Clinical observation on acupoint sticking therapy plus electroacupuncture for treating peripheral facial paralysis
2020-12-24FengLimei冯丽梅ZengTingting曾婷婷HouWenguang侯文光ZhuYudan朱宇丹WangKang王康JiangFenghui姜凤慧YuanWenmin袁文敏ChenHui陈慧LuoJinchao骆劲超
Feng Li-mei (冯丽梅),Zeng Ting-ting (曾婷婷),Hou Wen-guang (侯文光),Zhu Yu-dan (朱宇丹), Wang Kang (王康),Jiang Feng-hui(姜凤慧), Yuan Wen-min (袁文敏),Chen Hui(陈慧),Luo Jin-chao(骆劲超)
1 Department of Acupuncture-moxibustion, Yiwu Traditional Chinese Medicine Hospital,Zhejiang Province, Yiwu 322000,China
2 Department of Acupuncture-moxibustion, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine,Shanghai University of Traditional Chinese Medicine,Shanghai200437,China
3 Department of Traditional Chinese Medicine, Niansanli Street Community Health Service Center of Yiwu,Zhejiang Province,Yiwu 322000,China
Abstract
Keywords: Acupuncture Therapy;Electroacupuncture; Acupoint Sticking Therapy; Facial Paralysis; Visual Analog Scale;Pain Measurement
Peripheral facial paralysis is a common disease in neurology department and is mainly characterized by the movement disability of facial expression muscles.The main symptoms include deviation of mouth corner,an incomplete closure of palpebral fissure, a shallow nasolabial groove,a stiff or uncoordinated facial expression and disappearance of the frontal lines. The retroauricular pain exists in a large group of patients,and some cases are accompanied by symptoms like tearing against wind,hypogeusia and auditory abnormality. Such disease will cause a grave impact on patients’ daily life and social functions, lowering quality of life[1-3].Up till now, the pathogenesis of peripheral facial paralysis remains unclear, which may attribute to virus infection and poor immunity.The treatments majorly include improving nerve functions and glucocorticoid,which may alleviate symptoms to a certain degree,but remain limited general effect[4].Traditional Chinese medicine (TCM) has a long history in treating this disease.The principle rules are strengthening and consolidating body resistance,promoting blood circulation and unblocking meridians,tonifying qi to dispel the wind[5].Electroacupuncture(EA) can improve micro-circulation around acupoints,and promote the recovery of facial nerve functions[6].Mian Tan Gao (facial paralysis paste) was derived from Qian Zheng San(symmetry correcting powder), which can disperse wind and phlegm,nourish blood and unblock meridians, as well as accelerate blood flow and remove stasis. We chose 96 patients with peripheral facial paralysis to observe the clinical efficacy of acupoint sticking therapy with Mian Tan Gao(facial paralysis paste)plus EA for treating peripheral facial paralysis and its influence on patients’House-Brackmann(H-B)facial nerve function grading scale.The report is now given as follows.
1 Clinical Materials
1.1 Diagnosis criteria
This was based on the TCM and Western medicine diagnostic criteria in theTherapeutics of Acupuncture and Moxibustion[7]and theNeurology[8].
1.2 Inclusion criteria
Conforming to the diagnostic criteria above;first onset and in the acute stage;unilateral onset; good compliance;understood the study protocol and informed consented voluntarily.
1.3 Exclusion criteria
With serious liver,heart,kidney,or lung diseases;facial paralysis caused by injury, central nerve diseases or otitis;with tumor or tuberculosis;with cerebrovascular diseases,serious diabetes,hematopoietic or immune diseases;with serious cognitive or mental disorders; sensitive to EA treatment;women during pregnancy or lactation.
1.4 Statistical methods
Data were processed using SPSS version 22.0 software. The average age, disease duration, score of House-Brackmann(H-B) facial nerve function grading scale, visual analog scale (VAS), facial disability index (FDI)-physical function(FDIP)and FDI-social function(FDIS), and clinical symptoms and signs conformed to normal distribution with equal variance,and thus expressed as mean ± standard deviation(±s). Thet-test used for intra-group comparison,one-way analysis of variance for between-group comparison, and least significant difference for multiple comparisons.Data of gender, affected side, adverse event percentage,and the total effective rate were expressed as case or percentage, and compared by Chi-square test. The test standard was set asα=0.05, andP<0.05 considered to be statistical significance.
1.5 General data
This research won approval from the Ethics Committee of Yiwu Traditional Chinese Medicine Hospital, Zhejiang Province (Ethics No.: sc-2017-04). A total of 96 patients with peripheral facial paralysis in Yiwu Traditional Chinese Medicine Hospital between May 2017 and May 2019 were included and numbered from 1 to 96. One random number represented one patient. Then, the numbers were sequenced by the size.Numbers 1-32 were distributed into the observation group, 33-64 to the medicine group, and 65-96 to the EA group. Between-group comparisons of the general data across the three groups showed no statistical significance(allP>0.05),indicating comparability (Table 1).

Table1.Comparison of the general data among thethreegroups
2 Treatment Methods
2.1 Medicine group
Patients in the medicine group received conventional medicine treatment.Mecobalamine[State Food and Drug Administration (SFDA) Approval No.: H20041767,Yabao Pharmaceutical Group Co.,Ltd., China] 0.5 mg each time, 3 times/d, oral administration; prednisone acetate(SFDA Approval No.:H37021900,Chenxin Pharmaceutical Group Co., Ltd., China), with an initial dose of 30 mg each time,once a day,oral administration, then adjusted according to the change of condition. The treatment lasted for 4 weeks.
2.2 EA group
Patients in the EA group received the same medicine treatment as those in the medicine group,but with additional EA treatment. EA treatment started from one week after the onset.
Major acupoints: Bilateral Hegu (LI 4), and Yingxiang(LI 20), Xiaguan (ST 7), Jiache (ST 6), Dicang (ST 4), Yifeng (TE 17), Tinggong (SI 19), Taiyang (EX-HN 5), Yangbai(GB 14) and Cuanzhu (BL 2) on the affected side.
Adjunct acupoints: Yuye (EX-HN 13) and Jinjin (EX-HN 12) were added for taste abnormity; Chengjiang (CV 24)for deviation of nasolabial groove; Shuigou (GV 26) for deviation of philtrum; and Yuyao (EX-HN 4) for weak eyebrow lift.
Methods:After routine sterilization, filiform needles(Suzhou Medical Supplies Factory Co.,Ltd., China) of 0.30 mm in diameter and 40 mm in length were penetrated into acupoints. After qi arrival, connected the G6805-ⅡEA apparatus(Jining Fengtai Medical Equipment Co., Ltd., China) for stimulation, selected an intermittent wave with a frequency of 1.2-1.7 Hz, with an intensity to induce a mild contraction of facial muscles and the patient can tolerate. The treatment lasted for 30 min each time, once a day, 5 times a week for a total of 4 weeks.
2.3 Observation group
Patients in the observation group received the same EA treatment as mentioned before, and then received acupoint sticking therapy with Mian Tan Gao(facial paralysis paste).
Major ingredients in Mian Tan Gao (facial paralysis paste):Bai Fu Zi(Rhizoma Typhonii Gigantei)600 g,Quan Xie(Scorpion)500 g,Jiang Can(Bombyx Batryticatus)1 000 g,Bai Zhu(Rhizoma Atractylodis Macrocephalae)600 g,Dang Gui(Radix Angelicae Sinensis)900 g,Chuan Xiong(Rhizoma Chuanxiong)1 000 g,Hong Hua(Flos Carthami) 800 g,Sheng Jiang(Rhizoma Zingiberis) 600 g,Niu Bang Zi(Fructus Arctii)500 g, rice wine 1 000 g,Gan Cao(Radix Glycyrrhizae Preparata) 1 000 g,Bing Pian(Borneolum Syntheticu)800 g.After weighed and cleaned,the herbs were ground into powder. After 60 ℃ vacuum drying for 3 h,added 400 g lanolin and 350 g vaseline into the powder,and heated the mixture with mild fire for 2-3 h into paste. Smeared the paste on the gauze to make plasters,1 000 pieces in total.
Methods:Applied one piece of Mian Tan Gao (facial paralysis paste)to the affected Yifeng (TE 17).The plaster should do no harm to the skin, but in case of allergy or blistering, the skin will recover soon after the removal of the plaster. The plaster retained for 5 h each time, once a day for 4 weeks.
3 Therapeutic Efficacy Observation
3.1 Observation items
3.1.1 Facial nerve functions condition
H-B facial nerve grading scale was used for evaluating facial nerve functions. H-B scale was gradedⅠ to Ⅵlevels and scored 1-6 points respectively,1 point indicating a normal facial nerve function, and 6 points indicating a totally paralyzed facial nerve function. A higher score indicated a more serious case[9].
3.1.2 Pain intensity
VAS was used for evaluating the retroauricular pain intensity. VAS ranged from 0 to 10, in which 0 indicated no pain and 10 indicated an unbearable pain. A lower score indicated a lower retroauricular pain intensity[10].3.1.3 Facial disability condition
FDI was used to evaluate facial disability status,including FDIP and FDIS, 10 items in total. FDIP included 5 items with 4 grades in each item, counted 2 to 5 points separately.A lower score indicated a worse physical function disorder. FDIS included 5 items with 6 grades in each items, counted 1 to 6 points. A lower score indicated a better social function[11].3.1.4 Clinical symptoms and signs severity
Graded the severity of the symptoms and signs including deviation of mouth corner,an incomplete closure of palpebral fissure, a shallow nasolabial groove,a stiff or uncoordinated facial expression and disappearance of the frontal lines.Each symptom was graded 4 degrees of no,light,mild and severe,scored 0,1,2 and 3 points correspondingly.A lower score indicated lighter symptomsand signs.
3.2 Therapeutic efficacy criteria[12]
Clinically cured:Disappearance of all facial symptoms and signs,and H-B grading was Ⅰ.
Markedly effective:Obvious alleviation of facial symptomsand signs,and H-Bgrading wasⅡ.
Effective: Certain alleviation of facial symptoms and signs,and H-B grading was Ⅲ.
Invalid:No alleviation of facial symptoms and signs,and H-Bgrading wasⅣto Ⅳ.
3.3 Results
3.3.1 Comparison of the therapeutic efficacy
After 4-week treatment,the total effective rate in the observation group wasmarkedly higher than that in the medicine group and the EA group,and the betweengroup comparisons showed statistical significance(bothP<0.05),(Table 2).
3.3.2 Comparison of the facial nerve functions and retroauricular pain severity
智慧课堂教学与应试教育不同,教师更注重学生在英语学习中获得的学习体验,学生大量使用手机学习平台进行移动智慧学习,整个教学过程做到以学生为主体,尤其突出了学生的自主学习作用,学生参与度高,学习质量较传统课堂有很大提升。移动技术教育新时代的大学英语教学改革必须构建以核心素养培养为目标的高职大学英语智慧教学模式。高职大学英语教学内容要依据核心素养来选择,在教学设计和教学评价方面要围绕语言能力、学习能力、思维品质和文化意识四个核心素养要素进行整合,保障核心素养培养目标的实现,激发学生的学习兴趣,提高学生的学习效率,提高教学质量,不断优化教学效果。■
Before treatment,the differences in the scoresof H-B grading and VAS showed no statistical significance across the three groups(P>0.05).After 4-week treatment,the scores of H-B grading and VAS in the three groups all dropped significantly (allP<0.05),and the scores in the observation group were notably lower than those in the medicine group and the EA group(allP<0.05).The differences in the scores of H-B grading and VAS between the medicine group and EA group showed no statistical significance(bothP>0.05),(Table 3).
3.3.3 Comparison of the facial disability condition
Before treatment,the difference in the FDI score showed no statistical significance across the three groups (P>0.05).After 4-week treatment,the FDIPscore in the three groupsallincreased significantly (allP<0.05),and the score in the observation group was notably higher than that in the medicine group and the EA group (bothP<0.05).The FDISscore in the three groups all dropped significantly (allP<0.05),and the score in the observation group was markedly lower than that in the medicine group and the EA group(bothP<0.05).The differences in the scores of FDIP and FDIS between the medicine group and the EA group showed no statisticalsignificance(bothP>0.05),(Table 4).
3.3.4 Comparison of the scores of clinical symptoms and signs
Before treatment,the differences in the scores of clinical symptoms and signs showed no statistical significance across the three groups (allP>0.05). After 4-week treatment, the scores of clinical symptoms and signs in the three groups all dropped significantly (allP<0.05), and the scores in the observation group were markedly lower than those in the medicine group and the EA group (allP<0.05). The differences in the scores of clinical symptoms and signs between the medicine group and the EA group showed no statistical significance (allP>0.05), (Table 5 and Table 6).
3.3.5 Comparison of the adverse events
During the treatment period, the differences in the adverse events showed no statistical significance across the three groups (P>0.05), (Table 7).

Table2.Comparison of the clinical efficacy among thethree groups(case)
Table3.Comparison of the facial nerve function and retroauricular pain among thethreegroups( ±s,point)
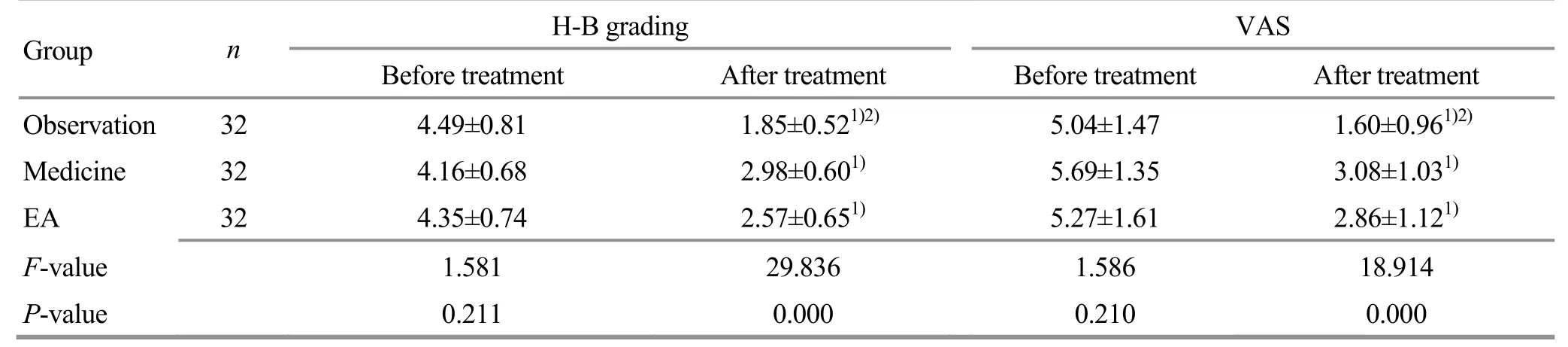
Table3.Comparison of the facial nerve function and retroauricular pain among thethreegroups( ±s,point)
Note:Intra-group comparison,1) P<0.05; compared with the medicine group and the EA group after treatment,2) P<0.05
Group n H-Bgrading ⅤAS Before treatment After treatment Before treatment After treatment Observation 32 4.49±0.81 1.85±0.521)2) 5.04±1.47 1.60±0.961)2) Medicine 32 4.16±0.68 2.98±0.601) 5.69±1.35 3.08±1.031) EA 32 4.35±0.74 2.57±0.651) 5.27±1.61 2.86±1.121) F-value 1.581 29.836 1.586 18.914 P-value 0.211 0.000 0.210 0.000
Table4.Comparison of the facial disability condition( ±s,point)
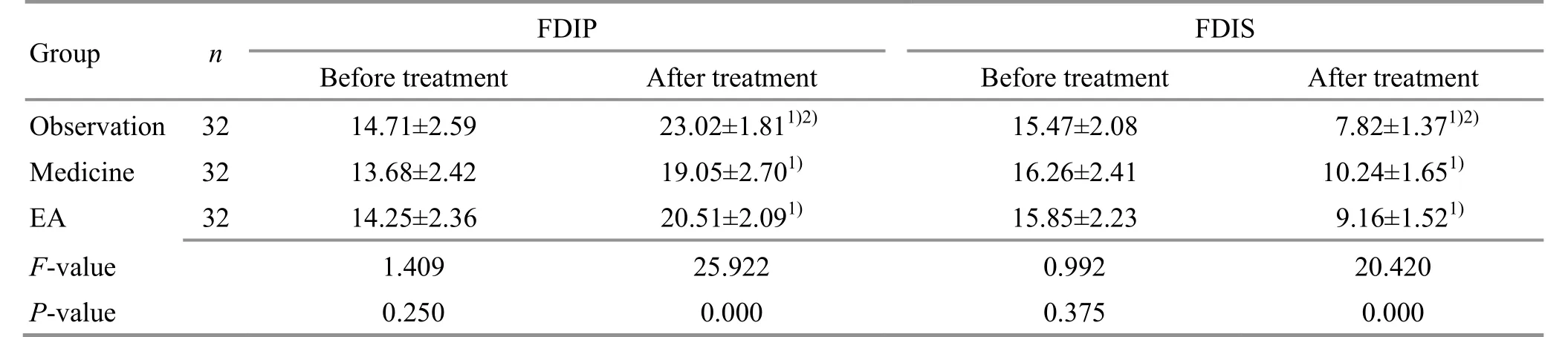
Table4.Comparison of the facial disability condition( ±s,point)
Note:Intra-group comparison,1) P<0.05; compared with the medicine group and the EA group after treatment,2) P<0.05
Group n FDIP FDIS Before treatment After treatment Beforetreatment After treatment Observation 32 14.71±2.59 23.02±1.811)2) 15.47±2.08 7.82±1.371)2) Medicine 32 13.68±2.42 19.05±2.701) 16.26±2.41 10.24±1.651) EA 32 14.25±2.36 20.51±2.091) 15.85±2.23 9.16±1.521) F-value 1.409 25.922 0.992 20.420 P-value 0.250 0.000 0.375 0.000
Table 5.Comparison of the scoresof deviation of mouth corner,incompleteclosure of palpebral fissure and shallow nasolabial groove ( ±s, point)
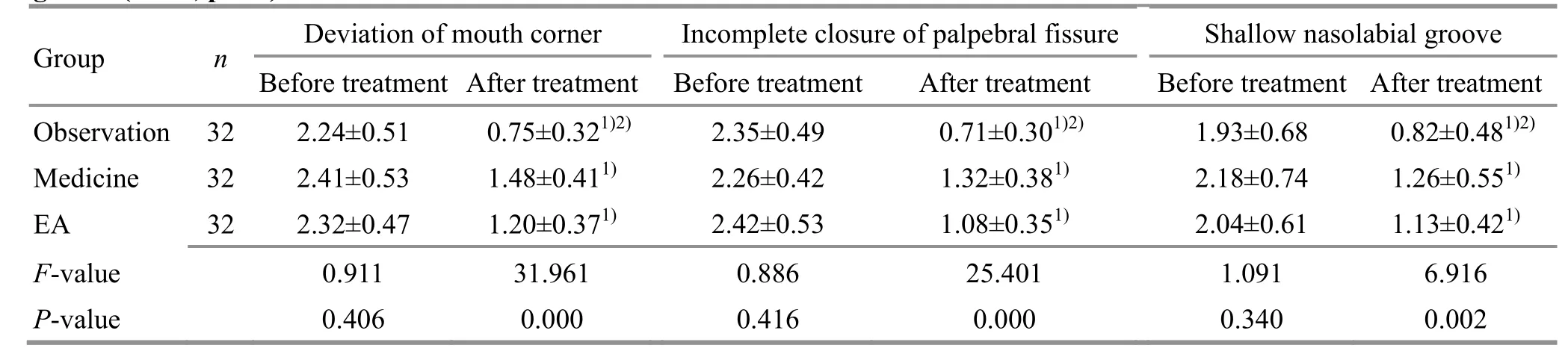
Table 5.Comparison of the scoresof deviation of mouth corner,incompleteclosure of palpebral fissure and shallow nasolabial groove ( ±s, point)
Note:Intra-group comparison,1) P<0.05;compared with the medicine group and the EA group after treatment, 2) P<0.05
Group n Deviation of mouth corner Incomplete closure of palpebral fissure Shallow nasolabial groove Before treatment After treatment Before treatment After treatment Before treatment After treatment Observation 32 2.24±0.51 0.75±0.321)2)2.35±0.49 0.71±0.301)2) 1.93±0.68 0.82±0.481)2) Medicine 32 2.41±0.53 1.48±0.411) 2.26±0.42 1.32±0.381) 2.18±0.74 1.26±0.551) EA 32 2.32±0.47 1.20±0.371) 2.42±0.53 1.08±0.351) 2.04±0.61 1.13±0.421) F-value 0.911 31.961 0.886 25.401 1.091 6.916 P-value 0.406 0.000 0.416 0.000 0.340 0.002
Table 6.Comparison of the scores of stiff or uncoordinated facial expression and disappearance of the frontal lines ( ±s, point)
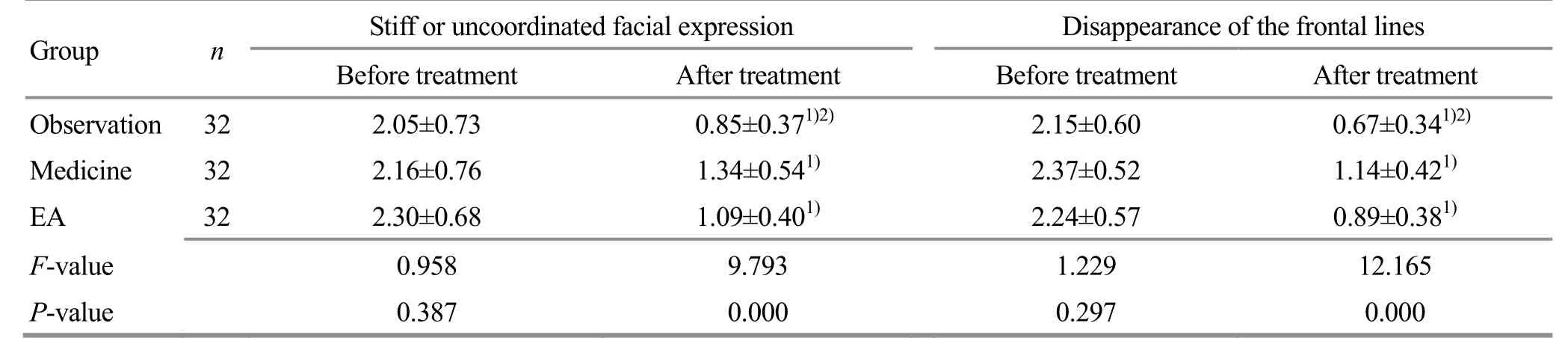
Table 6.Comparison of the scores of stiff or uncoordinated facial expression and disappearance of the frontal lines ( ±s, point)
Note:Intra-group comparison,1) P<0.05;compared with the medicine group and the EA group after treatment, 2) P<0.05
Group n Stiff or uncoordinated facial expression Disappearance of the frontal lines Before treatment After treatment Before treatment After treatment Observation 32 2.05±0.73 0.85±0.371)2) 2.15±0.60 0.67±0.341)2) Medicine 32 2.16±0.76 1.34±0.541) 2.37±0.52 1.14±0.421) EA 32 2.30±0.68 1.09±0.401) 2.24±0.57 0.89±0.381) F-value 0.958 9.793 1.229 12.165 P-value 0.387 0.000 0.297 0.000
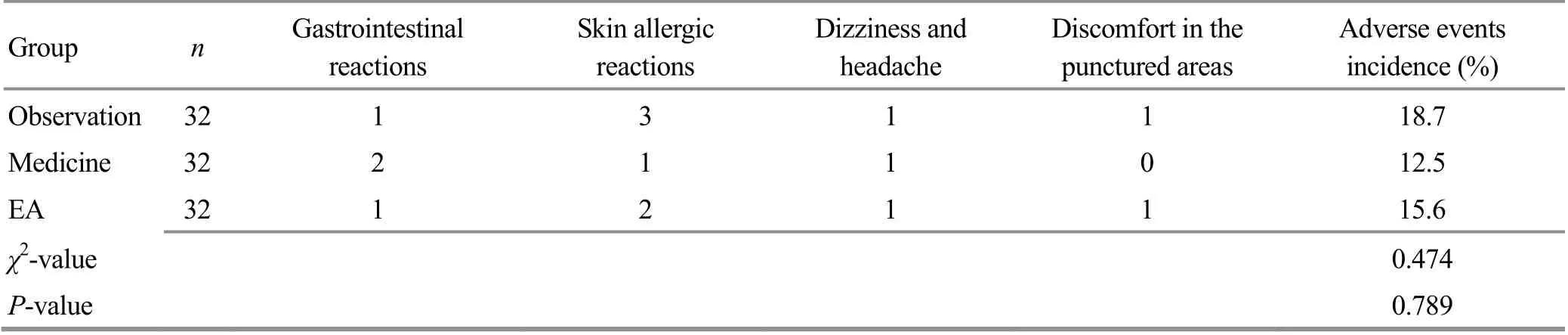
Table7.Comparison of the adverseeventsamong the three groups(case)
4 Discussion
Peripheral facial paralysis is a common disease more likely to happen in winter and spring. It may affect all age group. Although without life threatening danger,such disease affects facial appearance and causes grave mental burden to the patients[13-14]. Glucocorticoid and other routine Western medicine aiming to improve nerve functions have a limited therapeutic effect but may cause many adverse events[15].Acupuncture,acupoint sticking therapy or other TCM treatment methods have a satisfactory effect on peripheral facial paralysis, and are also known for the safety and low cost.
Recently,there has been increasing number of research conducted to investigate acupuncture combining herbal pastry for facial paralysis[19]. The main ingredients of Mian Tan Gao (facial paralysis paste),derived from Qian Zheng San(symmetry correcting powder,includedBai Fu Zi(Rhizoma Typhonii Gigantei),Quan Xie(Scorpion),Jiang Can(Bombyx Batryticatus),Bai Zhu(Rhizoma Atractylodis Macrocephalae),Dang Gui(Radix Angelicae Sinensis),Chuan Xiong(Rhizoma Chuanxiong),Hong Hua(Flos Carthami),Sheng Jiang(Rhizoma Zingiberis),Niu Bang Zi(Fructus Arctii),rice wine andGan Cao(Radix Glycyrrhizae Preparata).Bai Fu Zi(Rhizoma Typhonii Gigantei)can eliminate wind,dampness,and phlegm;Quan Xie(Scorpion)can unblock meridians and stop spasm by calming endogenouswind;Jiang Can(Bombyx Batryticatus)can remove phlegm and node,and calm wind and spasm;
Bai Zhu(Rhizoma Atractylodis Macrocephalae)can dry damp and reinforce spleen qi;Dang Gui(Radix Angelicae Sinensis)can stop pain,moisten dryness,accelerate and nourish blood;Chuan Xiong(Rhizoma Chuanxiong)can stop pain by facilitating qimovement;Hong Hua(Flos Carthami)can activate blood flow to remove stasis;Sheng Jiang(Rhizoma Zingiberis)can activate blood flow and disperse cold;Niu Bang Zi(Fructus Arctii)can reduce swelling and get rid of pathogenic wind-heat;rice wine can unblock meridians and activate blood flow;Gan Cao(Radix Glycyrrhizae Preparata) can mediate all herbs.The combination of the prescription has the function of nourishing and activating blood,removing stasis and unblocking meridians,and eliminating wind and phlegm.Modern research has showed thatBai Fu Zi(Rhizoma Typhonii Gigantei)can reduce inflammation and pain,downregulate blood vessel permeability and stabilize cell membrane.Quan Xie(Scorpion)isan anti-inflammatory drug and protector of the vascular endothelial cells.
Jiang Can(Bombyx Batryticatus)has the functions of anticoagulation,anticonvulsant and sedative.Bai Zhu(Rhizoma Atractylodis Macrocephalae)owns functions of anti-inflammation,adjusting immune system,and dilating vessels.Dang Gui(Radix Angelicae Sinensis)can adjust the immune system.Chuan Xiong(Rhizoma Chuanxiong)has functions of antiplatelet aggregation,antioxidant,dilating capillaries and protecting vascular endothelial cells.Hong Hua(Flos Carthami)has been used to resist inflammation.Gan Cao(Radix Glycyrrhizae Preparata)is usually used to eliminate inflammation and allergic reaction,and accelerate the discharge of toxin,and thus alleviate clinical symptoms[20-21].
This research showed that after 4-week treatment,the total effective rate of acupoint sticking therapy with Mian Tan Gao(facial paralysis paste)plus EA treatment was higher than that in the medicine group and the EA group, with better effects in improving the scoresof H-B grading,VAS and clinical symptomsand signs,while the comparisons between the medicine group and the EA group showed no statistical significance.Such results showed that acupoint sticking therapy with Mian Tan Gao (facial paralysis paste)plus EA had a certificated effect for peripheral facial paralysis,and the combination of two methods had a piling-up effect to get a quick recovery of facial nerve functions,and thus strengthen the clinical effect.Besides,after 4-week treatment,the FDIP score in the observation group ranked the highest, together with the lowest FDIS score,while the differences in the scores of FDIP and FDIS showed no statistical significance between the medicine group and the EA group,indicating that acupoint sticking therapy with Mian Tan Gao (facial paralysis paste)plus EA can not only improve the physical functions,but also improve other socialactivities.Lastly,after 4-week treatment,the comparison of the adverse events among the three groups showed no statistical significance,indicating a satisfactory safety in all three groups.
Above all,acupoint sticking therapy with Mian Tan Gao (facial paralysis paste)plus EA had a certificated effect for peripheral facial paralysis. It can improve the symptoms and signs,and ameliorate social functions,and thusworthy of clinicalpopularization.
Conflict of Interest
The authors declare that there is no potential conflict of interest in this article.
Acknowledgments
This work was supported by The Fourth Batch Research and Training Project for National Outstanding Talent of Traditional Chinese Medicine (Clinical or Basic) [第四批全国中医(临床、基础)优秀人才研修项目].
Statement of Informed Consent
Informed consent was obtained from all individual participants.
Received:15 January 2020/Accepted:13 March 2020
杂志排行

Journal of Acupuncture and Tuina Science的其它文章
- The role of microglia in thalamic reticular nucleus in acupuncture regulating cognitive deficits in insomnia rats
- Study on the acupoints belonging to the three yin meridians of foot reflecting the variation pattern of uterine qi and blood in women with moderate constitution
- Effects of electroacupuncture on uterine prostaglandin F2α, cyclooxygenase 2 and nuclear factor κB in rats with primary dysmenorrhea
- Effect of moxibustion at sensitized-acupoints on quality of life in patients with chronic superficial gastritis
- Research advances in the brain mechanisms of acupuncture effects based on the BOLD-fMRI technology
- Effects of intradermal needle therapy plus pinaverium bromide on gastrointestinal hormone levels in irritable bowel syndrome-diarrhea patients