“Six-and-twelve” score for outcome prediction of hepatocellular carcinoma following transarterial chemoembolization. In-depth analysis from a multicenter French cohort
2021-01-14XavierAdhouteGuillaumenarandaJeanLucRaoulJeanPierreBronowickiRodolpheAntyMarcBourlire
Xavier Adhoute, Guillaume Pénaranda, Jean-Luc Raoul, Jean-Pierre Bronowicki, Rodolphe Anty, Marc Bourlière
Xavier Adhoute, Marc Bourlière, Department of Gastroenterology and Hepatology, Hôpital Saint-Joseph, Marseille 13008, France
Guillaume Pénaranda, AlphaBio Laboratory, Marseille 13003, France
Jean-Luc Raoul, Department of Medical Oncology, Institut de Cancérologie de l'Ouest, Nantes 44805, France
Jean-Pierre Bronowicki, Department of Gastroenterology and Hepatology, Centre Hospitalo-Universitaire de, Nancy 54511, France
Rodolphe Anty, Department of Gastroenterology and Hepatology, Hôpital Universitaire de l’Archet, Nice 06200, France
Abstract The “six-and-twelve” (6&12) score is a new hepatocellular carcinoma (HCC) prognostic index designed for recommended transarterial chemoembolization (TACE) candidates. Quick and easy to use by the sum of tumor size (cm) and number, this model identifies three groups with different survival time (the sum is ≤ 6; or > 6 but ≤ 12; or > 12); a survival benefit with TACE can be expected for HCC patients with a score not exceeding twelve. Recently, Wang ZW et al showed that the “6&12” model was the best system correlated with radiological response after the first TACE. Thus, we wanted to assess its survival prediction ability as well as its prognostic value and compared it to other systems (Barcelona Clinic Liver Cancer, Hong Kong Liver Cancer (HKLC) staging, Albumin-Bilirubin grade, tumor nodularity, infiltrative nature of the tumor, alpha-fetoprotein, Child-Pugh class, and Performance Status score, Cancer of the Liver Italian Program, Model to Estimate Survival for HCC scores, up-to-seven criteria) different from Wang ZW et al study in a multicenter French cohort of HCC including only recommended TACE candidates retrospectively enrolled. As previously demonstrated, we show that the "6&12” score can classify survival within this French cohort, with a prognostic value comparable to that of other systems, except HKLC staging. More importantly, the “6&12” score simplicity and ability in patients’ stratification outperform other systems for a routine clinical practice.
Key words: Hepatocellular carcinoma; Transarterial chemoembolization; “Six-and-twelve” score; Prognosis; Albumin-Bilirubin grade; Tumor nodularity, infiltrative nature of the tumor, alpha-fetoprotein, Child-Pugh class, and performance status score
TO THE EDITOR
We have read with great interest the study by Wanget al[1]who assessed and compared different prognostic models for hepatocellular carcinoma (HCC) patients undergoing transarterial chemoembolization (TACE) treatment, especially the latest “six-and-twelve” (6&12) score[2]within a nationwide Chinese HCC cohort (n= 1107). Increased survival after TACE is correlated with radiological response[3,4]and this study shows that the “6&12” index is the best system correlated with radiological response after the first TACE. The study population was more heterogeneous than the population used to develop the score, including patients with slightly altered performance status (PS) and logically a model like the 3rd version of the hepatoma arterial-embolization prognostic score[5](which include liver function parameters) had a higher predictive value for survival. However, simplicity (using two cut-off values for risk stratification) and presumed reliability of the “6&12” score have convinced us to assess once again[6]the reproducibility and the predictive value of this new model in a multicenter French cohort of HCC patients including only recommended TACE candidates (n= 324) ie intermediate and early unresectable stages according to the treatment stage migration concept. We compared it to other systems different from Wanget al[1]’s study (Barcelona Clinic Liver cancer[7](BCLC) staging, Child-Pugh (CP) class, Albumin-Bilirubin[8](ALBI) grade, NIACE[9][tumor nodularity, infiltrative nature of the tumor, alpha-fetoprotein (AFP), CP class, and PS] score (Table 1)) using time-dependent area under receiver operating characteristic curve (AUROC) values and C-indices.
Patients were retrospectively enrolled over a six years period in two centers (Marseille, Nancy). Demographic and clinical characteristics of HCC patients are shown in Table 2. HCC patients were mostly male (85%), with a median of age of 68 years. Cirrhosis was present in 96% of cases, CP class A (77%), CP class B7 (23%). Underlying liver disease was mostly related to alcohol abuse (38%) or viral C hepatitis (40%). Patients were BCLC stage B (n= 179), BCLC stage A (n= 145). HCC were multinodular in 71% of cases and the median tumor diameter was 35 mm (25-50). The mean session number of conventional TACE was 2.7 ± 1.8.
After a median follow-up duration of 24.4 (15.0-36.8) mo, eighty one percent of patients died. Kaplan-Meier analyses showed significant differences in overall survival (OS) distributions across subgroups of BCLC staging, “6&12” (Figure 1) and NIACE scores within this cohort (P< 0.05) (Table 3). Liver function at baseline also had an impact on survival; median OS was significantly different according to the CP class[CP-A, 27 (25-31) mo; CP-B7, 21 (15-24) mo (P= 0.0003)], or ALBI grade [grade 1, 35 (25-43) mo; grade 2, 26 (22-28) mo; grade 3, 16 (12-24) mo (P= 0.0029)].
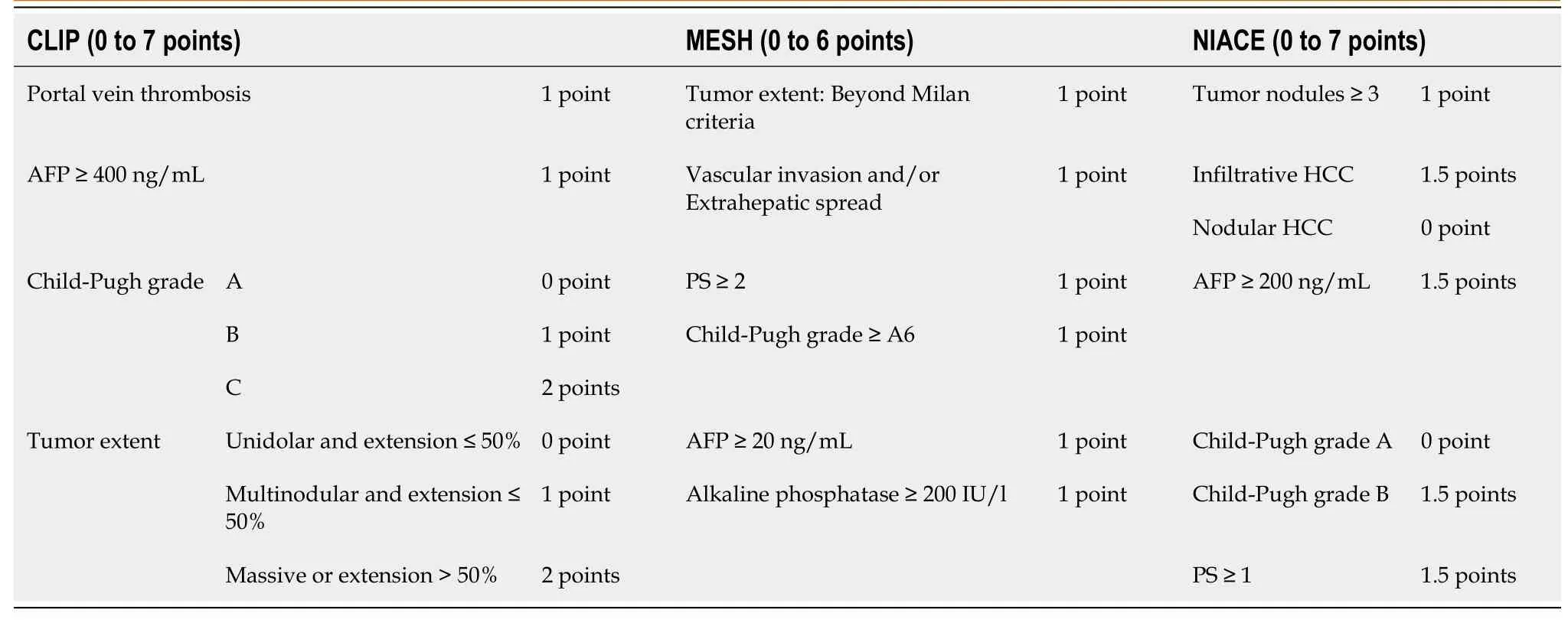
Table 1 Summary of points-based scores
Performances of the “6&12” score and other systems for survival prediction are indicated in Table 4. Time-dependent AUROC values and C-indices of the “6&12” score was not significantly different from those of other systems. We checked our results within the main cohort from Marseille (n= 252) (Table 2) by comparing the “6&12” score to other staging scoring systems (Hong Kong Liver Cancer[10](HKLC), Cancer of the Liver Italian Program[11](CLIP), Model to Estimate Survival for HCC[12](MESH), up-to-seven criteria[13]). Significant differences in survival distributions were also found across subgroups of the “6&12” score and other systems within this single center cohort (P< 0.05) (Table 5). Its predictive value remained comparable to that of other systems [C-index “6&12” 0.63 (0.56-0.70)vsCLIP 0.70 (0.62-0.78)vs“up-toseven” 0.61 (0.56-0.66)vsMESH 0.71 (0.63-0.78), not significant] except for HKLC staging, which provides a better prognostication ability [3-year AUROC (“6&12”) 0.56 (0.44-0.68)vs(HKLC) 0.69 (0.65-0.74),P= 0.0325] using a more complex stratification into five subgroups.
Firstly, our findings confirm previously published results[1,2], the “6&12” score can classify survival among recommended TACE candidates. Its prognostic performance was similar within our cohort compared to Wanget al[2]original study [3-year AUROC values: 0.64 (0.58-0.71)vs0.65 (0.61, 0.70); C-indices: 0.66 (0.58-0.74)vs0.66 (0.63, 0.69) (Table 4)], and higher than that observed in this nationwide Chinese cohort[1][c-index: 0.58 (0.56, 0.60)]. Moreover, HCC patients with the highest tumor burden [sum of largest tumor size (cm) and number exceeding 12] have a median survival of 15 mo similar to Wanget al[1]’s manuscript. Thus, this model can also identify within our population a subgroup of patients with poor prognosis who may not achieve benefit from TACE. The “6&12” risk stratification into three subgroups is relevant. Indeed, the first one (sum of tumor size and number not exceeding six) identifies TACE candidates with long-term survival especially those who may achieve a complete necrosis after this treatment[14,15]. Moreover, TACE is also an effective therapy for the second subgroup (sum of tumor size and number above six and not exceeding twelve), which has clear boundaries unlike intermediate stage subclassifications[16,17]that divide tumor burden according to the up-to-seven criteria (within/out).
Secondly, in our study the “6&12” score prognostic value is comparable to that of other systems, but most of these models cannot be used to guide treatment decision directly. “6&12” simplicity outweighs other systems for a current clinical practice including models with online calculator[5]. Indeed, therapeutic management is determined using a multidisciplinary approach and control of different published prognostic scores for TACE by clinicians (surgeons, oncologists, hepatologists and radiologists) is very unusual. By adding “the sum of largest tumor size and number”, it is true that consensus is easy to achieve among all clinicians. Moreover, other scores[9]encompass other baseline features that are likely to impact OS such as morphology of the tumor[18], but those parameters are not routinely recorded, whichlimits their use.

Table 2 Baseline characteristics of hepatocellular carcinoma patients undergoing transarterial chemoembolization treatment, n (%)
Thirdly, TACE should be limited to HCC patients with preserved liver function, and our results also highlight the importance of liver function in our population that included only recommended TACE candidates. Our patients are older, with more cirrhotic patients, and more alcohol-related diseases. This probably explains the differences in survival observed between this multicenter French cohort and Wanget al[2]original study, with OS ranging from 31.0 to 15.0 mo compared to 43.3 to 16.8 mo (according to “6&12” score), respectively. However, OS observed in our cohort was comparable to that of this nationwide Chinese cohort[1]including a more heterogeneous population with OS ranging from 31.3 to 18.5 mo.
Fourthly, Wanget al[19]findings on ABCR score are not surprising. This model designed for further TACE combines four parameters (AFP serum level, BCLC stage, change in Child-Pugh grade, and radiological tumor Response), but unlike ART[20,21](assessment for re-treatment with TACE) model the highest coefficient is assigned toradiological tumor response.

Table 3 Kaplan-Meier survival analysis according to “Six-and-twelve” score and other systems in the multicenter French cohort (n = 324)

Table 4 Comparison of predictive accuracy for overall survival between “Six-and-Twelve” score and staging/scoring systems (multicenter French cohort n = 324)
In summary, in this multicenter French HCC cohort different staging/scoring systems classify survival among recommended TACE candidates with a similar predictive power. However, “6&12” score simplicity and ability in patients’ stratification outperform other systems for a routine clinical practice.

Table 5 Kaplan-Meier survival analysis according to “Six-and-twelve” score and other systems in the main cohort from Marseille (available data for 241 hepatocellular carcinoma patients)

Figure 1 Kaplan-Meier analysis of overall survival according to “Six-and-twelve” criteria in the multicenter French HCC cohort (n = 324).
杂志排行
World Journal of Hepatology的其它文章
- Mechanisms and consequences of COVID-19 associated liver injury:What can we affirm?
- Review: Pathogenesis of cholestatic liver diseases
- Lipidomics in non-alcoholic fatty liver disease
- Update on diagnosis and management of sepsis in cirrhosis: Current advances
- Cell competition in liver carcinogenesis
- Management of hepatitis C in children and adolescents during COVID-19 pandemic