Mesenchymal stromal cell-dependent immunoregulation in chemically-induced acute liver failure
2021-04-08JiaHangZhouXuanLuCuiLinYanXinYuShengHongCuiCao
Jia-Hang Zhou, Xuan Lu, Cui-Lin Yan, Xin-Yu Sheng, Hong-Cui Cao
Jia-Hang Zhou, Xuan Lu, Cui-Lin Yan, Xin-Yu Sheng, Hong-Cui Cao, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou 310003, Zhejiang Province, China
Hong-Cui Cao, Zhejiang Provincial Key Laboratory for Diagnosis and Treatment of Aging and Physic-chemical Injury Diseases, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou 310003, Zhejiang Province, China
Abstract Drug-induced liver injury (DILI), which refers to liver damage caused by a drug or its metabolites, has emerged as an important cause of acute liver failure (ALF) in recent years.Chemically-induced ALF in animal models mimics the pathology of DILI in humans; thus, these models are used to study the mechanism of potentially effective treatment strategies.Mesenchymal stromal cells (MSCs) possess immunomodulatory properties, and they alleviate acute liver injury and decrease the mortality of animals with chemically-induced ALF.Here, we summarize some of the existing research on the interaction between MSCs and immune cells, and discuss the possible mechanisms underlying the immunomodulatory activity of MSCs in chemically-induced ALF.We conclude that MSCs can impact the phenotype and function of macrophages, as well as the differentiation and maturation of dendritic cells, and inhibit the proliferation and activation of T lymphocytes or B lymphocytes.MSCs also have immunomodulatory effects on the production of cytokines, such as prostaglandin E2 and tumor necrosis factor-alpha-stimulated gene 6, in animal models.Thus, MSCs have significant benefits in the treatment of chemically-induced ALF by interacting with immune cells and they may be applied to DILI in humans in the near future.
Key Words: Mesenchymal stromal cell; Immune response; Drug-induced liver injury; Acute liver failure; Dendritic cell
INTRODUCTION
Drug-induced liver injury (DILI), the most common cause of acute liver failure (ALF) in developed countries, accounts for approximately 50% of ALF cases[1].In patients with hypersensitivity or reduced tolerance due to special constitutions, the immuneprivileged state of the liver can be disrupted by drugs and chemicals or their metabolites, such as reactive intermediate species[2], resulting in unbalanced immune cell infiltration and liver injury[3].
Mesenchymal stromal cells (MSCs) are widely studied adult pluripotent stem cells.They possess not only all of the common characteristics of stem cells but also immunomodulatory properties.They have been extensively researched due to their wide range of sources and easy availability.Since the first MSC transplantation in a pediatric patient experiencing grade IV treatment-refractory acute graftvshost disease (GVHD) in 2004[4], there have been an increasing number of studies demonstrating that MSC transplantation can effectively modulate the immune system in several immunerelated disorders.In addition to the ability of MSCs to migrate to damaged liver sites and undergo proliferation and differentiation into hepatocytes, the therapeutic mechanism of MSCs in ALF mainly depends on their potential immunomodulatory nature[5].
The main immune cells consist of neutrophils, T cells, B cells, natural killer (NK) cells, monocytes/macrophages, and dendritic cells (DCs).MSCs alter macrophages from a regularly activated (M1) phenotype to an either/or activated (M2) phenotype, resulting in reduced secretion of the proinflammatory cytokines, such as tumor necrosis factor-alpha (TNF-α), interferon-γ (IFN-γ) and interleukin (IL)-1, and increased secretion of the anti-inflammatory cytokine IL-10, which to a great extent is dependent on cell-to-cell contact or soluble factors, such as prostaglandin E2 (PGE2), indoleamine 2,3-dioxygenase (IDO), and TNF-α-stimulated gene 6 (TSG-6)[6].MSCs impact two stages of DCs: differentiation and maturation.When co-cultured with MSCs, DC precursors and immature DCs express lower levels of major histocompatibility complex class II (MHCII) and costimulatory molecules cluster of differentiation (CD) 86, CD80, and CD40, which result in a weakened ability to stimulate T cell proliferation.However, the immunosuppressive capacity of MSCs in mature DCs remains controversial[7].
Several studies have shown the inhibitory effects of MSCs on T cell activation, proliferation, and differentiation to T helper 17 (Th17) cells through PGE2, programmed cell death protein 1 (referred to as PD-1), and IL-10[8].Additionally, MSCs can stimulate the generation and proliferation of immunosuppressive regulatory T cells (Tregs)[9].Similarly, MSCs suppress the proliferation, activation, and antibody production ability of B cells and induce the B regulatory cells (Bregs)[10].
MSCs have been studied as a prospective therapy for the treatment of DILI and ALF due to their immunomodulatory ability.Several animal models of chemically-induced ALF have been used to study the mechanisms of DILI and the mechanisms of potentially novel therapies[3].MSCs can alleviate ALF by interacting with different immune cells because the main pathogenic immune cells differ in these animal models, and these discoveries in animal models will contribute to the clinical application of MSC-based strategies for the treatment of human DILI.
In this review, we summarize a number of existing studies on the interplay of MSCs and the immune system, and discuss some possible mechanisms underlying the immunomodulatory ability of MSCs in chemically-induced ALF.MSC-based therapy may be applied to DILI in humans in the near future.
IMMUNE SYSTEM RESPONSE TO CHEMICALLY-INDUCED ALF
The liver is an organ that is dominated by metabolic functions.It is inevitably exposed to the metabolites of various foods or drugs in the blood from the portal vein, which requires this organ to have high immune tolerance and self-repair abilities[2].Chemically-induced liver injuries refer to liver damage caused by chemical hepatotoxic substances, including alcohol, drugs, traditional Chinese medicines, chemical poisons from food, and organic and inorganic poisons in industrial production.On the one hand, the immune system of the liver has to tolerate the heavy antigenic load of daily food residues from the portal vein in a healthy state; on the other hand, it must respond efficiently to numerous viruses, bacteria, parasites, and chemical hepatotoxic substances[11].Excessive inflammation often contributes to morbidity and mortality in chemically-induced ALF (Figure 1).
Innate immune cells in response to chemically-induced ALF
In DILI, necrotic hepatocytes show many damage-associated molecular patterns (referred to as DAMPs), such as high-mobility group box-1 protein, DNA fragments, and heat shock proteins[12], and these factors can be identified by Toll-like receptors (commonly known as TLRs) on innate immune cells.Then, proinflammatory factors recruit inflammatory immune cells into the liver, activating them to remove necrotic cell debris[13].
Liver macrophages mainly include two cell types: resident Kupffer cells and infiltrating monocyte-derived macrophages.Although of different cellular origins, both types of macrophages can phagocytose microorganisms and metabolic waste in liver sinusoids.The numbers of liver macrophages become greatly increased in any type of liver injury, due to the self-renewal ability of Kupffer cells and the infiltration of monocyte-derived macrophages[14].In the early stages of liver injury, Kupffer cells recognize DAMPs derived from damaged hepatocytes and then secrete several proinflammatory cytokines and chemokines to attract neutrophils, NK cells, and bonemarrow-derived monocytes to the regions of inflammation[15].Ly6C+monocytes and Ly6C-monocytes exist in the blood of mice, and can differentiate into hepatic macrophages.Infiltrating Ly6C+monocytes promote inflammation and induce organ impairment, but eventually maturate with the downregulation of Ly6C expression, at which point they acquire the ability to restore liver integrity[16].
Neutrophils are the first-line immune cells that have the fastest response when inflammation occurs.However, uncontrolled neutrophil infiltration and activation lead to excessive inflammation in chemically-induced liver injuries.The expression levels of C-X-C motif chemokine ligand (referred to as CXCL) 1, IL-6, TNF-α, and monocyte chemoattractant protein-1 in the injured liver are significantly increased to regulate the infiltration and activation of neutrophils[17].Tissue-resident phagocytes, including macrophages and DCs, release a variety of proinflammatory mediators and establish a chemoattractant gradient, triggering neutrophil recruitment into tissues.Neutrophils express receptors (G protein-coupled receptor, Fc-receptors, adhesion molecules, TLRs, C-type lectins) that can recognize these signals and then release granules (myeloperoxidase), generate reactive oxygen species, and form neutrophil extracellular traps[18,19].
DCs in ALF engage in the innate immune response involving macrophages and neutrophils, with antigen recognition by pattern-recognition receptors.However, the most important effect of DCs is initiation of the adaptive immune response.DCs reside in organs such as the liver as immature cells, which are very effective at antigen recognition, capture and processing, and then circulate in the blood or lymph fluid to peripheral immune organs where they can achieve terminal maturation with the ability of efficient antigen presentation as well as activation of T cells[20].
In the healthy state, hepatocytes express MHC-I, which binds to inhibitory receptors on NK cells, preventing NK cell activation[21].In contrast, infected hepatocytes lacking MHC-I can be recognized and eliminated by NK cells[22].

Figure 1 Regulation of immune cells in response to chemically-induced acute liver failure.
Adaptive immune cells in response to chemically-induced ALF
Contrary to innate immune responses, which induce acute liver injury (ALI) in experimental animal models[13], adaptive immune responses play an undefined secondary role in DILI[23].In homeostasis, liver sinusoidal endothelial cells and Kupffer cells constitutively express IL-10, prostaglandins, TNF-α, and transforming growth factor-beta (TGF-β) to expand Tregs, attenuate T cell activation, and induce liver immune tolerance[12].In some ALI models induced by some special types of drugs or chemicals, T cells are important.Yuet al[24]found that IL-1β is upregulated in the AAGL (Agrocybe aegerita galectin) model and is crucial to recruit T cells from peripheral blood into the injured liver; treatment with IL-1β antibody can significantly alleviate hepatocyte damage.The possible mechanism may be inhibition of p38 or nuclear factor-kappa B (NF-κB) signaling pathways and subsequently reduced infiltration of T cells into the liver.Heymannet al[25]applied a concanavalin A (Con A)-induced liver injury model to mimic immune reactions observed in humans, trigger an inflammatory cascade by activating resident Kupffer cells, initiate neutrophil infiltration, and increase CD4+T cell infiltration and activation[26].Although Tiegset al[27]showed that CD4+T cells play a more critical role than CD8+T cells in Con Ainduced liver injury in wild-type mice, CD8+T cells played an important role in T celltransferred Rag2-knockout mouse (in which T cells cannot mature) challenged with Con A.Both IL-33 released by the injured liver and perforin secreted by CD8+T cells were crucial components in their study.
INTERACTION BETWEEN MSCS AND IMMUNE CELLS
Immune characteristics of MSCs
Quiescent MSCs display immune homeostatic features biased towards suppression.When MSCs are induced by various proinflammatory cytokines, these immunosuppressive properties can be considerably enhanced, resulting in polarization to immunosuppressive phenotypes of MSCs.IDO and inducible nitric oxide synthase (referred to as iNOS) are the key to the immune regulatory functions of MSCs, with a series of potential complementary suppressor pathways, including heme oxygenase-1, soluble human leukocyte antigen-G5, TGF-β, PGE2, galectin, and TSG-6[28].MSCs possess a pro-inflammatory or anti-inflammatory phenotype by contacting immune cell responses in different situations, and regulate the immune response by secreting soluble factors or direct cell contact[6].
Potential mechanisms underlying the immunoregulatory properties of MSCs through innate immune cells
MSCs can regulate the proliferation and activation of Kupffer cells, macrophages, DCs, neutrophils, and NK cells (Figure 2).MSCs reportedly transfer to injury sites in response to large amounts of inflammatory factors, such as IL-6 and TNF-α secreted by activated Kupffer cells[29].MSCs, in turn, inhibit the phenotype transition of activated Kupffer cells to M1 and stimulation of the NF-κB pathway in lipopolysaccharide (commonly known as LPS)-treated Kupffer cells[30].Several studies have revealed the mechanism by which MSCs cause immunosuppressionviathe interaction of macrophages.MSCs can interact directly and physically with innate immune cells.Upregulated CD54 on human MSCs (referred to here as hMSCs) co-cultured with M1 macrophages in anin vitroco-culture system increased IDO activity and inhibited the proliferation of T cells[31].Similarly, upregulated CD200 on mouse bone marrow stromal cells (BMSCs) in contact with M1 macrophages can also enhance the immunotherapeutic effects of MSCs to reprogram proinflammatory macrophages[32].On the other hand, soluble factors secreted by MSCs can contribute to the immunoregulatory properties of MSCs.Corneal-derived MSCs can secrete pigment epithelium-derived factor and then modulate the immunophenotype and angiogenic function of macrophages[33].TSG-6 and PGE2 secreted by MSCs have also been widely studied, due to their immunoregulatory effects on MSCs and macrophages[32,34].
In addition, MSC-derived exosomes, which are rich in proteins, mRNAs, and microRNAs (designated as miRs), have been used as a therapy for liver diseases in recent years.In a study of experimental autoimmune hepatitis, BMSC-derived exosomes, which are rich in miR-223, effectively alleviated liver injury by downregulating formation of the NLR family pyrin domain containing 3 (referred to as NLRP3) inflammasome[35].In another study, miR-17 derived from adipose tissuederived MSC (AMSC)-derived exosomes was shown to ameliorate LPS/Dgalactosamine-induced ALI by inhibiting activation of the TXNIP/NLRP3 inflammasome of macrophages[36].MSCs can limit neutrophil recruitment or infiltration and inhibit neutrophil activation to prevent an excessive inflammatory response.MSCs ameliorate the hepatic inflammatory response by reducing the release of neutrophil chemoattractant CXCL2 and attenuating neutrophil chemotaxisviadownregulation of C-X-C motif chemokine receptor 2 expression in neutrophils[37].In a septic mouse model, MSCs optimally balanced the distribution of circulating and tissue-infiltrated neutrophils, maximizing bacterial killing and minimizing liver injury[34].
Many studies have focused on the effects of MSCs on DCsin vitro, especially through soluble factors.One showed that TSG-6 secreted by mouse BMSCs suppressed the maturation and activation of DCs by inactivating mitogen-activated protein kinase and NF-κB signaling pathways[38].In addition, IL-6 reportedly participates in the immune regulation mechanism mediated by the murine MSC lineviainhibition of DCs[39].Regarding hMSCs, Spaggiariet al[40]demonstrated that human BMSCs can secrete PGE2 to inhibit differentiation of monocyte-derived DCs.Selleriet al[41]showed that human umbilical-cord-derived MSCs can secrete lactate to induce granulocytemacrophage colony-stimulating factor/IL-4-treated monocytes to differentiate into M2 macrophages rather than DCs by metabolic reprogramming.A study by Liuet al[42]showed that MSCs derived from mouse embryonic fibroblasts can induce a type of novel regulatory DCs that express low levels of CD11c and Ia and are phenotypically different from immature and mature DCsviaIL-10.
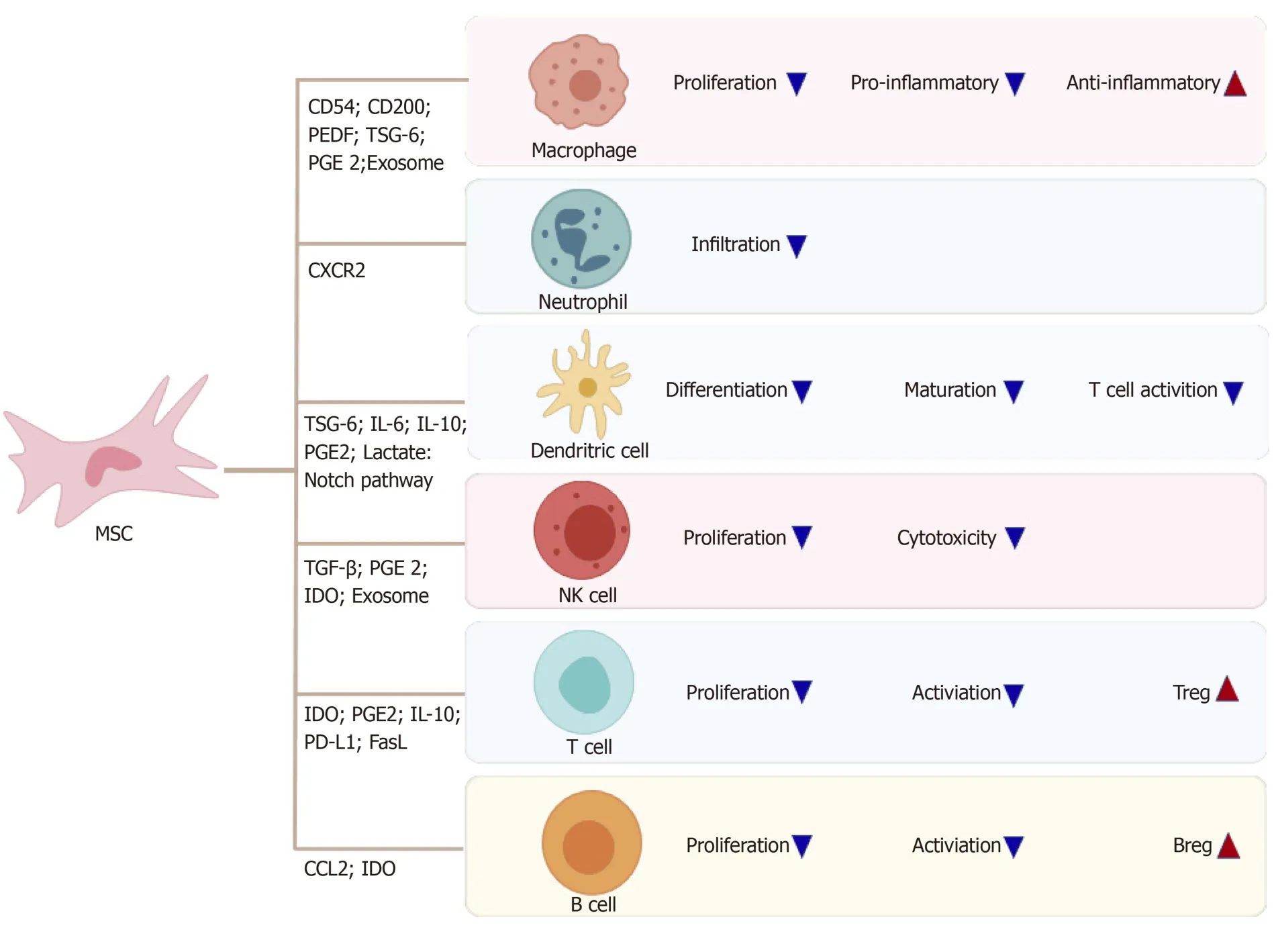
Figure 2 Mesenchymal stromal cells regulate innate and adaptive immune cells.
In addition, direct cell contacts are as important as soluble molecules in MSC/DC interactions.hMSCs can inhibit the proliferation ability and differentiation capability of CD34+hemopoietic progenitor cells into interstitial DCs but cannot inhibit maturation of CD34+hemopoietic progenitor cell-derived DCs, and the inhibitory effect is associated with the Notch pathway[43].Cahillet al[44]demonstrated that mouse MSC induction of functional tolerogenic DCs that can induce Tregsin vitrorequires Notch signaling.This hypothesis was confirmed in an animal model treated with Jagged-1 knockdown MSCs.In another study, mature DCs cocultured with MSCs expressing Jagged-2 acquired tolerogenic properties[45].MSCs can influence the proliferation capacity, cytokine release, phenotypic conversion, and cytotoxicity of IL-2-induced NK cells[46].The mechanism may include TGF-β[47], PGE2[48], IDO[49]and exosomes[50].Moreover, NK cells can stimulate MSC recruitment by secreting neutrophil-activating peptide 2[51], and activated NK cells can efficiently lyse MSCs[46].
Potential mechanisms of the immunoregulatory properties of MSCs through adaptive immune cells
MSCs can inhibit proliferation, activation, and differentiation of T cells, induce apoptosis of T cells and induce recruitment of Tregs.MSCs can also induce cell cycle arrest by downregulating cyclin D2 and upregulating p27kip1 in T cells, resulting in division anergy of activated T cells[52].Of note, MSCs can inhibit T cell function by inducing apoptosis of activated T cells.Plumaset al[53]showed that this apoptosis can be associated with transformation of tryptophan to kynurenine by IDO expressed by MSCs in the presence of IFN-γ.Akiyamaet al[54]revealed that BMSCs may trigger apoptosis of transient T cells through the Fas ligand (FasL)-dependent pathway, and that apoptotic T cells can induce production of TGF-β in macrophages, thereby upregulating Tregs.In some experimentsin vitro, MSCs were shown to inhibit allogeneic T cell responses in mixed lymphocyte reactions by IDO after MSCs were activated by IFN-γ[55].Recently, MSCs were shown to inhibit activation of CD4+T cells and reduce secretion of IL-2viaPD-1 ligands[56].
Several investigators have highlighted that MSCs can effectively inhibit Th17 differentiation.Duffyet al[57]demonstrated that this inhibition requires cyclooxygenase-2 induction, which is dependent on cell contact, leading to direct Th17 inhibition by PGE2.Quet al[58]also showed that MSCs inhibit Th17 cell differentiation, and suggested that increased secretion of IL-10 may play a role.One important aspect of the immunomodulatory effect of MSCs is the recruitment and influence of Tregs[59].MSCs can reinforce the regulatory function of CD8+CD28-Treg cells by increasing expression of IL-10 and FasL[60].They can also induce cell cycle arrest in the G0/G1 phase instead of induction of B-cell apoptosis in a soluble factor-dependent manner[61].Furthermore, MSCs inhibit proliferation and activation of B cells by modifying the phosphorylation levels of the extracellular signal-related kinase 1/2 or p38 pathways[62].Rafeiet al[63]clarified that MSC-derived chemokine (C-C motif) ligand 2 (referred to as CCL2) can suppress secretion of immunoglobulin (referred to as Ig) in plasma cells and induce proliferation of plasmablasts, leading to IL-10-mediated blockadeviainactivation of signal transducer and activator of transcription 3 (referred to as STAT3) and induction of paired box 5in vitro.MSCs can enhance the survival and proliferation rates of CD5+Bregs in an IDO-dependent manner, increasing IL-10 expression and ameliorating refractory, chronic GVHD[10].Similarly, AMSCs reduce plasmablast formation or induce IL-10-producing CD19+CD24highCD38highB cells[64].Parket al[65]elucidated the effect of human AMSCs on the proliferation of Bregs in an animal model of systemic lupus erythematosus.
MSC TRANSPLANTATION TO TREAT CHEMICALLY-INDUCED ALI
Viral infection remains the main cause of ALF in developing countries, whereas DILI is more common in developed countries[1].DILI accounts for 50% of ALF cases in the United States[66]and Europe, and the main drug responsible is acetaminophen[67].Several animal models induced by chemical substances have been used to study the mechanisms of ALF[3].Chemical substances, such as Con A, α-galactosylceramide (commonly known as α-GalCer) and carbon tetrachloride (CCl4), have been used in ALF animal models in which MSCs have been demonstrated to alleviate the symptoms of liver injury effectively; although, the mechanisms are complex and not fully understood (Table 1).
Volarevicet al[68-70]conducted several studies on the immunoregulation of MSCs in ALF induced by Con A.Their previous studies showed that Con A-induced ALF is an excellent murine model of immune-mediated liver injury.CD8+T cells, CD4+T cells, NK T (NKT) cells, NK cells, and macrophages are reportedly related to this model and can be transferred to injured liver sites and secrete many cytokines.Meanwhile, the authors confirmed the efficacy of AMSCs for ALF induced by Con A[71].Gazdicet al[72]researched the MSC-NKT cell interaction in Con A- and α-GalCer-induced murine models of ALF, and elucidated that MSCs protect hepatocytes from the cytotoxicity of liver NKT cells by attenuating their ability to produce inflammatory factors, such as TNF-α, IFN-γ and IL-4, in an iNOS- and IDO-dependent manner.In a recent study of α-GalCer-induced ALF, Itoet al[73]demonstrated that MSCs can increase IL-10 in Tregs, which in turn, attenuates the hepatotoxicity of liver NKT cells[9].
Milosavljevicet al[74]revealed another mechanism of MSC-NKT cell interaction, specifically that MSCs can attenuate CCl4-induced ALF by downregulating IL-17 in liver NKT cells.Their findings highlighted the reduction of liver NKT cell cytotoxicity and the critical importance of increased regulatory cells (Tregs and NK Tregs) in MSCmediated attenuation of ALF, indicating the importance of MSC-induced regulatory cells as a prospective cell-based ALF therapy.Liuet al[75]demonstrated through a highdimensional analysis that MSCs significantly ameliorated CCl4-induced ALF and regulated the immune system of the liver.In this model, MSCs regulated different immune cells in two phases.During the injury stage, MSCs reduced the numbers of Ly6ClowCD8+resident memory T cells (referred to as TRM) cells, conventional NK cells, and IgM+IgD+B cells but increased the quantity of immunosuppressive monocytederived macrophages.During the recovery stage, MSCs enhanced the retention of Ly6ClowCD8+TRM cells and maintained the immunosuppressive ability of monocytederived macrophages.To reveal alterations in immune cell subsets of CCl4-induced ALF after MSC transplantation, the authors detected the metabolomic profile of the immune system.Using high-performance chemical isotope labeling liquid chromatography-mass spectrometry, they confirmed 256 metabolites as candidate biomarkers of the immune response in CCl4-induced ALF animal models, and 114 metabolites as candidate biomarkers of the immune response after MSCtransplantation.However, the potential immunomodulatory role of metabolites needs further investigation[76].MSCs have exhibited positive effects in a rat model of DGalN/LPS-induced ALF by inhibiting the recruitment and activity of neutrophils.Compared with monotherapy, combination of MSCs and anti-neutrophil serum can inhibit cell apoptosis more efficiently, ameliorate liver function, and reduce the mortality rate[77].In a mouse model of thioacetamide-induced ALF, both MSCs and MSC-conditioned medium treatment reduced the incidence of death.MSC-treated livers showed less hepatocellular apoptosis and more liver regeneration, as well as downregulation of macrophage infiltration and alteration of CD4+T cells to an antiinflammatory phenotype[78].
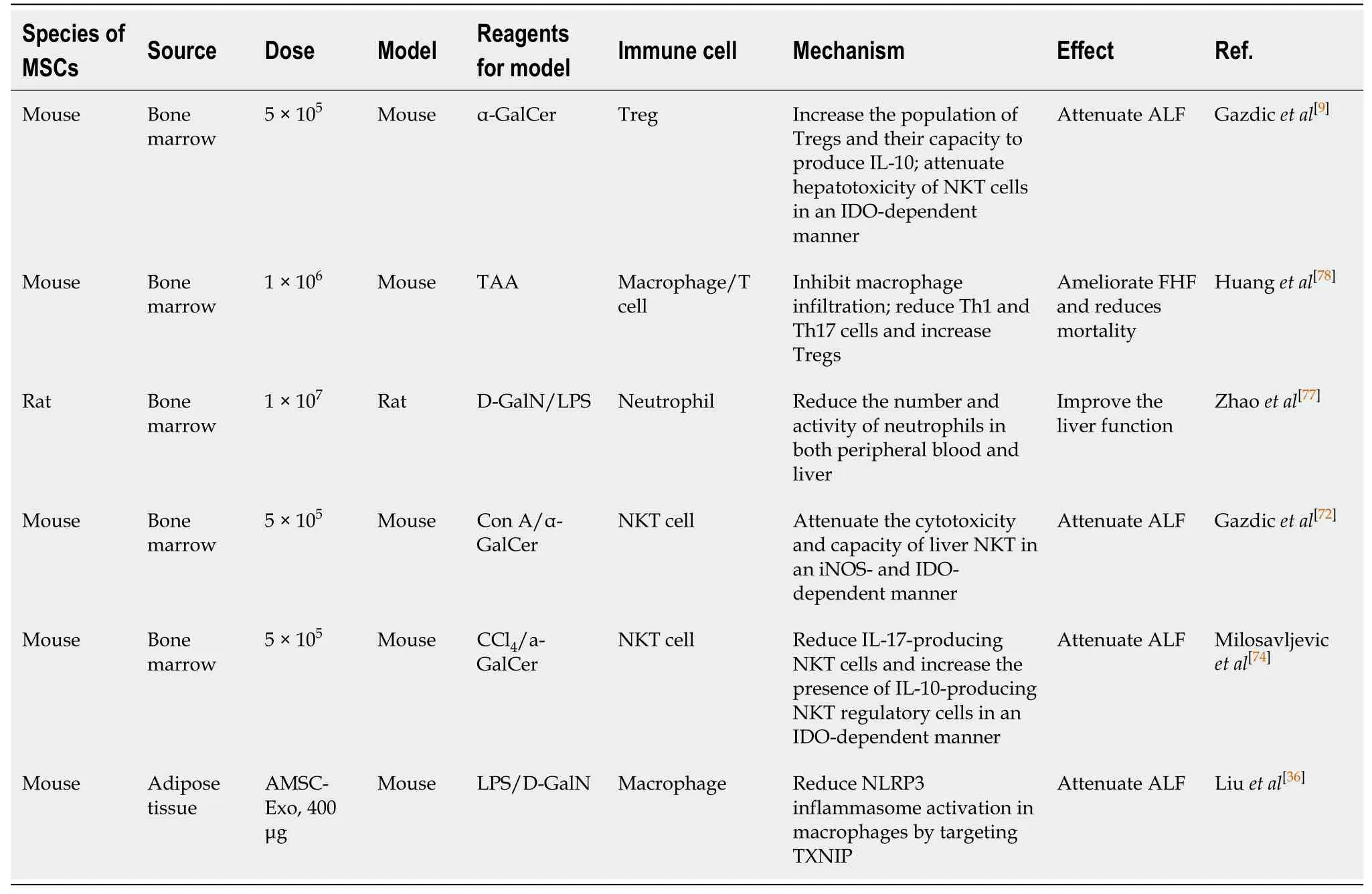
Table 1 Immunoregulatory mechanisms of mesenchymal stromal cells in alleviating chemically-induced acute liver failure
CONCLUSION
Increasing evidence has shown that MSCs have immunosuppressive capacities to regulate the function of immune cells in ALI as well as promote internal environmental homeostasis in chemically-induced ALF.MSCs can interact with both innate and adaptive immune systemsviacell-to-cell interactions and the paracrine pathway, coordinating an integrated response to liver injury and preventing hepatocyte necrosis.However, there are still some deficiencies in the research of MSCdependent immunoregulation in chemically-induced ALF.For example, the pathogenesis of liver injury models and the role of the immune system are still unclear.There has not been enough extensive and in-depth research on MSCdependent immunoregulation in chemically-induced ALF.
Different sources and different pretreated MSCs have varying therapeutic effects on liver injury.To date, there is no uniform standard for MSC applications in animal models[79].Thus, the results from different studies cannot be compared or repeated in different laboratories under different conditions[80].
MSCs have been widely studied for their differentiation and immunomodulation abilities.However, in one study, researchers focused on a single capability of MSCs, ignoring comparisons of their various capabilities.Future studies are needed to determine which MSC capability dominates.
There have been no clinical trials on DILI treated by MSCs.Clinical trials on MSC treatment are often applied to chronic diseases such as GVHD, diabetes, and malignant blood disease[81].MSCs are rarely used in DILI, which has a rapid onset and high mortality rate, and more conventional and conservative treatments tend to be used.Clinical trials can be conducted only if the efficacy and safety of MSCs are supported by sufficient research.The two main obstacles to translating the results from animal experiments into clinical practice are that the pathogenicity of ALI caused by clinical drugs differs from that of animal models[6], and that the immune system of animals, such as mice, is different from that of humans, so the results demonstrated in mice are not necessarily applicable to humans.Possible solutions to these issues are to verify the results obtained in animal experiments in organoids derived from human liver, and to identify animal models with similar pathogenicity to DILI in humans.Further studies are needed to reveal the therapeutic mechanisms of MSCs.
In conclusion, MSC transplantation can efficiently reduce the high mortality rate of chemically-induced ALF and may become a prospective therapy in clinical practice.More prospective randomized studies are needed to ensure the therapeutic effects of MSCs.
