Determinants of COVID-19 vaccine acceptance and encountered side-effects among the vaccinated in Bangladesh
2021-09-11MdIftakharParvejSaminaSultanaMimmaTabassumSeefatMannanFirozAhmed
Md. Iftakhar Parvej, Samina Sultana, Mimma Tabassum✉, Seefat E Mannan, Firoz Ahmed
1Department of Statistics, Noakhali Science and Technology University, Noakhali 3814, Bangladesh
2Department of Obstetrics and Gynecology, President Abdul Hamid Medical College, Bangladesh
3Department of Social Work, Noakhali Science and Technology University, Noakhali 3814, Bangladesh
4Department of Microbiology, Noakhali science and Technology University, Noakhali 3814, Bangladesh
ABSTRACT
KEYWORDS: COVID-19; Vaccination; Determinants; Vaccine acceptance; Side-effects; Bangladesh
1. Introduction
The coronavirus disease 2019 (COVID-19) is a deadly infectious disease, which was firstly reported in Wuhan city, Hubei province,China[1,2]. It has become a major threat in almost every country around the world[3]. As of May 18, 2021, more than 163 million confirmed cases have been reported with more than 3 million deaths globally[4]while more than 78 thousand confirmed cases and 12 181 deaths occurred in Bangladesh[5]. Currently, Bangladesh has been swept by a new COVID-19 wave that has seen daily infections rise sevenfold and deaths triple from the first week of April, 2021. Considering the situation, the Bangladesh government has taken many measures like strict lockdown, restriction of movements, expanded treatment facilities and extended campaign on health and hygiene in news media etc[6]. The Government of Bangladesh (GoB) launched a mass vaccination program in February 2021 to protect the people from COVID-19 pandemic[7].
We know that there are many people who are very much against vaccination. From the smallpox vaccine to the ongoing polio-DPT vaccine, campaigns are underway against vaccination[8,9]. Moreover,recent surveys in different countries have shown that some people are reluctant to take the COVID-19 vaccine[10]. Recently many such studies have been conducted to reveal the determinants of COVID-19 vaccine acceptance and reported diverse outcomes as 53.1%to 89.27%[11-17]. In another comprehensive survey of 19 nations,conducted in June 2020, the variables, either likely or very likely to take a vaccine, ranged from 55% to 89%[18]. However, another study conducted on vaccine acceptance in Russia showed the acceptance rate was 41.7% prior to vaccine availability, which increased to 63.2% after vaccines became available with verified safety and effectiveness[3].
Bangladesh is a highly populated country and is surrounded most of its border by India, which is facing a tremendous crisis now due to the second wave of COVID-19 pandemic[19]. Hence, we are in the midst of rapid infection spread with continuously mutating SARS-CoV-2 highly infective potential strains like Indian, UK,South African or Brazil variants[20,21]. In this emerging situation,vaccination of the people is essential to prevent the devastating COVID-19 pandemic. The undertaken step vaccination program of GoB is a timely intervention to prevent unprecedented loss of lives. Accordingly, people should spontaneously participate in the vaccination program commenced by the Bangladesh government.However, mass vaccine reception can be interfered by sociodemographic determinants such as level of education, economic status and cultural context etc. On the other hand, it has been reported that a huge amount of unawareness, rumours, and lack of information are prevailing among general people about COVID-19 vaccines from the very beginning of the COVID-19 pandemic[22].Hence, it is important to assess the spontaneity of vaccination among the people of Bangladesh in the current situation which will help the government to take necessary steps towards mass vaccination.
Furthermore, all vaccines may have minor side effects. Previous studies also documented side effects such as headache, fever,nauseous and muscle pain after getting the vaccine shots[23].According to public health experts, all these side effects are temporary reactions and these are signs that the immune system is kicking into action and getting ready to protect people from COVID-19[24]. Sometimes these side effects create reluctance in the public to receive the vaccine. There may be doubts in the minds of the people about the effectiveness of the vaccine that was prepared very quickly to protect the human race during the global COVID-19 pandemic. To date, certain clusters of people in Bangladesh have already received the COVID-19 vaccine. Their experience on side effects after receiving the vaccine may help increase the success of the COVID-19 vaccination program initiated by GoB. Therefore, our current survey has been conducted for determining the acceptability of the COVID-19 vaccine among the people of Bangladesh. This study aims to verify the acceptability of the vaccine based on factors influencing the vaccination program and accumulating information about the side effects from vaccinated people to help the government and policymakers of countries for taking necessary steps to cope with the challenges efficiently and effectively.
2. Subjects and methods
2.1. Study design and participants
This was a cross-sectional study conducted online, using social media platforms, such as Facebook, WhatsApp, messenger, and e-mails as well as some direct interviews. The respondents were the general population of Bangladesh aged 18 years and above.Participants encompassed all religions and races and represented various socioeconomic groups including different occupations.
2.2. Data collection tool
After preliminary review of relevant literature, a draft questionnaire had been developed, the majority of which had been drawn from previous similar studies and modified by the authors[11,15]. The draft self-administered questionnaire was bilingual (Bangla and English)and contained two sections. Section A contained the questions about the participant's socio-demographic background such as age,religion, education level, occupation, and current living area, etc.Section B included information about participant’s willingness to accept the COVID-19 vaccine including the type of side effects from respondents who already received the COVID-19 vaccine and other study variables. The questionnaire was first pre-tested in a sample of 50 Bangladeshi adults. This was then revised and finalized based on feedback from pre-test. The questionnaire was self-administered.
2.3. Data collection
The adult population of Bangladesh is approximately 104.97 million in 2019[25]. Considering a recently published study with 61% vaccine acceptance[26] and 2.5% error margin (95% CI 58.5%-63.5%), we calculated a sample size of at least 1 462. The study was conducted by applying a non-probability purposive sampling technique. The maximum questionnaire was sent on social media platforms for responses within a specific time period from April 17, 2021, to April 26, 2021. Before sending the questionnaires to the participants, the aim of the study was clearly articulated and formal consent was taken from each of them. Participants were allowed to join freely in the survey and were given the option to terminate the survey at any time. So, we only reached out to those who had access to the Internet and smart devices. Since many people(especially the old and illiterate participants in rural and semi urban)in Bangladesh do not have Internet access or smartphones and they do not understand the online survey, some face-to-face interviews were conducted using a convenient sampling methodology. To reach these respondents, social distancing and other safety issues were maintained with formal consent from each person. A total of 1 529 adults participated among whom online participants were 1 386 (90.65%) and face-to-face respondents were 143 (9.35%)in the study during the above-mentioned timeline. The survey did not require any personal information thus, confidentiality and anonymity of the respondents were confirmed. The researchers also did not pursue people for joining in the study, so the responses were unbiased. The study was approved by the Ethical Review Committee(approval No.: 74/2021) of the Science Faculty, Noakhali Science and Technology University, Noakhali, Bangladesh.
2.4. Statistical analysis
SPSS version 25.0 was used for the analysis of the data. Based on the objectives of the study, descriptive statistics (frequencies and percentage) were used to describe the demographic characteristics, to measure the COVID-19 vaccine acceptance, and to quantify the sideeffects of the vaccine as well as to describe other study variables.Chi-square test and multinomial logistic regression with 95%confidence intervals (95% CI) were used to explore the associations between demographic variables and willingness to get the vaccine.A P-value of less than 0.05 indicates the results are statistically significant at a 5% level of significance. Initially bivariate analysis(Chi-square test) was performed between the variables one at time.Those variables found to be significant at bivariate level (at P<0.05)were entered in to multivariate analysis using a logistic regression.When the questionnaire was categorized as willingness of vaccine acceptance analysis and perception on side effect analysis the Cronbach’s alpha values were 0.65 and 0.62, respectively. The standardized Cronbach’s alpha of the questionnaire is 0.68.

Table 1. Distribution of socio-demographic characteristics of respondents and willingness to receive the COVID-19 vaccine [n (%)].
3. Results
3.1. Socio-demographic characteristics
A total of 1 553 questionnaires were returned within the timeline after our call for participation in the survey, of which, 1 529 (98.45%)individuals completed the survey and 24 (1.55%) refused to participate.This includes 1 386 (90.65%) online respondents and 143 (9.35%)face-to-face interviewees. Among the respondents, male and female participants represented 1 012 (66.19%) and 517 (33.81%),respectively. The present survey comprised 972 (63.57%) urban, 296(19.36%) semi-urban and 261 (17.07%) rural respondents. In this study, only 90 (5.89%) would reject the vaccine if they are eligible for vaccination. On the other hand, 1 025 (67.04%) wanted to receive the vaccine, and 414 (27.08%) were uncertain about the acceptance of the vaccine. The distribution of socio-demographic characteristics of respondents and willingness to receive the COVID-19 vaccine was demonstrated in Table 1. Of the respondents, 610 (39.90%) participants were aged 40 years and above. Most of the participants were Muslim(87.25%) while 195 (12.75%) were other religion participants. When analysed educational status of the participants, at least 971 (63.50%)respondents completed their graduation. Almost half (42.45%) of the respondents’ monthly income was US$ 176.91-US$ 589.69. Most of the participants were healthy 1 209 (79.07%) and around 745 (48.72%)had no chronic diseases (Table 1).The postgraduate persons were more likely to accept the COVID-19 vaccine (80.00%). Respondents from other religions were more willing than Islam to receive the vaccine against COVID-19 (78.97%vs. 65.29%,χvalue=15.754 and P<0.001). Participants with income level below US$ 176.91 per month were the least accepting group of COVID-19 vaccination (49.54%). Urban people were more inclined to accept the vaccine (71.71%). Among the healthy participants, 844(69.81%) were more willing to accept the COVID-19 vaccine than people who are not good in health (Table 1).

Table 2. Acceptance of COVID-19 vaccine in comparison to different variables identified by logistic regression analysis.
3.2. Multinomial logistic regression analysis for acceptance of COVID-19 vaccine
Logistic regression analysis showed that the acceptance of the COVID-19 vaccine was associated with various factors which are presented in Table 2. Muslims were less likely to accept COVID-19 vaccine (OR 0.23; 95% CI 0.07-0.71; P=0.011) than other religions.As compared to higher secondary certificate and below, educated persons (undergraduate, graduate and postgraduate) were more likely to accept COVID-19 vaccine (undergraduate: OR 3.56; 95% CI 1.21-10.47; P=0.021; graduate: OR 3.00; 95% CI 1.26-7.18; P=0.013 and postgraduate: OR 3.43; 95% CI 1.23-9.51; P=0.018). Most notably,people living in urban areas were the most willing group to receive COVID-19 vaccine (OR 2.44; 95% CI 1.25-4.73; P=0.009). It was noteworthy that those who believed that vaccines protect against infectious diseases were more accepting of the COVID-19 vaccine(OR 10.08; 95% CI 3.96-25.64; P<0.001), participants who gave their opinion about vaccines have health-related risks were less interested to take the vaccine compared to the others who gave opposite response (OR 0.07; 95% CI 0.03-0.20; P<0.001). Moreover,participants in support of the development of natural immunity rather than receiving COVID-19 vaccine were less likely to receive COVID-19 vaccine in contrast to the participants who rely on vaccination to be protected from infectious diseases (OR 0.40; 95%CI 0.19-0.88; P<0.001) (Table 2).
3.3. Attitudes towards receiving the COVID-19 vaccine
To identify the factors of COVID-19 vaccine acceptance and rejection, we wanted to know the opinion from the respondents.About 984 (64.36%) participants believed that vaccines protect against infectious diseases, and 764 (49.97%) respondents felt that vaccination would stop the ongoing COVID-19 pandemic. On the other hand, the reason behind the unwillingness to receive the vaccine was that 927 (60.63%) were doubtful about the efficacy of the COVID-19 vaccine and 873 (57.10%) were worried about the side effects of the COVID-19 vaccine (Table 3).
3.4. Side effects after receiving COVID-19 vaccine
Table 4 presented the percentage distribution of side effects encountered after receiving the COVID-19 vaccine. Almost half(45.00%) of respondents in our study have already received the COVID-19 vaccine. Among them, only 125 (18.17%) felt mental pressure or stress, and more than half (57.41%) encountered different side effects within 48 h after receiving the vaccine. The majority suffered from fever (36.05%), muscle pain (31.69%), pain in the injection site (30.67%), and headache (23.40%). As a remedy for side-effects, 259 (37.65%) participants took medicines. Among the respondents who took medicine, the majority of participants(91.12%) received antipyretic.
4. Discussion
Vaccination has become a recognized approach in controlling and preventing of infectious diseases[27]. However, after long research and concerted efforts, vaccines against a number of diseases,including HIV, tuberculosis, and malaria have not been successful and these diseases are considered as persistent global health priorities in the world for several decades[28-30]. The journey to develop an effective cholera vaccine has already passed one hundredand fifty years[31]. Moreover, conventionally from the discovery of a vaccine to its application to the mass population requires several steps;notably, protective efficacy studies from animal models to human volunteers in various phases is extremely time consuming[32]. On the other hand, COVID-19 being an emerging rapidly evolving situation,has captured the overall media attention and many dialogues on the global health threats were conducted. As a result, major advantages availed using modern life sciences and global vaccine research and development set up in combination with experiences on a wide range of diseases as concerted efforts for providing vaccines against SARSCoV-2 virus within a short time. Pneumonia vaccines and its previous application have been particularly helpful in this regard. Considering the overall situation, the World Health Organization and all other health research organizations arranged faster approval of the vaccines for mass vaccination. Hence, within a short period, several COVID-19 vaccines have already been invented and some of them have already been allowed to apply to the public to prevent global community from the ongoing SARS-COV-2 pandemic[33-35]. However, these rapid discoveries in a short period of time in contrast to the mentioned vaccine implementation convention have raised suspicions among concerned citizens of all societies resulting in confusions and questions regarding their application. Thus, differences in COVID-19 vaccine acceptance were observed in many countries[36]. To ensure equitable distribution of the COVID-19 vaccine, it is crucial to make a projection of the acceptance in the public and identify the predictors associated with vaccine acceptance[37].

Table 3. Percentage distribution of the reasons behind the acceptance and rejection to receive the COVID-19 vaccine.
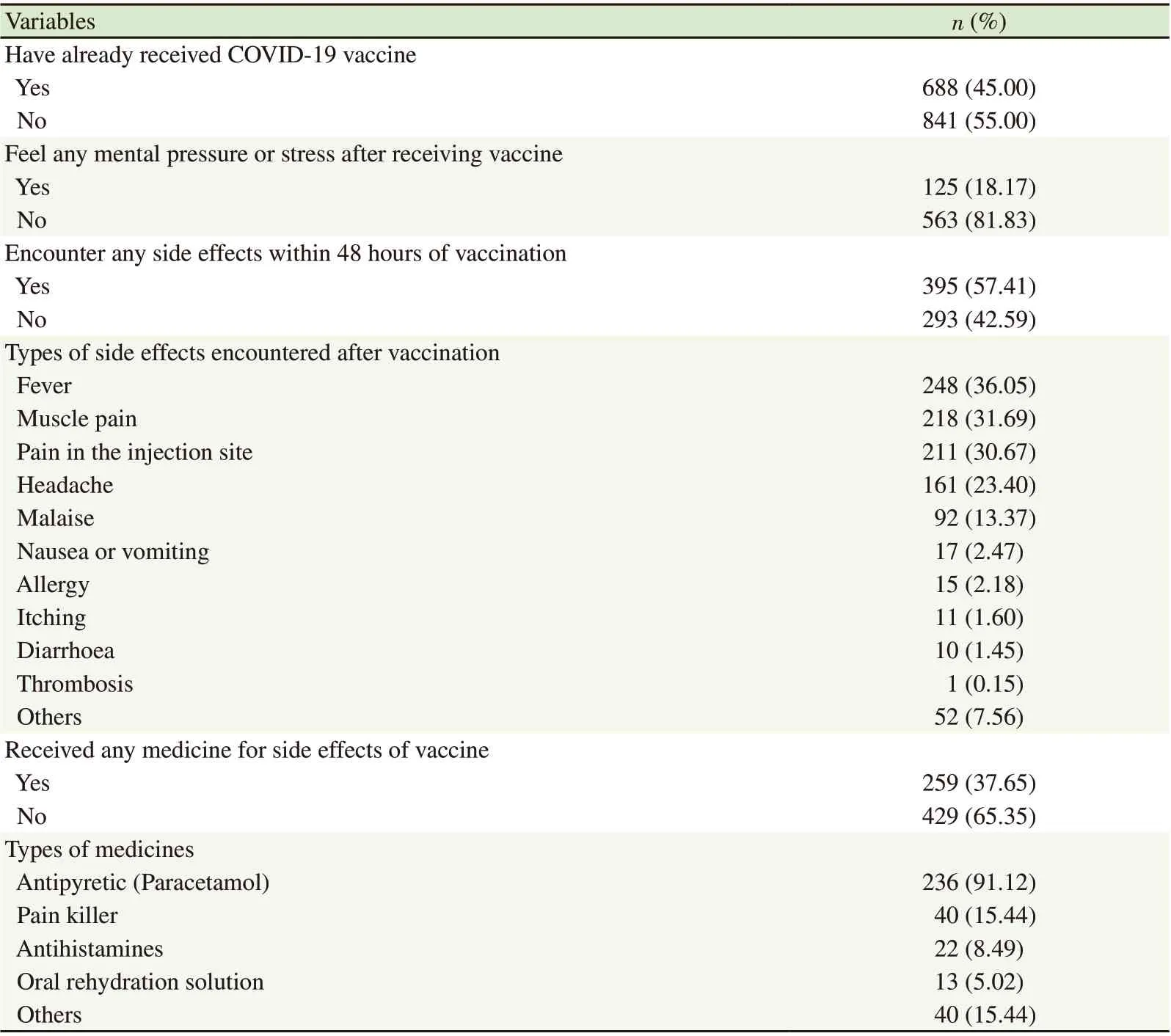
Table 4. Percentage distribution of side effect faced after receiving COVID-19 vaccine.
As the GoB has already launched a cluster-based vaccination program to control the COVID-19 pandemic, it is imperative that the initiative be successfully completed and hopefully protect all people of Bangladesh. To understand the public perception, this present survey was conducted in April 2021 at a time when the second wave of COVID-19 cases was increasing in Bangladesh. From this survey,we found that 67.04% agreed to receive the COVID-19 vaccine when the vaccine is available for all. Another study was also conducted among Bangladeshi population which found similar responses[38].The acceptance rate amongst the respondents of our survey was varied to other similar studies conducted in different countries. The acceptance rate of COVID-19 among Bangladeshi participants was consistently lower than that among residents of Australia (80%)[39],Denmark (80%)[40] and India (89.3%)[12]. Besides, the acceptance rate estimated in Bangladeshi studies were similar to those studies reported in the USA (67%-69%)[11,41], Saudi Arabia (64.7%)[16],and after verified the safety and effectiveness of vaccine in Russia(63.2%)[3]. Interestingly, Indonesian study correspondingly showed 93.3% and 67% acceptance upon 95% and 50% effectiveness of the COVID-19 vaccines[17]. However, our acceptance rate (82.28%) among health care providers was comparable with neighbouring countries as observed in India (79.3%)[42] and Pakistan (70.25%)[13]. In contrast,still a large proportion of respondents (27.08%) were uncertain and only 5.89% showed unwillingness to accept the COVID-19 vaccine.The main reasons were related to being reluctant towards receiving the COVID-19 vaccine included the doubt on the effectiveness of the vaccine (60.63%) and worries about the side-effects of the vaccine(57.10%). Such reasons have been reported in some previous studies in other countries[15,40,41]. For any newly introduced vaccine, safety has been reported as one of the major concerns in a systematic review manuscript on vaccine hesitancy[43].
Determining vaccine acceptability factors for immediate vaccination are complex and context-specific, which vary with time,place, and type of vaccines[16,43]. In addition, differences in race,religion, caste and education also generate differences in perception among people in developed and developing world on the COVID-19 pandemic and adopting vaccines for prevention[44,45]. In this study, we found statistically significant acceptability of COVID-19 vaccine with religion, education level and living area (urban). These socio-demographic factors were also found as significant factors for pandemic vaccine acceptability in the UK, France, Australia, US,and Japan[11,46,47]. In Saudi Arabia, only age was found as significant factors in determining the willingness of accepting the COVID-19 vaccines[16]. Another study in Kuwait identified only age and gender as significant factors for accepting the vaccine[15]. In the present study, age and gender has no significant effect on vaccine acceptance.As expected, results of our study revealed that participants who believed that vaccines protect against infectious diseases were more likely to receive the COVID-19 vaccine (76.28%) than those who did not believe that vaccines offer protection (32.26%). Likewise,vaccine acceptability was found statistically significant with those who indicated that vaccines do not have health-related risks. Besides,respondent’s perception on natural immunity is superior to immunity conferred by vaccination was found statistically significant in favour of acceptance of COVID-19 vaccine. In Kuwait, belief in vaccines protecting against infectious diseases and vaccines not having health-related risks were found as significant factors in determining the willingness of accepting the COVID-19 vaccines[15]. The vaccine confidence in the public would lower because of the uncertainties of new vaccines and new infectious diseases[48]. Although estimates of herd immunity and vaccination are changing rapidly, some of the estimates indicated at least 60% of a population needs to be vaccinated to achieve herd immunity[46]. From our study, we also found that 45.00% of respondents vaccinated till April, 2021 due to prioritizing approach of the GoB to vaccinate high risk group and the belief of common people that vaccines protect against infectious diseases (64.36%) and vaccination will stop ongoing the COVID-19 pandemic (49.97%). Hence, it requires extensive initiatives to be taken by the GoB to increase the number of vaccinated populations.
As mentioned earlier, the majority of the people have to participate in COVID-19 vaccination program to achieve population immunity.However, effectiveness of this particular vaccination program has become globally challenging because of concerns on vaccines’newness along with fear of adverse effects. Research findings on adverse effects also identified nocebo effects during COVID-19 pandemic that amplify and even induce adverse effects[49]. In our study, more than half (57.41%) respondents encountered side effects within 48 h of vaccination. Notably, fever (36.05%), muscle pain(31.69%) and pain in the injection site (30.76%) were predominant among the total vaccinated people. Factors such as headache, fever,nauseous and muscle pain were also reported in a prior study[23].However, only few respondents reported facing adverse effects like allergy (2.18%), diarrhea (1.45%), thrombosis (0.15%) among the total vaccinated ones. It has to be acknowledged that all those vaccines might cause unwanted effects. However, adverse effects that most people experience are only mild adverse effects which have been observed in our and other studies conducted for COVID-19 vaccine acceptance. These are also common phenomena with other established vaccines for mass vaccination like DPT, polio and Hib vaccines. It also needs to consider that not all symptoms that occur following vaccination are caused by the vaccine. However, to build trust and address concerns before escalating a level of fear that amplifies the negative experience, healthcare authorities responsible for vaccination programs will have to ensure prompt medical advice in case of adverse effects. Considering COVID-19 vaccines risk-benefit ratio, larger information campaigns and individual conversations may increase vaccine uptake. To accomplish the maximum outcome of the program, healthcare authorities of GoB can develop evidence-based ‘Easy-to-Access and Easy-to-Understand Information System’ to provide accurate information about vaccination adverse effects through positive framing of mild side effects and addressing misinformation based on studies conducted in Bangladesh.
This study has some limitations. First, we could not conduct a massive number of offline face-to-face surveys due to the COVID-19 pandemic and used the online platform to collect information that may limit the representativeness of the sample. Like other online surveys in the developing countries, there was low participation of people with lower educational levels and the illiterate as well as rural community representatives and the elderly. In addition, most of the participants (80.18%) were from explicable education level(undergraduate, graduate and postgraduate) who understood the online survey, so bias may still exist. Moreover, not all literate people are using smartphones. However, to overcome these limitations,some face-to-face interviews were conducted. Second, a convenience sampling technique adopted in this survey is a limitation of the study. All our respondents were from our acquaintances over online platforms (Facebook and WhatsApp, etc).
The most common causes of severe morbidity and mortality due to SARS-CoV-2 infection is pneumonia with additional extra pulmonary manifestations and major complications including acute myocardial injury, arrhythmia and shock mainly in elderly patients. Several recent studies have shown that the discovery of the COVID-19 vaccines have been successful in preventing the ongoing SARS-COV-2 pandemic in some regions of the world.The adverse effects of the vaccines are not serious and a very small proportion of vaccinated person encounter a minimum level of side effects. Therefore, it is very important to call for the prevention of devastating pandemic by creating awareness among the people of Bangladesh about the developed COVID-19 vaccines.This study focused on willingness to receive the COVID-19 vaccine in Bangladesh, taking into account the relationships with sociodemographic and health-related characteristics. Based on the previous history of pandemic vaccines and vaccine hesitancy as well as adoption, a well-structured research strategy might be required for achieving comprehensive acceptance of vaccines in every country.The results of our recent research will make significant contributions to the vaccination program of GoB and public health stakeholders in adopting specific approaches for the prevention of the COVID-19 pandemic. Further research is required to assess the perception of rural and illiterate populations which would help to incorporate them to the COVID-19 vaccination program. Hence, the policymakers urgently take the necessary step to make strategies to remove doubt on the efficacy of COVID-19 vaccines.
Conflict of interest statement
We declare that we have no conflict of interest.
Authors’ contributions
MIP, SS, and MT developed the concept and were involved in the design of the study. SS, MT and SM performed data collection and processing; MIP and MT analyzed the data; MIP, MT and FA wrote the methodology; MIP, MT, and SM wrote the draft manuscript with the guideline of SS and FA; MT, and FA supervised the whole study.All authors have read and approved the final manuscript.杂志排行

Asian Pacific Journal of Tropical Medicine的其它文章
- Prevalence and clinical significance of antiphospholipid antibodies among hospitalized COVID-19 patients
- Predictors of in-hospital mortality by logistic regression analysis among melioidosis patients in Northern Malaysia: A retrospective study
- EWMA control chart based on its first hitting time and coronavirus alert levels for monitoring symmetric COVID-19 cases
- Co-expression of HBZ, TAX and FOXp3 and HTLV-1-associated myelopathy/tropical spastic paraparesis development in HTLV-1-infected individuals: A systematic review
- Failure of space spraying to eliminate dengue virus-infected Aedes aegypti may explain failure to prevent secondary cases in Southern Thailand