Effect of Shaolin internal qigong exercise on the surface electromyography signals of shoulder muscle groups in patients with capsulitis of the shoulder
2020-12-24WanBijiang万碧江LiMengmeng李萌萌XiaoQian肖倩HuangWei黄伟TangHongtu唐宏图HuZhaoduan胡昭端
Wan Bi-jiang (万碧江),Li Meng-meng (李萌萌),Xiao Qian (肖倩),Huang Wei(黄伟),2,Tang Hong-tu (唐宏图),Hu Zhao-duan (胡昭端)
1 College of Acupuncture and Orthopedics,Hubei University of Chinese Medicine,Wuhan 430061,China
2 Acupuncture-moxibustion Department,Hubei Provincial Hospital of Traditional Chinese Medicine, Wuhan 430061,China
Abstract
Keywords:Acupuncture Therapy;Electroacupuncture;Qigong;Shaolin Internal Qigong;Physical and Breathing Exercises;Shoulder Pain; Bursitis;Electromyography
Capsulitis of the shoulder (CS) is a chronic aseptic inflammation caused by degeneration of shoulder joint capsule and its surrounding soft tissues.It attacks a comparatively wide scope and manifests as persistent shoulder pain in the early stage,which then gets deteriorated gradually,coupled with adhesive and contractual soft tissues and limited positive and passive motions in various directions, finally presenting topical amyotrophy[1]. CS is usually treated through releasing pain, improving motor function and elevating muscle strength[2]. As a part of the precious cultural heritage of China, Shaolin internal qigong is a static qigong exercise that can strengthen the body resistance to eliminate pathogenic factors and benefit both external and internal.With isometric contractions to maintain postures and movements,together with the forced static contraction of the antagonistic muscles, Shaolin internal qigong can effectively increase the muscle strength and endurance[3-4], which is in line with the principle in the treatment of CS. In this trial, sixty CS patients were recruited to observe the changes in the surface electromyography (sEMG)of glenohumeral muscle groups after practice of Shaolin internal qigong or electroacupuncture (EA) treatment, so as to provide clinical reference for the treatment of CS with Shaolin internal qigong exercise and its efficacy evaluation.
1 Clinical Materials
1.1 Diagnostic criteria
According to the diagnostic criteria for CS in theCriteria of Diagnosis and Therapeutic Effects of Diseases and Syndromes in Traditional Chinese Medicine[5]:people aged around 50 years are at a high risk, women are more likely to develop this condition, and the right shoulder is more commonly affected; significant pain in the affected shoulder, usually in absence of swelling,worse at night, which may interfere with sleep; limited range of motion of the shoulder, especially when lifting,abducting, backward extending, and internally rotating,and the shoulder usually remains lifted, even coupled with amyotrophy in the topical area; tenderness in the shoulder, especially in the acromion, coracoid process and intertubercular sulcus,accompanied by stressed muscles; commonly, there is a history of chronic strain or contraction of wind-cold;mostly,the X-ray examination reports normal, though osteoporosis may be found in long-duration cases;shoulder pain or limited range of motion generated from trauma, tumor or neurological system and mental factors should be excluded.
1.2 Inclusion criteria
Conformed to the above diagnostic criteria, only one side was affected; aged 45-70 years old; not using any treatment that may affect the efficacy evaluation in the recent 1 month;in the adhesive stage;signed the informed consent form and willing to receive the treatment protocol in this trial.
1.3 Exclusion criteria
Unable to cooperate or complete the treatment;severe cerebro-cardiovascular or hematopoietic diseases;mental disorders;suspicious or confirmed with skin infection, ulcers, fracture, bone tumor, bone metastasis or tuberculosis; severe osteoporosis.
1.4 Rejection criteria
Failed to revisit on time or those quitted halfway;those with poor compliance and unable to receive the treatment following the protocol.
1.5 Statistical methods
The SPSS version 20.0 was used for statistical analysis.The normally distributed measurement data were expressed as mean ± standard deviation (±s), with the intra-group comparisons tested by paired samplet-test and the between-group comparisons tested by independent samplet-test. The enumeration data were examined using Chi-square test.P<0.05 was considered statistically significant.
1.6 General data
A total of 60 CS patients were recruited from Guoyitang Clinic of Hubei University of Chinese Medicine between January 2018 and January 2019.According to the visiting sequence, the patients were divided into a qigong group and an EA group based on the random number table, with 30 cases in each group.There were no significant differences in the general data between the two groups (allP>0.05), suggesting the comparability (Table 1).
2 Intervention Methods
2.1 Qigong group
Patients in this group practiced Shaolin internal qigong exercise regularly.
Methods:The patient was required to use static muscle force all over the body, keep the lower limbs straight, hold the thighs tight, place the heels firmly on the ground, and tuck the toes slightly to grasp the earth,while gathering force through the shoulders,arms,elbows, wrists and fingers, abducting the thumbs and putting the other four fingers together to form a‘八’-like palm. The patient was also asked to keep the body straight and pull the stomach in, and open the chest. While exerting a static force all over the body, the patient should maintain breathing naturally and let the force reach the limbs and back. The movements mainly included:pushing eight horses forward(Figure 1),dragging nine oxen backward(Figure 2),phoenix extending wings (Figure 3),overlord lifting the ancient cooking vessel(Figure 4),holding the heaven with two hands (Figure 5),pushing the boat along with the current (Figure 6),embracing the moon(Figure 7),the immortal showing the way (Figure 8),supporting the tower with palms (Figure 9),wind swinging lotus leaves(Figure 10),phoenix worshipping the sun(Figure 11),pulling gold ring with single palm(Figure 12),moving the palms as overlapping tiles (Figure 13),black dragon drilling hole on the earth (Figure 14) and hungry tiger pouncing on its prey (Figure 15).The exercise was practiced based on the relevant description of Shaolin internalqigong in theExercise and Techniques of Tuina[6].Five to eight movements were chosen to practice each time.

Table 1.Comparison of the general data between the two groups

Figure 1.Pushing eight horses forward

Figure 2.Dragging nine oxen backward

Figure 3. Phoenix extending wings
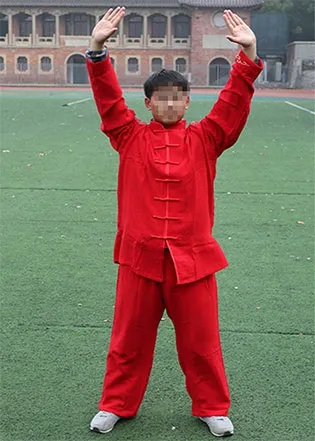
Figure 4.Overlord lifting the ancient cooking vessel

Figure 5. Holding the heaven with two hands

Figure 6.Pushing the boat along with the current

Figure 7. Embracing the moon

Figure 8.The immortal showing the way

Figure 9. Supporting the tower with palms

Figure 10. Wind swinging lotus leaves

Figure 11.Phoenix worshipping the sun

Figure 12. Pulling gold ring with single palm

Figure 13.Moving the palms as overlapping tiles

Figure 14.Black dragon drilling hole on the earth

Figure 15. Hungry tiger pouncing on its prey
Treatment course: One-hour practice each morning.The efficacy was evaluated after 1-month consecutive practice.
2.2 EA group
Patients in the group received EA treatment.
Acupoints: Jianyu (LI 15), Jianliao (TE 14), Jianzhen(SI 9), Jianqian(Extra), Ashi points and Yanglingquan(GB 34), as well as Tiaokou (ST 38) which was punctured towards Chengshan (BL 57).
Method: The acupoints were selected according to the treatment prescribed for Lou Jian Feng (shoulder exposed to wind) in theTherapeutics of Acupuncture and Moxibustion[7]and modified based on the patient’s own condition. Firstly, the patient took a sitting position or lied on the side. After routine sterilization, sterile acupuncture needles of 0.35 mm in diameter and 40 mm in length (Jiangsu Medical Equipment Approval No.:20162270588,Suzhou Acupuncture-moxibustion Appliance Co., Ltd., China) were used for treatment. The depth, angle and direction when inserting the needles all referred theScience of Meridians and Acupoints[8].The distant acupoint Tiaokou(ST 38)was initially inserted with the tip of the needle towards Chengshan(BL 57). When needling qi was achieved, the patient would be asked to move the affected shoulder joint.Treatment of the rest acupoints only started when there was a topical distending sensation or a sensation radiating towards the arm.After needling qi was obtained,the needle handles were connected to G6805-Ⅱ EA apparatus [Jianyu (LI 15) and Jianliao (TE 14) as a pair and Yanglingquan (GB 34) and Tiaokou (ST 38) as a pair], with sparse-dense wave, 2 Hz/100 Hz,and the stimulation should cause a tingling sensation or mild vibration of the muscles in the local areas but without pain. The needles were retained for 30 min each time.
Treatment course:The treatment was conducted once a day, with 6 consecutive sessions as a course at 1-day intervals.The efficacy was evaluated after 4 courses of treatment.
3 Observation of the Results
3.1 Observation items
Test of sEMG:According to the anatomical study of the location and function of the upper-limb motor muscles and the preliminary study of the effects of Shaolin internal qigong exercise on the sEMG of different muscle groups,we finally chose the biceps brachii,triceps brachii,deltoid,pectoralis major,latissimus dorsi and trapezius muscles for sEMG test.When the patient was in a proper position,the physician repeatedly swabbed the testing skin spotsand the surrounding areas with 75% alcohol to wipe off the oil stain and necrotic horny layer on the skin surface.The electrodes were adhered to the prominent muscle bellies.The recording electrode should be parallel to the muscle fibers and form up a regular triangle with the reference electrode,with 2-3 cm between the two electrodes[9].MyoMove-EOW sEMG apparatus(Shanghai Nuocheng Medical Appliance Co.,Ltd.,China)was adopted to detect the above six muscles,and each muscle was tested twice.The test was performed 1 d before and after practice of the exercise,respectively.During the test,the patient should keep relaxed.When the sEMGsignal was at baseline,the patient was asked to abduct the shoulder by 45°, flex the arm forward by 60° and internally rotate the shoulder when bend the elbow by 90°,to simultaneously collect the signals of the biceps brachii,triceps brachii,deltoid,pectoralis major,latissimus dorsi and trapezius muscles at the maximum isometric contraction.The data collection duration was only 1 s to prevent from fatigue.The patient was asked to relax again after data collection,for 5-7 s.Each movement wastested 6 times to take the average value[10-11].When the test finished,MATLB analysis software was used to processthe sEMG signals and calculate the corresponding integrated electromyography (iEMG)of each muscle.
3.2 Criteria for therapeutic efficacy
The treatment result was classified into 4 levels based on theGuiding Principles for Clinical Study of New Chinese Medicines[12].
Recovered: The pain in the affected shoulder was completely released and the shoulder joint motor function wascompletely restored.
Markedly effective:The pain in the affected shoulder was substantially released and the shoulder joint function was substantially restored.
Effective:The pain in the affected should was reduced and the shoulder joint motor dysfunction was partly improved.
Invalid: The symptomsremained unimproved.
3.3 Results
3.3.1 Comparison of the clinical efficacy
The total effective rate was 93.3%in the qigong group,versus 83.3% in the EA group,and the Chi-square test revealed a significant difference between the two groups(P<0.05),proving that Shaolin internal qigong exercise was effective for CS (Table 2).
3.3.2 Comparison of the iEMG at 45° abduction of the shoulder during maximal isometric contraction
The iEMG of the biceps brachii,triceps brachii,deltoid and pectoralis major muscles increased after treatment in the qigong group(allP<0.05),and the increase of the deltoid muscle was most significant(P<0.01),and the iEMG of the trapezius and latissimus dorsimuscles decreased after treatment(bothP<0.05),especially the iEMGof the trapezius (P<0.01).The iEMG of deltoid increased after treatment in the EA group(P<0.01),while there was no significant change in the iEMGof the other muscles(allP>0.05).After treatment,there was no significant difference in the iEMGof the deltoid muscle between the two groups(P>0.05),while significant differences were found in the iEMG of the rest muscles(allP<0.05),(Table 3 and Table 4).
3.3.3 Comparison of the iEMG at 60° flexion of the shoulder during maximal isometric contraction
The iEMG of the biceps brachii,triceps brachii,deltoid and pectoralis major muscles increased after treatment in the qigong group(allP<0.05),especially the iEMGof the biceps brachii muscle(P<0.01),and the iEMG of the trapezius and latissimus dorsi muscles decreased after treatment (bothP<0.05).The iEMGof the biceps brachii and pectoralis major muscles increased after treatment in the EA group (bothP<0.05),while the changes in the iEMG of the other muscles were statistically insignificant (allP>0.05).After treatment, the iEMG values of the biceps brachii and pectoralis major were lower in the EA group than in the qigong group(P<0.05),while the between-group differences in the iEMG of the other muscles were statistically insignificant(allP>0.05),(Table 5 and Table 6).

Table 2.Comparison of the clinical efficacy between thetwo groups (case)
Table 3.Comparison of the iEMG of the upper-limb muscles at 45°abduction of the shoulder during maximal isometric contraction ( ±s,μV·s)

Table 3.Comparison of the iEMG of the upper-limb muscles at 45°abduction of the shoulder during maximal isometric contraction ( ±s,μV·s)
Note:Compared with the same group before treatment,1) P<0.05,2) P<0.01
Group n Biceps brachii Triceps brachii Deltoid Pre-treatment Post-treatment Pre-treatment Post-treatment Pre-treatment Post-treatment Qigong 30 12.38±2.77 14.89±2.931)8.98±2.37 11.42±2.991) 17.16±4.32 27.35±4.422) EA 30 12.83±3.12 13.24±2.83 9.13±2.45 9.79±2.94 17.56±3.66 27.84±4.232) t-value-0.591 2.290 -0.948 2.128-3.870-0.432 P-value 0.557 0.026 0.347 0.038 0.700 0.668
Table 4.Comparison of the iEMG of the trunk muscles at 45ºabduction of the shoulder during maximal isometric contraction ( ±s,μV·s)

Table 4.Comparison of the iEMG of the trunk muscles at 45ºabduction of the shoulder during maximal isometric contraction ( ±s,μV·s)
Note:Compared with the same group before treatment,1) P<0.05,2) P<0.01
Group n Pectoralismajor Latissimusdorsi Trapezius Pre-treatment Post-treatment Pre-treatment Post-treatment Pre-treatment Post-treatment Qigong 30 13.99±3.29 17.06±3.211)18.43±2.64 16.22±2.711) 28.19±3.63 18.03±2.782)EA 30 14.15±2.86 15.14±3.10 18.38±3.21 17.91±2.85 27.73±3.71 26.54±3.56 t-value-0.202 2.312 0.149-2.357 0.478-10.693 P-value 0.841 0.024 0.941 0.022 0.635 0.000
Table 5.Comparison of the iEMG of the upper-limb muscles at 60ºflexion of the shoulder during maximal isometric contraction ( ±s,μV·s)

Table 5.Comparison of the iEMG of the upper-limb muscles at 60ºflexion of the shoulder during maximal isometric contraction ( ±s,μV·s)
Note:Compared with the same group before treatment,1) P<0.05,2) P<0.01
Group n Biceps brachii Triceps brachii Deltoid Pre-treatment Post-treatment Pre-treatment Post-treatment Pre-treatment Post-treatment Qigong 30 15.38±2.88 27.74±3.072)6.29±1.77 8.49±2.511) 12.45±3.79 16.20±3.651)EA 30 15.31±2.91 18.10±3.181)7.27±2.58 7.13±1.95 12.99±4.51 13.90±3.83 t-value 0.093 11.529-1.659 2.364-2.573 2.302 P-value 0.926 0.000 0.103 0.022 0.013 0.025
Table 6.Comparison of the iEMG of the trunk muscles at 60ºflexion of the shoulder during maximal isometric contraction( ±s,μV·s)

Table 6.Comparison of the iEMG of the trunk muscles at 60ºflexion of the shoulder during maximal isometric contraction( ±s,μV·s)
Note:Compared with the same group before treatment,1) P<0.05,2) P<0.01
Group n Pectoralis major Latissimusdorsi Trapezius Pre-treatment Post-treatment Pre-treatment Post-treatment Pre-treatment Post-treatment Qigong 30 13.50±3.75 16.27±3.161)14.38±2.81 12.31±3.241) 16.14±3.45 12.79±2.761)EA 30 13.67±4.01 15.11±4.001)13.94±2.96 13.92±2.51 16.38±4.00 14.72±3.36 t-value -0.166 2.272 2.558-2.081-0.244-2.346 P-value 0.868 0.027 0.013 0.042 0.808 0.023
3.3.4 Comparison of the iEMG at 90° internal rotation of the shoulder with elbow flexed during maximal isometric contraction
The iEMG of the biceps brachii,triceps brachii,deltoid,pectoralis major and latissimus dorsi muscles increased after treatment in the qigong group(allP<0.05), especially that of the biceps brachii, pectoralis major and latissimus dorsi(allP<0.01),and the iEMGof the trapezius muscle decreased after treatment (P<0.05).The iEMGof the biceps brachii and pectoralis major increased after treatment in the EA group (bothP<0.05),while the other muscles showed insignificant changes(allP>0.05).After treatment,there was a significant difference between the two groups in the iEMGof each muscle(allP<0.05),(Table 7 and Table 8).
Table 7.Comparison of the iEMG of the upper-limb muscles at 90º internal rotation of the shoulder with elbow flexed during maximal isometric contraction ( ±s,μV·s)

Table 7.Comparison of the iEMG of the upper-limb muscles at 90º internal rotation of the shoulder with elbow flexed during maximal isometric contraction ( ±s,μV·s)
Note:Compared with the same group before treatment,1) P<0.05,2) P<0.01
Group n Biceps brachii Triceps brachii Deltoid Pre-treatment Post-treatment Pre-treatment Post-treatment Pre-treatment Post-treatment Qigong 30 15.33±3.40 26.48±3.022) 10.19±2.15 12.19±2.541) 14.91±3.05 17.47±2.841) EA 30 16.54±2.91 18.67±3.131) 9.93±2.48 10.07±2.86 15.08±3.07 15.31±2.34 t-value-0.591 9.816 0.436 3.028-0.223 3.204 P-value 0.557 0.000 0.664 0.004 0.824 0.002
Table 8.Comparison of the iEMG of the trunk muscles at 90ºinternal rotation of the shoulder with elbow flexed during maximal isometric contraction ( ±s, μV·s)

Table 8.Comparison of the iEMG of the trunk muscles at 90ºinternal rotation of the shoulder with elbow flexed during maximal isometric contraction ( ±s, μV·s)
Note:Compared with the same group before treatment,1) P<0.05,2) P<0.01
Group n Pectoralis major Latissimus dorsi Trapezius Pre-treatment Post-treatment Pre-treatment Post-treatment Pre-treatment Post-treatment Qigong 30 16.01±3.78 28.32±4.162)16.55±3.04 26.85±3.822)19.00±3.40 15.16±2.501) EA 30 17.31±3.45 19.22±3.501)15.98±3.91 17.01±3.63 18.41±3.85 17.10±3.33 t-value -1.404 9.166 0.634 10.222 0.625-2.547 P-value 0.165 0.000 0.528 0.000 0.535 0.014
The results showed that Shaolin internal qigong practice effectively increased the iEMG of the biceps brachii,triceps brachii,pectoralis major and deltoid at 45°abduction,60°flexion and 90°internal rotation of the shoulder in CS patients, suggesting that this exercise can elevate the force of both agonists and antagonists and improve the stability during the movement of shoulder joint.Moreover,the iEMGof the trapeziusand latissimus dorsi dropped after practice of Shaolin internal qigong exercise,demonstrating that this exercise can relax these muscles and improve the coordination during movements.In the EA group,the iEMGof the bicepsbrachii,pectoralismajor and deltoid muscles increased while that of the triceps brachii,trapezius and latissimus dorsi showed no significant changes after treatment,indicating that EA can effectively increase the force of the agonistsbut not the antagonists.Therefore,Shaolin internal qigong exercise had certain advantages in improving the motor stability and coordination compared with EA treatment.
4 Discussion
In traditional Chinese medicine(TCM),CS is also named‘Wu Shi Jian’(shoulder of the fifty),‘Lou Jian Feng’(shoulder exposed to wind),‘Jian Ning Zheng’(curdled shoulder)or ‘Dong Jie Jian’(frozen shoulder).It is an aseptic inflammation attacking the soft tissues around the shoulder joint,majorly presenting with peri-shoulder pain,tenderness,limited motion and amyotrophy.Some cases may have some systemic conditions such as dysphoria,insomnia and palpitation.It severely interferes with the quality of life and psychosomatic health of the patients[13].The existing treatments for CS majorly are oral non-steroidal anti-inflammatory drugs(NSAIDs),oral and external Chinese medication,acupuncture and moxibustion therapy, cupping, scraping,massage,local or pain spot block therapy,physical factor therapy,arthrolysis,surgery and functional exercise[14-16].As one of the basic treatment options,functional exercise can strengthen the body,boost the body resistance to eliminate pathogenic factors,activate blood flow to get rid of stagnation,reduce swelling and cease pain,nourish the tendons and meridians,mitigate amyotrophy and adhesion to correct the body posture and coordinate motions,so as to play an important role in the rehabilitation of CS.In recent years,functional exercise has been putting on more and more emphasis.A part of the patientsdid achieve fullrecovery through functional exercise alone[17-18].
Shaolin internalqigong exercise isa traditionalqigong exercise that can both regulate the internal Zang-fu organs and nourish the spirit,qi and mind,and strengthen the tendons and bones and improve the body constitution.It requires the body to maintain a certain tension while relaxed,so that the muscles, joints and tendons will keep stretching for a certain period of time, which can help reduce pain.Practicing in this way can prevent from injury or tear of the muscles or tendons resulting from abrupt force stretching the soft tissues around the shoulder joint,and thus is more beneficial to the recovery[19-20].Through practicing this type of exercise,the antagonists can improve its muscle force by compulsory static contraction,the muscle groups around the shoulder joint get more activated,and the adhesion-caused limited joint motion gets improved,so that,the topical blood circulation is boosted,the inflammation is reduced and the shoulder joint function is restored.
Literature research has found that in the treatment of CS,the efficacy is mostly evaluated using scales,including those for efficacy or pain grading and shoulder joint function estimation[e.g.range of motion,activities of daily living,shoulder joint function evaluation scale,and Constant Murley shoulder assessment score,which lack accurate quantitative assessment[21-22].By recording the bioelectrical signals during the activities of nerves and muscles via applying electrodes to skeletal muscles,sEMG conducts a quantitative analysis of the muscle function and strength status.It is easy-to-operate,safe and noninvasive and relatively reliable[23].It can record and analyze the electromyographical signals when the muscle group is doing the maximum isometric contraction.This technique has been extensively used to evaluate the muscle function and force[24].Asa major parameter in sEMG analysis,iEMG reflects the total discharge of the motor units participating in the movement at a certain time and can be used to measure the changes in the muscle strength[25].Research showed that the iEMGwas positively related to the muscle strength and tension during voluntary static contraction[26].
The current study demonstrated increased iEMG in the biceps brachii,triceps brachii,pectoralis major and deltoid muscles in CS patients after regular practice of Shaolin internal qigong (allP<0.05),suggesting that the activation of these muscles were boosted.Meanwhile,the iEMG in trapezius and latissimus dorsi muscles declined after practice(bothP<0.05),indicating a decreased electrical activity, which may be associated with the motor compensation during the development of CS.Some scholors found that scapular movement will replace the function of the glenohumeral joint duing the CS development,which activates the compensatory movement of trapezius and latissimus dorsi muscles[27].After practicing Shaolin internal qigong exercise,the CS patients showed decreased compensatory movement of trapezius and latissimus dorsi muscles in this study,suggesting improved coordination in joint movement and a better condition.The results revealed:regularly practicing Shaolin internal qigong exercise was effective for CS,as it can effectively increase the activation intensity of the biceps brachii,triceps brachii,pectoralis major and deltoid muscles and reduce the compensation of the latissimus dorsiand trapezius muscles,and subsequently increase the coordination and steady consistency in shoulder joint movements;meanwhile,sEMGcan be taken as an objective quantitative measure to estimate the efficacy in treating CS.
Conflict of Interest
The authors declare that there is no conflict of interest.
Acknowledgments
This work was supported by Scientific Research Project of China Association of Medical Qigong (中国医学气功学会科研项目, No. YXQG-MS-2017001).
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received:8 November 2019/Accepted:18 February 2020
猜你喜欢
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- Clinical observation on electroacupuncture plus long-snake moxibustion for rheumatoid arthritis due to kidney deficiency and cold coagulation
- Observation on therapeutic efficacy of heat-sensitive moxibustion plus Western medicine for diabetic peripheral neuropathy
- Clinical observation on acupoint sticking therapy plus electroacupuncture for treating peripheral facial paralysis
- Clinical observation on acupoint massage plus Vitalstim electrical stimulation for deglutition disorder after stroke
- Effects of intradermal needle therapy plus pinaverium bromide on gastrointestinal hormone levels in irritable bowel syndrome-diarrhea patients
- Research advances in the brain mechanisms of acupuncture effects based on the BOLD-fMRI technology