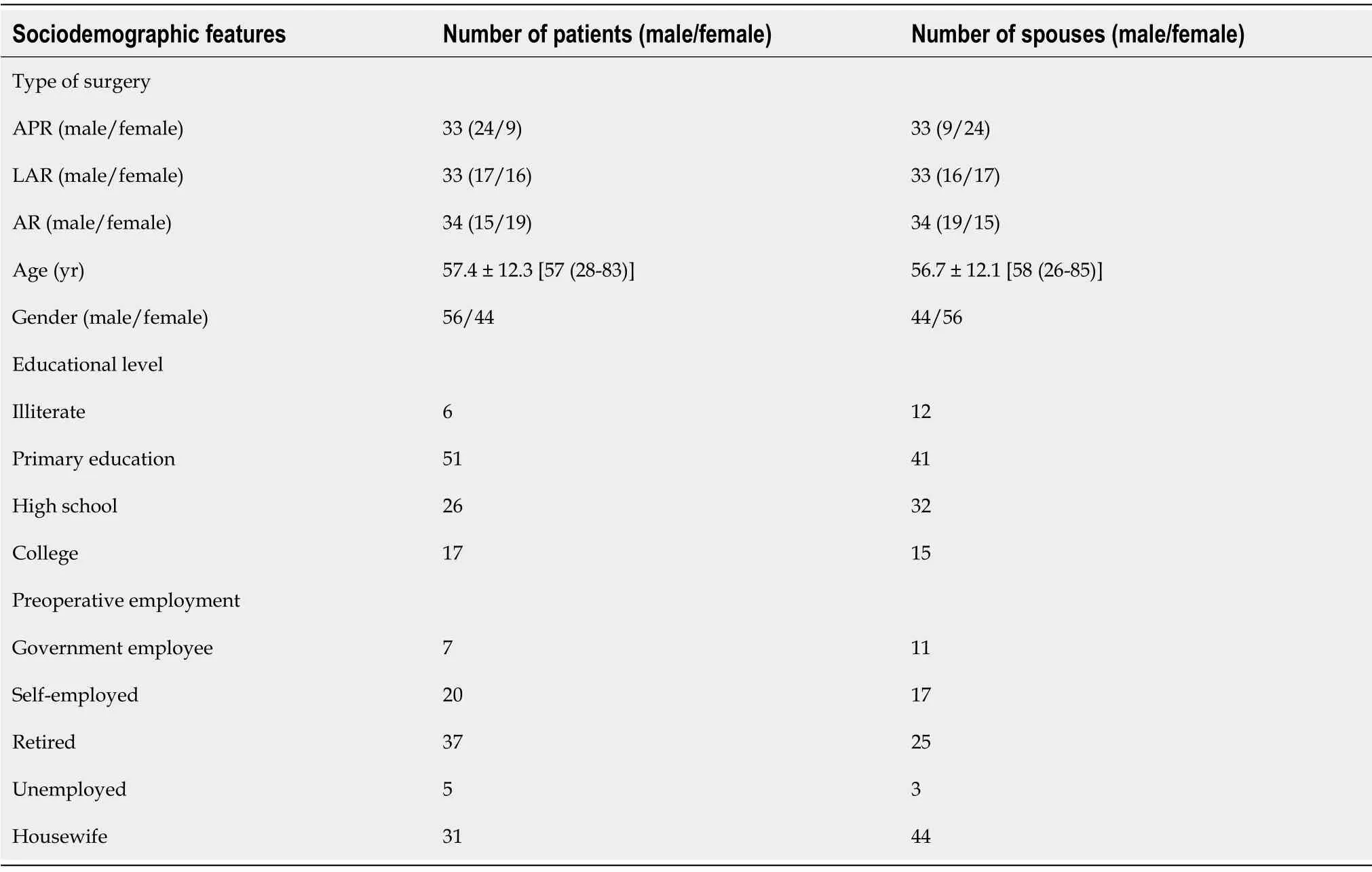
Table 1 Sociodemographic features of patients and their spouses (n = 100)

Table 2 Correlation of the percentage change in quality of life scores between patients and their spouses
For all the subscales of the WHODAS-II,there was an increase in postoperative disability across all surgery types.This increase in disability was minimal in patients who underwent AR compared with patients who underwent LAR or APR:The LAR group had a significantly greater increase in disability scores for the “getting around”and “life activities” subscales,whereas the AR group had significantly less change in disability scores for the “getting along with people” and “participation in society”subscales and the WHODAS-II total score compared with the other two groups.Similar changes were found for the disability levels of patients’ spouses.The “life activities” and WHODAS-II total scores were the least changed in the AR group,whereas the increase in disability level for the “participation in society” subscale was highest in the LAR group (Table 3).

Table 3 Comparison of quality of life changes in patients and their spouses according to type of surgery
In all the subscales of the SF-36,there was a decrease in the QoL of patients with all surgery types from the preoperative to postoperative period.However,the change in patients’ SF-36 scores was significantly lower in the AR group than in the LAR and APR groups.The most significant decrease in QoL scores was detected in the LAR group.Changes in spousal SF-36 scores echoed patients’ scores (i.e.,they were significantly less changed in the LAR group than in the other groups for the “vitality,”“social function,” “emotional role,” “mental health,” “PCS,” and “MCS” subscales)(Table 3).
Comparison of the disability and QoL changes in patients and their spouses by gender
There were increases in the postoperative disability level for all subscales of the WHODAS-II in both genders,but these increases were not statistically significant,except for the “life activities” subscale,which showed a significant increase in female patients and male patients’ spouses compared with males,and the “participation in society” subscale,which showed a significant increase in female patients’ spouses (Table 4).

Table 4 Comparison of the changes in patients’ and spouses’ quality of life according to gender
There was a decrease in QoL scores between the preoperative and postoperative measurements for both genders as assessed by the subscales of the SF-36.Although these decreases tended to be greater in female patients,they were not significantly different when compared with the decreases observed among male patients.Regarding the spouses’ QoL,similar changes were found in both genders (Table 4).
When the data were analyzed with respect to gender and type of surgery,no significant difference was detected in most of the WHODAS-II and SF-36 scores,with the exception of disability level,which showed higher scores on the “life activities”subscale for the female LAR patient group and on the “understanding and communicating” subscale for the female LAR patients’ spouses group.
Ankara university life standards questionnaire
A comparison of patients’ and spouses’ feelings regarding their own general health and their QoL preoperatively and 18 mo postoperatively revealed significant decreases in self-rated health and QoL following surgery (P<0.001).This negative effect was observed across all types of surgery,but the most significant decrease was found in the LAR group when compared with the AR group (Table 5).However,there were no gender differences in either the patient group or spouse group for these measures(data not shown).
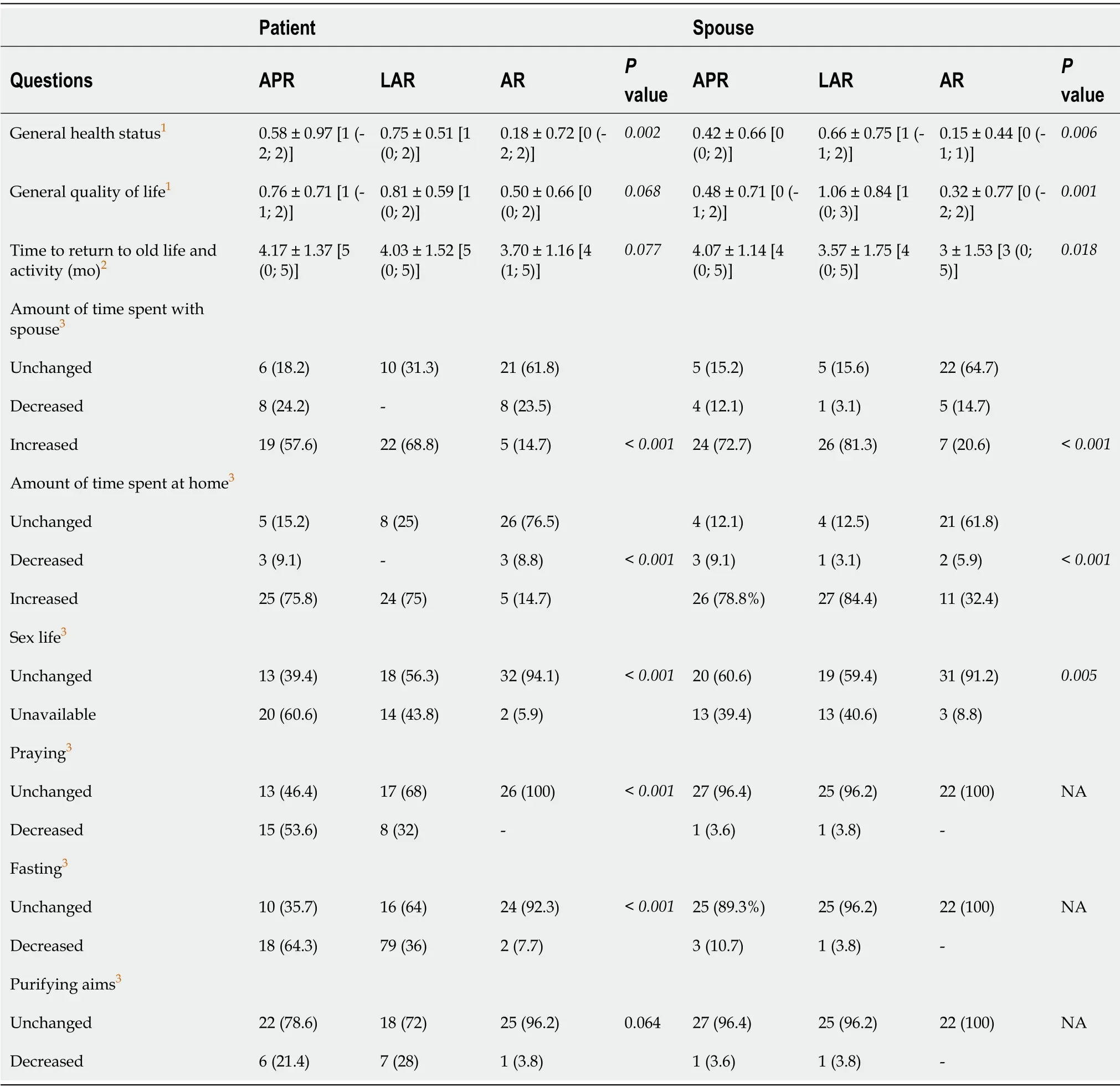
Table 5 Evaluation of the Ankara University Life Standards Questionnaire according to the type of surgery
The time it takes to return to former activities of daily living and work capabilities was increased following APR and LAR,but these increases were not statistically significant (Table 5).Furthermore,no gender differences were detected (data not shown).Patients who underwent either LAR or APR spent more time together with their spouse and more time at home following surgery than patients in the AR group(Table 5).Moreover,male patients’ spouses spent significantly more time with their husbands (P= 0.009;while 71.4% of male patients’ spouses reported that they spent more time with their husbands,only 40.9% of female patients’ spouses said the same)and spent more time at home (P<0.001) than female patients’ spouses (the proportion of spouses who spent more time at home was 82.1% and 43.2% for male patients’spouses and female patients’ spouses,respectively).Alterations to the patients’ sexlives were significantly more common following LAR and APR than AR (Table 5).Regarding the religious worship of patients,praying and fasting activities were decreased after surgery;these decreases were significant in the LAR and APR groups compared with the AR group.There were no changes in the praying and fasting activities of spouses (Table 5).The fulfillment of religious activities decreased in male patients compared with female patients (data not shown).
DISCUSSION
The evaluation of the consequences of diseases and treatments on patient-reported outcomes,such as QoL,has gained extensive attention[8,13-17].In fact,the diagnosis of cancer and the associated treatment process have considerable social,physical,psychological,and sexual impacts for both patients and their spouses.Little information is available regarding spouses’ QoL following colorectal cancer surgery.Depending on the localization of the colorectal carcinoma,either sphincter-saving or sphincter-sacrificing radical surgery can be performed.All procedures have a significant impact on patients’ QoL.The stoma itself can disrupt rectal function owing to the presence of a low anastomosis.Moreover,significant sexual and urological dysfunction has also been reported,mainly due to damage to the autonomic pelvic nerve plexus[1].Colorectal cancer diagnosis and treatment are not isolated experiences[18].Spouses are the most frequent providers of support to patients with colorectal cancer.Patients with cancer and their caregivers (e.g.,spouses) experience emotional distress,physical problems,psychological difficulties,and sexual problems related to changes in their life[19,20].The present study aimed to evaluate the QoL following surgery for colorectal cancer,namely,AR,LAR,and APR,in both patients and their spouses during the same time frame.
The present study revealed a significant relationship between the disability levels of patients and their spouses in terms of both the total score and subscales (self-care,life activities,and participation in society) of the WHODAS-II.There were also positive correlations between the QoL of patients and their spouses for most of the subscales(bodily pain,general health,vitality,social function,emotional role,mental health,and MCS) of the SF-36.When the evaluations were conducted separately for each surgical procedure,there was an increase in postoperative disability levels in patients for all surgery types;however,the level of disability was minimal in patients following AR when compared with patients who underwent LAR or APR.Similarly,there was a decrease in the patient QoL for all surgery types during the postoperative period as measured by all subscales of the SF-36.However,this deterioration was minimal in the AR group when compared with the LAR and APR groups.
As hypothesized,we found decreases in the QoL scores over time in the spouses of patients with colorectal cancer when measured with the SF-36,specifically in the“vitality,” “social function,” “emotional role,” “mental health,” and MCS subscales.Additionally,we found an increase in spousal disability over time for the “life activity” and “participation in society” subscales and the total score of the WHODASII.Similarly,Badgeret al[21] showed that 25% of partners often suffer the same or higher levels of emotional distress compared with cancer survivors.In fact,cancer treatment,with its collateral side effects,produces physical and emotional disturbances that influence QoL.A study by Graça Pereiraet al[3],which compared different modes of treatment (i.e.,surgery,surgery plus chemotherapy,or surgery followed by radiotherapy) in colorectal cancer,demonstrated that patients who received only surgery had lower levels of depression,anxiety,and traumatic stress symptoms when compared with patients who received surgery plus chemotherapy or surgery plus radiotherapy.Similar results were found for the spouses of patients undergoing these treatments.
Previous studies on changes in the QoL of spouses of patients with breast and prostate cancer have not explored gender-related differences in QoL,as doing a gender-based comparison is only meaningful in gender nonspecific cancers such as colorectal cancer[2,22,23].In the present study,there was an increase in postoperative disability for all subscales of the WHODAS-II for both genders,but these increases were not statistically significant except for the “life activities” subscale,which showed a significant increase the score among female patients and male patients’ spouses.The“participation in society” subscale also showed a significant increase among female patients’ spouses.
The results of the Ankara University Life Standards Questionnaire show that patients’ and spouses’ perceptions of their own general health and general QoL significantly decreased following patients’ surgeries.Many studies in the literature have compared patients who underwent LAR with patients who underwent APR,and the general consensus in these publications is that there exists a possibility of LAR syndrome in patients with very low-level anastomosis,which has a negative effect on QoL.In these patients,constipation,diarrhea,frequent stools,and the development of fecal incontinence is a major problem that decreases QoL[24-26].In our study,when the types of surgery were compared,there was a distinct deterioration in the LAR group.However,there were no gender differences between the patients and spouses.We found that patients and their spouses tended to spend more time together and at home following surgery,especially in the LAR and APR groups.Interestingly,we found that male patients’ spouses spent significantly more time with their husbands and spent more time at home than female patients’ spouses.This situation significantly impacts the lifestyle of male patients’ spouses.As mentioned previously by Cakmaket al[27],this may be because male patients are more willing to have their colostomy care managed by their wives.Changes in sex life were significantly more common following LAR and APR than in the AR group.
With regard to the religious attitudes of patients,the literature suggests that religion is an important factor in coping with cancer[28,29].Shaheen Al Ahwalet al[28] found that religiosity is associated with fewer depressive symptoms and fewer suicidal thoughts in Muslim patients with colorectal cancer.We found that religious activities,such as praying and fasting,decreased significantly in the LAR and APR groups when compared with the AR group,whereas there were no changes in praying and fasting in spouses.This is probably because of the importance of cleanliness and the desire to be free of any fecal material,especially when praying in Islam.We also found that fulfillment of religious duties decreased more among male patients than among female patients.
Although the present study has shown valuable findings,its design is not without certain flaws.The main limitations could be counted as followed:The first concern is to include the patients who underwent AR for sigmoid colon cancer.AR is a different type of surgery compared to LAR and APR.It is already known that these patients have better functional and sexual outcomes.Another limitation is about the exclusion criterias;patients with major morbidity were excluded from the study.Complications are an unavoidable aspect of colorectal surgery.It may be better to eveluate the effects of major complications in QoL scoring.
CONCLUSION
Colorectal cancer surgery has a significant effect on the QoL of both patients and their spouses,with a greater impact on male patients’ spouses.Preoperative counseling regarding potential problems should therefore collectively address the patient and their spouse as a couple rather than the patient alone,particularly for patients undergoing LAR and APR procedures.
ARTICLE HIGHLIGHTS
Research background
We hypothesized that colorectal cancer surgery affects not only the patient’s physical,social,and psychological aspects of lifestyle,but also the quality of life (QoL) of the patient’s spouse.
Research motivation
Although there are many studies investigating the QoL in patients who have colorectal cancer none of these focus on the spousal QoL.To the best of our knowledge,this is the first prospective and comparative study investigating the QoL following colorectal cancer surgery in both the patients and their spouses during the same time frame.
Research objectives
The aim of this prospective and comparative study was to investigate the QoL of patients and their spouses.
Research methods
Patients who remained well a minimum of 5 years after curative surgery for colorectal carcinoma and their spouse's as well were included in this prospective study.Both patients (n:100) and their spouses (n:100) filled SF-36 (Medical Outcome Study 36-item Short Form Survey) and WHODAS-II (World Health Organization-Disability Assessment Schedule II) preoperatively (preop),and postop 15-18 mo.
Research results
There were statistically significant positive correlations between the disability scores of both patients and their spouses for the ”self-care”,”life activities” and ”participation in society” subscales of WHODAS II and the total score for WHODAS II (P <0.01;for each).There were also positive correlations between the life quality of both patients and their spouses in most of the subscales of SF-36.Statistically significant correlations were found for ”bodily pain”,“general health”,”vitality”,”social function”,”role emotional”,”mental health” and MCS subscales of SF-36 (P <0.05;for each).When the gender differences were evaluated,it was found that the QoL of female spouses changed more than male sp ouses for all subscales of WHODAS-II.
Research conclusions
Patients as well as their spouses QoL was affected following colorectal cancer surgery.These changes detected more significantly in female spouses.
Research perspectives
Randomized controlled trials are expected to be conducted to measure the effect of counseling of the patients with colorectal cancer and their spouses.
杂志排行

World Journal of Gastrointestinal Surgery的其它文章
- Trends of rapamycin in survival benefits of liver transplantation for hepatocellular carcinoma
- Role of minimally invasive techniques in gastrointestinal surgery:Current status and future perspectives
- Fluorescence in situ hybridization-based confirmation of acute graftvshost disease diagnosis following liver transplantation:A case report
- Three colonic cancers,two sites of complete occlusion,one patient:A case report
- Perioperative steroid administration reduces overall complications in patients undergoing liver resection:A meta-analysis
- Literature review of the outcome of and methods used to improve transperineal repair of rectocele