Ocular trauma in an urban Spanish population:epidemiology and visual outcome
2021-09-14MartaBelmonteGrauGuadalupeGarridoCecaPaulaMarticorenalvarez
Marta Belmonte-Grau, Guadalupe Garrido-Ceca,2, Paula Marticorena-Álvarez
1Department of Ophthalmology, Hospital Universitario de La Princesa, Madrid 28006, Spain
2Universidad Autónoma de Madrid, Medicine University,Madrid 28006, Spain
Abstract
● KEYWORDS: ocular trauma; epidemiology; domestic accident
INTRODUCTION
Eye trauma continues to be an important health problem worldwide. It is one of the principal causes of unilateral loss of visual acuity (VA)[1], with great socio-economic and psychological repercussions[1-2]. Despite advances in treatment,the prognosis for these injuries is still uncertain[2-5]. They pose a challenge to ophthalmic surgeons, given the variety of lesions and the affectation, in many cases, of both eyeball segments.Each year an estimated 72 000 people suffer eye trauma leading to loss of VA[1]. Most of these injuries are produced in foreseeable circumstances, and therefore could be prevented by means of appropriate eye protection. Among the most established risk factors are age, gender, socio-economic status and life style[2].The epidemiological aspects of eye trauma are highly dependent on the area of population studied[6]and it is useful to be familiar with these in order to identify the scenarios and individuals at risk. However, whereas the epidemiological characteristics of eye trauma in adults have been extensively described in the United States, United Kingdom or Hungary[2],they have not been well defined in other European countries such as Spain, where only limited literature on this topic is found[1,3-4,6-8].
During the 1980s, traumatisms to the eye were the first cause of anatomical loss of the eyeball in Spain[7]. Later, from 1980 to 1991, the first multi-centre prospective study[9]was carried out on a sample of 1378 eyes. The study revealed that 23.20%of eye trauma cases were due to occupational accidents,with domestic accidents following closely at 22.50%. The most recent study, published 10 years ago[1], examines the epidemiological characteristics of 92 patients with openglobe eye trauma in a south-eastern region of Spain where greenhouse farming is one of the foremost productive sectors.At present, in Spain, eye trauma is the third cause of blindness or significant after-effects, glaucoma and diabetic retinopathy taking first and second place[10].
Hospital Universitario (H.U.) de La Princesa provides healthcare service to an adult population of some 280 000 inhabitants.Centrally located in Madrid (Spain), and encompassing an area with high socio-economic levels and life expectancy rates that contains an abundance of night-life spots, bars and restaurants[11], this hospital offers a unique opportunity to study the epidemiology of eye trauma in an inner-city setting.
The principal aim of this study is to analyse the epidemiological characteristics of eye trauma patients requiring urgent surgery at a tertiary hospital in Madrid. A secondary aim is to identify the factors associated to the final visual outcome. This study may contribute to identifying risk scenarios and individuals at risk in the inner-city environment and thus, to developing the appropriate preventive measures to help reduce the incidence of this type of trauma.
SUBJECTS AND METHODS
Ethical ApprovalA retrospective descriptive study was conducted following the principles of the Helsinki Declaration.The study included all eye trauma patients reaching the emergency unit at H.U. de la Princesa requiring urgent surgery.All information relating to the patients, their injuries and the treatment administered was gathered from the hospital medical records. The data were anonymised and entered on a database specific to this study. The period studied was from January 2010 to April 2020 (10y and 4mo). Patients with non-traumatic spontaneous ruptures, non-surgical closed trauma and selfsealed corneal perforations were excluded from the study.
Injuries were sorted into categories according to Birmingham Eye Trauma Terminology (BETT)[12]; closed eyeball lesions including lamellar laceration and contusion and open-globe lesions subdivided into ruptures and lacerations [perforating,penetrating and laceration with intra-ocular foreign body(IOFB)].
The variables studied were gender, age, risk factors predisposing to more severe lesions (previous surgery, low VA, myopia magna, corneal ectasia), date of injury, affected eye and image test on arrival [computerised tomography (CT), radiography,ultrasonography]. In the initial physical exploration, we recorded the presence of associated damage to the eye (such as retinal detachment, vitreous hemorrhage, alterations of the crystalline)and lesions to the adjacent structures or fractures of the orbit wall were likewise evaluated. Regarding surgical operations,we collected: date, type of anesthesia applied, repairs carried out and complications, if any. Similarly, we analysed the number of operations conducted and VA at 6mo, which we recoded as final VA.
The causes of the lesions were classified as aggression,domestic accident, occupational accident, traffic accident and sport/leisure. VA was classed under two groups: <0.1 and ≥0.1(Snellen scale). VA of <0.1 at 6mo of undergoing surgery was considered as an unfavourable visual outcome. The location of the damage was determined as per the Ocular Trauma Classification Group[13]that orders lesions into three groups according to the area affected. Zone I comprises lesions limited to the cornea or limbus; Zone II, lesions up to 5 mm to the rear of the limbus; and Zone III, lesions extending beyond 5 mm behind the limbus. Patients were also separated into categories according to the Ocular Trauma Score (OTS)[14].
The statistical analysis was carried out using the SPSS 25.0 data processing programme. Categorical variables were analysed using the Chi-square test, applying Yates’ correction whenever necessary. Continuous variables were compared using the Studentt-test for equal variances in the case of homoscedasticity and for unequal variances in the case of heteroscedasticity (n>30, robust test for normality). To determine the strength of association, the odds ratio (OR) was used with a confidence interval (CI) of 95%. We studied the variables that were likely to influence the visual prognosis of patients in our sample by means of running a univariate analysis and introducing in the multivariate Logistic regression model those withP≤0.10. By comparing the likelihood ratio test we obtained the parsimonious model.P-value ≤0.05 was deemed statistically significant.
RESULTS
Over a period of 10y and 4mo, a total of 92 patients were studied (n=92 eyes) of which 59.8% (n=55) were male and 40.2% (n=37) female. Mean age was 54.76±22.18y, the mean among women (64.38±22.90y) being higher than mean age in men (48.29±19.33y,P<0.05). Totally 35.13% (n=32) of the sample were over 65y. The incidence rate was 1.45 cases per 100 000 inhabitants per year. Details of the distribution by age and gender are given in Table 1.
On examining the activity engaged in at the time of sustaining trauma, we observed that the most frequent cause was domestic accident (44.60%), followed by aggression(22.80%) and occupational accident (17.40%). Of the domestic accidents, 61% (25 eyes) occurred in patients >65y (P<0.001),lesions from aggression were sustained in 66.70% (14 eyes)of cases among the youngest patient group (P<0.001) and occupational accidents were more common in the 15-45 years age group (8 eyes, 50%;P<0.001). Patients over 65y presented an OR=10.71 (95%CI: 3.47-33.09,P<0.001) for suffering a domestic accident, in comparison with other age groups.Patients in the 15-45y and 46-65y age groups were found to be at greater risk of trauma through aggression [OR=17.52(95%CI: 2.14-143.70) and OR=10.94 (95%CI: 1.22-98.56);P<0.001 respectively] compared against patients >65y. With regard to trauma and gender, trauma was sustained in the homemore often by women (53.66%; female:male ratio=1.16:1,P=0.011) while trauma through aggression was more frequent among men (85.71%; male:female ratio=6:1,P=0.006). Details for causal mechanisms, as well as their relation to age and gender, are given in Table 2.
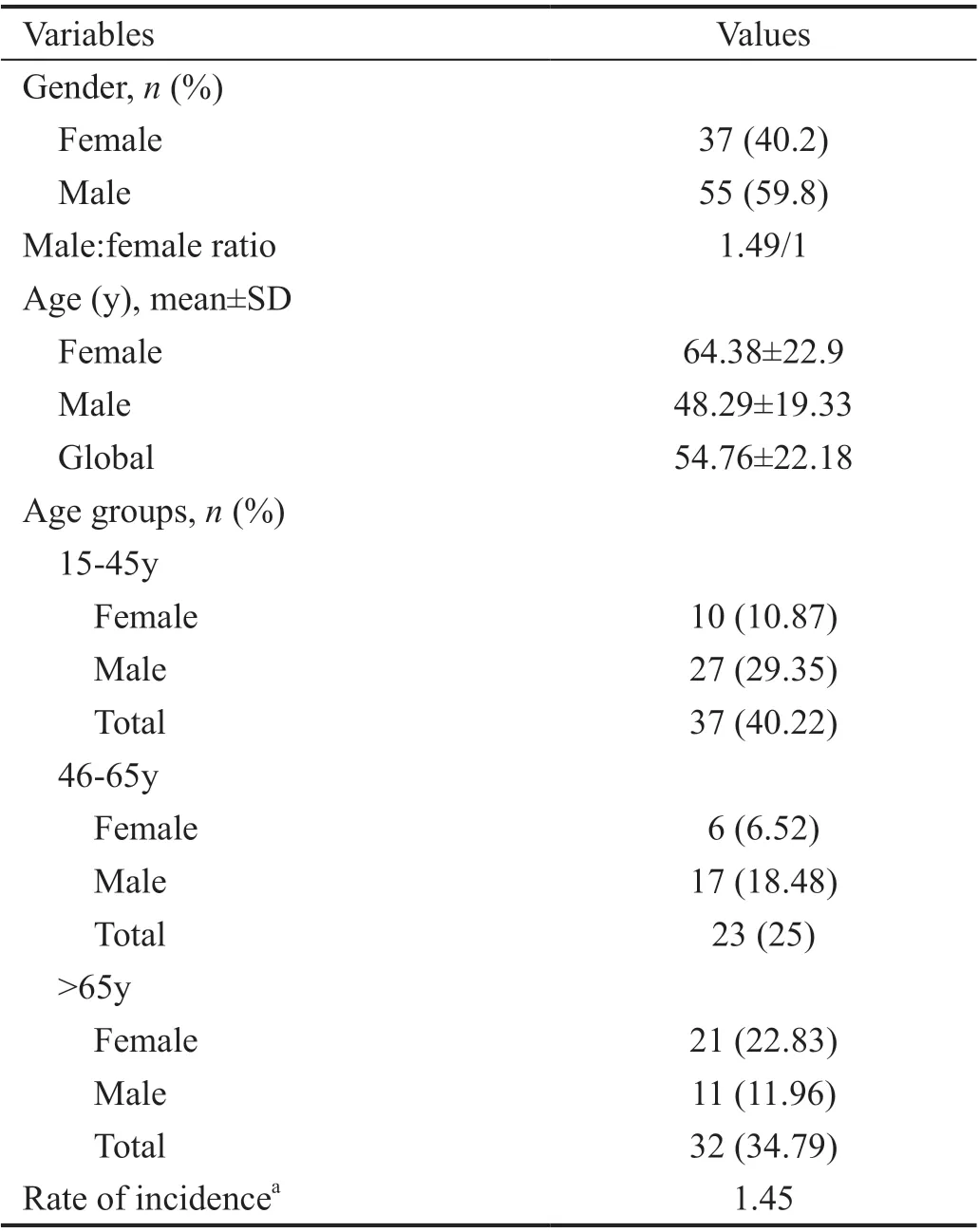
Table 1 Socio-demographic characteristics
As for types of trauma, blunt traumatisms (n=62, 67.40%)were more frequent than incisive traumatisms (n=30, 32.60%)except in the occupational accident subgroup, 56% of which were caused by sharp objects. Regarding types of injury,classified according to BETT, 63.04% (n=58) were open-globe lesions. The most common of these was rupture of the eye wall (n=36, 39.13%) followed by penetrating laceration (n=13,14.13%) and laceration with IOFB (n=8, 8.70%).
The region most frequently affected was Zone II (n=25,27.20%), followed by Zone I (n=23, 25%) and, lastly, Zone III(n=10, 10.90%). In one patient, the location of the lesion could not be determined. Moreover, 35.87% (n=33) of the traumas requiring surgery were closed-globe lesions. Details of the type and location of lesions are given in Table 3.
Initial VA and details of the medical exploration on arrival at the emergency unit are shown in Table 4. Hyphema was present in 51.09% (n=47) of cases. Of the patients, 26.10%(n=24) developed complications relating to the crystalline/intra-ocular lens (IOL), the most frequent initial complication being luxation of the IOL (n=7) followed by traumatic cataract(n=6). The retina was affected in 28.26% of cases (n=26).Patients with Zone III lesions (80%) sustained a higher proportion of retinal damage than those with Zone I (26.10%)and Zone II (40%;P=0.006) lesions. Relative afferent pupillary defect (RAPD) was observed during the initial exploration in 6.50% (n=6). Initial VA was recorded in 74 eyes, and VA at 6mo of surgery was noted in 47 cases. Patients with an initial VA of <0.1 totalled 48.65% (n=36). In 21.73% of cases two or more surgical interventions were needed and 5.43% were eviscerated. No instances of endophthalmitis or sympathetic ophthalmia were recorded. Final VA was <0.1 in 19.14% of patients and OTS was ≤3 in 52.20% of patients.
In the univariate analysis, we found that an OTS>3, being female and having a closed globe trauma were factors predictive of a favourable visual outcome. Similarly, being over 85 years of age, presenting in the initial examination retinal, choroidal or lens damage and fractures of the orbit wall were also associated with a poorer visual outcome (Table 5).On performing a Logistic regression with significant or close to significant variables (P≤0.10) we found that patients with retinal damage were 162.61 times (95%CI: 8.853-2986.685)more likely to have poor vision (<0.1) at 6mo than patients with no such damage (P=0.001). Patients in the over 85 age group were 42.11 times more likely to have poor vision (<0.1)than younger patients, this association being close to statistical significance.
DISCUSSION
This study shows that the causes of eye trauma requiring surgery vary with gender and age. The data support the idea that eye trauma patterns in a given region reflect the socioeconomic status of its inhabitants[4,15-16].
The incidence rate in the area studied (1.45 per 100 000 inhabitants/year) was notably lower in comparison to other similar studies[1,17-22]. This variability may be explained by the specific characteristics of the inner-city location of the healthcare district. As mentioned earlier, this area contains a population with a high socio-economic level engaged in highly qualified occupations[11]. These individuals are probably less exposed to occupational risks and, in the event of an occupational accident, are more likely to resort to private medical cover or a mutual insurer.
Men were more often involved than women, representing 59.80% of the sample. Other studies in this field of research have also reported the prevalence of men[12-14,17,21-25]. This may be due to the fact that men tend to occupy higher-risk jobs,engage in more dangerous sports and are generally more likely to be caught up in fights with varying degrees of physical aggression. We found an OR of 5.514 (95%CI: 1.49-20.39,P<0.006) for aggression in menvswomen.
Focusing on the female group, women suffered domestic accidents more often in their elderly years. In our series, thewomen showed an odds ratio of 3.20 (95%CI: 1.298-8.204,P=0.011) for accidents in the home as opposed to men. Women have traditionally borne a greater burden in household tasks,and it is common knowledge that the elderly population is increasingly feminine, with a life expectancy of 86.22yvs80.87 for men[26]. With age, the risk of accident also increases;mobility and dexterity worsen, and co-morbidities appear that may include eyesight alterations.

Table 2 Causes of trauma by age and gender

Table 3 Lesion type and location n (%)
Moreover, the mean age in our series was 54.76±22.18y,notably higher than in other similar studies[4,7,19,27-28]. These differences were yet more visible between the sexes, the mean age among men being 48.29y and among the women 64.38y.This variability may also be justified by the demographic characteristics in the chosen healthcare district, home to an ageing population in which 22.57% is ≥65y of age and up to 11.42% of homes consist of one woman aged ≥65[29], with a high ageing index (209.52% in contrast to the provincial mean of 105% and a national mean of 120%), as well as over-ageing(37.96%)[26].
In our series, most of the accidents happened at home(44.60%). We have found similar data in some studies in which between 44.40%-51.80% were domestic accidents[8,16,19-20]. Thesecond most frequent cause (up to 22.80%) were instances of aggression, while occupational accidents came third (17.40%).This figure is low in comparison with previous studies in which we found that occupational accidents account for around one third of all traumatisms[1,8,19,21,30-31]. Especially noteworthy is the study by Grupo para el Estudio Multicéntrico de los Traumatismos Oculares en España (GEMTO)[9], in which occupational accidents were identified as the most frequent cause of severe eye trauma in Spain between 1989 and 1991.
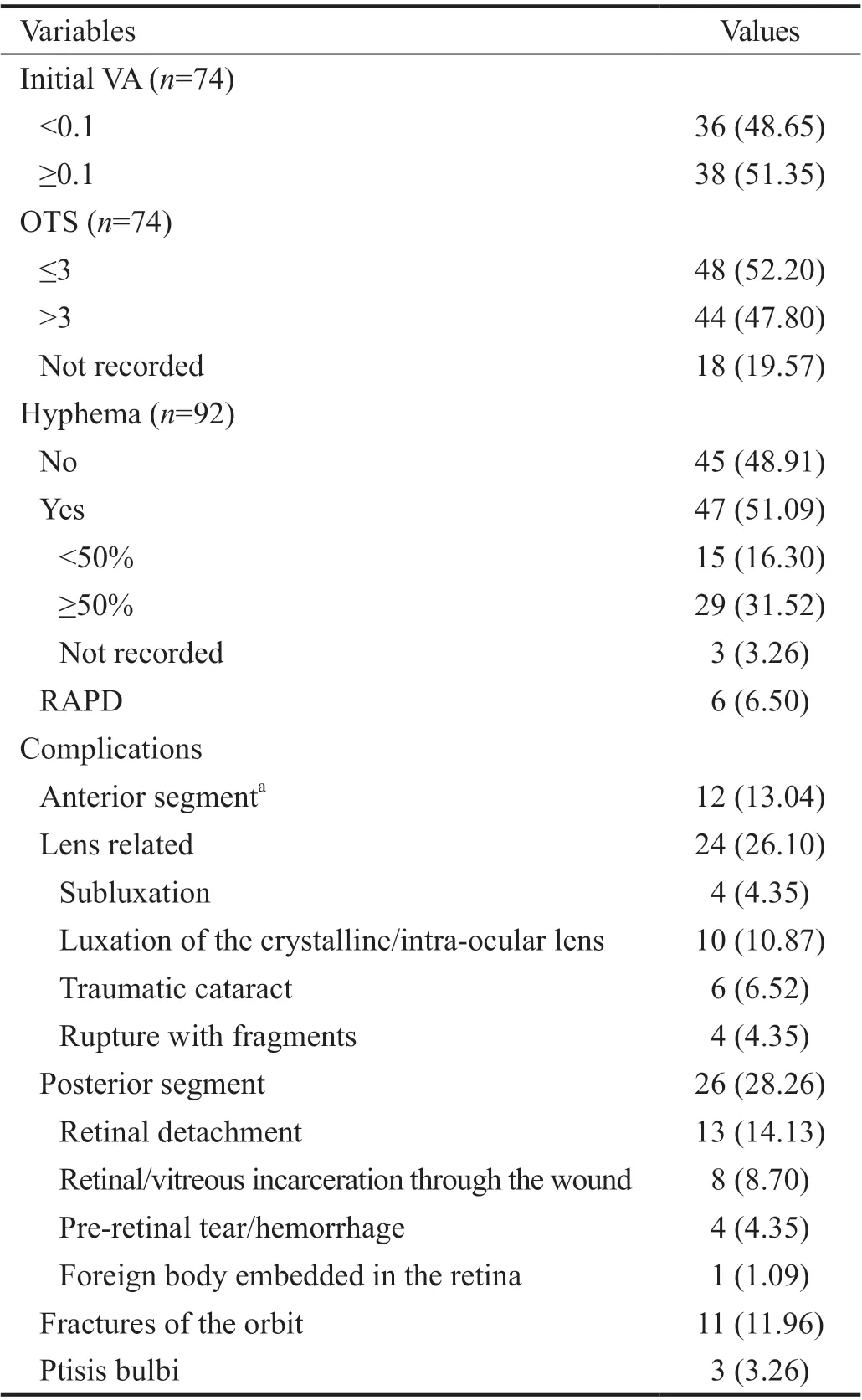
Table 4 Clinical characteristics of the lesion n (%)

Table 5 Univariate and multivariate analyses of potential factors affecting the final visual outcome
The lower incidence rate of eye trauma at the workplace in our series may be due, as mentioned earlier, to the socio-economic characteristics of the area of influence. According to Social Security enrolment data, the residents in the studied area are mainly engaged in the services sector (93%) and to a much smaller extent in agriculture (0.16%), industry (4.14%) or building (2.64%)[11]. By enrolment groups, the most prevalent are engineers, graduates and top management post-holders.
With respect to aggression as the second most frequent cause in our series, this may respond to the abundance of bars,restaurants and night clubs in the area[11]. As our results indicate, it was those under 65 years of age who were most at risk of aggression related injury.
As for home-related injuries, they occur from casual falls,performing maintenance tasks or risky activities on elderly patients where eye protection is often neglected. Information of the population about risky activities and how to avoid them should be enhanced[24,32-33].
As for the mechanism by which injuries are sustained, we found that blunt trauma was more common than incisive trauma, and that the region most often affected was Zone II.This area, according to several published works, is the most commonly affected among citizens over 65y[34-35]. Nonetheless,the GEMTO study[9]reported a higher frequency of injuries solely to the cornea (51.9%) in open-globe trauma. Our data may be explained by the fact that blunt trauma is produced by objects that cause a sudden increase in intraocular pressure and rupture at a point distant from the place of impact. Moreover, our cases were selected through a search for cases of eye trauma requiring urgent surgery. Corneal lesions that did not require surgery (e.g.self-sealed lesions)were dismissed.
Although in the majority of studies the percentage of endophthalmitis stands at around 1%-5% of the sample[8,18,36-37],no cases were recorded in our series. Probably, this was due to the fact that we performed early primary closure and applied intravenous antibiotic therapy, that most traumas occur in the urban environment, and to the small incidence of IOFB in our sample.
Primary surgery was performed urgently by the surgical oncall team with the aim of ensuring the early closure of the wound. When the posterior segment was affected, surgical repair of the lesion was deferred, as normally there is no team available comprising a surgeon and instrumentalist specialising in vitreo-retinal surgery. In these situations, and whenever complications arose, secondary interventions were necessary(21.73%). Evisceration merits special mention as we found that 5 (5.43%) of our patients required this surgical intervention.We identified similar percentages in other studies[27,37].
In Logistic regression analysis, old age and retinal involvement were found to be associated with higher rate of unfavourable visual outcome. These factors have already been described in previous literature[8,27,38-40]. Although in the univariate analysis we observed significant differences with several factors also described in the existing literature (OTS, choroidal involvement, orbit wall fractures), these differences were not significant in the multivariate analysis[8,19,27,30].
Lastly, it must be highlighted that almost 50% of patients had an initial VA of <0.1 and that after receiving the appropriate care and treatment this percentage dropped to 19.14% at 6mo,despite the fact that a high percentage of the sample (52.20%)presented an OTS≤3, unfavourable from the point of view of visual prognosis.
The limitations of this study are its retrospective nature, and insufficient documentation relating to eye protection measures and to initial and final VA. This last item may be ascribed to the patient’s circumstances at the time of arrival at the emergency unit, that may have involved low conscience level,being stretcher-borne or uncooperative. Final VA data could not be collected for patients from different areas until they were transferred to their reference hospital after surgery. In addition, we did not include patients under 15y or patients with injuries that did not require surgery.
Therefore, it would be of great interest to avail of a nationwide database, as is the case in other countries [United States Eye Injury Registry (USEIR) or Hungarian Eye Injury Registry (HEIR)] to guarantee complete data records on cases of eye trauma to facilitate more exhaustive analyses, in order to conduct specific prevention campaigns targeting high-risk population groups.
To sum up our findings, the causes of severe eye trauma in urban Madrid vary with age and gender, aggression being more common in younger patients and domestic accidents in the over 65 age group. The data suggest that retired citizens are a high-risk group vulnerable to severe ocular injury and,therefore, should receive specific messages raising their awareness toward prevention. Further, the increasing severity of accidents in the home environment should encourage ophthalmologists and authorities alike to promote the adoption of eye protection measures for tasks conducted without the workplace.
In conclusion, the causes of severe eye trauma vary with age and gender, aggression being more common in men under 65 and domestic accidents in women over 65. Domestic accidents are more relevant than workplace accidents in older urban areas with high socio-economic status. It would be desirable to carry out specific prevention in older age groups. Despite the rapid establishment of treatment, the severity of injuries can lead to serious and irreversible visual loss.ACKNOWLEDGEMENTS
Conflicts of Interest: Belmonte-Grau M,None;Garrido-Ceca G,None;Marticorena-Álvarez P,None.
杂志排行

International Journal of Ophthalmology的其它文章
- Five-year results of refractive outcomes and visionrelated quality of life after SMlLE for the correction of high myopia
- Role of glycolysis in retinal vascular endothelium, glia,pigment epithelium, and photoreceptor cells and as therapeutic targets for related retinal diseases
- Predictive value of retinal function by the Purkinje test in patients scheduled for cataract surgery in Kinshasa, DR Congo
- Simultaneous pars plana vitrectomy, panretinal photocoagulation, cryotherapy, and Ahmed valve implantation for neovascular glaucoma
- Displacement of the retina after idiopathic macular hole surgery with different internal limiting membrane peeling patterns
- Analogs of microgravity: the function of Schlemm’s canal, intraocular pressure and autonomic nervous during the head-down tilt test in healthy subjects