Meteorological Influence on Tissue Expander-Related Major Infection
2020-12-22MinghaoZHAOHuiLIUChengGAN
Minghao ZHAO ,Hui LIU ,Cheng GAN
1 Plastic Surgery Hospital,Chinese Academy of Medical Sciences,No.33 Badachu Road,Beijing 100144,China
2 Medical Informatics Center,Peking University,No.38 Xueyuan Road,Beijing 100191,China
3 National Healthcare Data Center,Affiliated to National Center for Medical Service Administration,Beijing 100191,China
4 Ninth Department of Plastic Surgery,Plastic Surgery Hospital,Chinese Academy of Medical Sciences,No.33 Badachu Road,Beijing 100144,China
ABSTRACT Background Infection is a relevant complication of tissue expander surgery that may compromise the flap.The effects of meteorological variables on surgical site infection have been observed in many surgeries; however,their influence on tissue expander infection is unknown.Methods We identified tissue expander implantation and infection based on their International Classification of Diseases,10th revision,codes in electronic hospitalization summary reports of 26 cities from January 1,2014 to December 31,2015.The data of the present study were collected for administrative purposes without any personal identifiers.The Cox proportional hazard model was used to investigate the association between meteorological variables and tissue expander-related major infection with six covariates.Results A total of 3,089 patients were enrolled.Of them,8.7% experienced a major infection during the study period.The optimal daily average temperature was between 22.9 ° C and 26.8 ° C,and the risk of major infection was significantly decreased in this range.The minimal infection temperature was 24.4 ° C,with a hazard ratio of 0.85.When the average relative humidity was 37%,the infection risk was minimal with a hazard ratio of 0.86;however,a relative humidity of ≥ 79% significantly increased the risk of infection.Conclusions This is the first study to investigate the impact of temperature and relative humidity on tissue expander-related major infection.Our study suggests that there may be an optimal range of both temperature (22.9 ° C-26.8 ° C) and relative humidity (< 79%) that can lower the risk of major infection after tissue expander implantation.
KEY WORDS Tissue expander; Infection; Meterological influence; Data analysis
INTRODUCTION
Tissue expander implantation is a unique technique for patients with soft tissue defects.It is widely performed by plastic surgeons in a variety of surgical scenarios,including reconstruction for microtia,extensive scars,and deformity after tumor resection.Infection is an important complication,with rates varying from 3.2% to 9.3% in different patient groups[1-4].Infection may compromise the flap,cause expander extrusion,or promote local contracture[5].The known risk factors for tissue expander complications include age,body mass index,smoking[6],anatomic site[7],surgical experience[8],depression[9],and radiation exposure[10].
Epidemiologic studies have found that surgical site infection presents seasonal or weekly variations after different surgical procedures (general,gynecological,or spine surgery)[11,12].Patients undergoing surgery such as appendectomy in summer,and accordingly after warm days,experience more complications,especially superficial surgical site infections[13].Previous clinical studies have found that perioperative meteorological influence may account for this seasonal variation[13,14].
However,little is known about the association between tissue expander infection and meteorological variables.In this study,we examined electronic hospitalization summary reports from 26 cities with corresponding meteorological data from January 1,2014 to December 31,2015,to document the incidence of infection,to investigate the association between weather conditions and tissue expander infection,and to attempt to determine the range of meteorological variables with protective effects against infection.
PATIENTS AND METHODS
Data Source
Patient data were extracted from the hospitalization summary reports of the top-ranked public hospitals in care safety and quality,as evaluated by the National Hospital Performance Evaluation Project at the National Healthcare Data Center (see Supplemental Fig.1).Hospitalization summary reports contain information on basic demographics; admission and discharge dates;hospitalization and discharge diagnoses in Chinese and their corresponding International Classification of Diseases,10th Revision (ICD-10) codes; surgical operations and their corresponding ICD-9,Clinical Modification (ICD-9-CM) codes; and outcomes of hospitalization,including survival status,drug allergy,hospitalization infection,and financial cost.Each listed diagnosis is assigned to a variable that specifies the time it was made.The present study was exempted from the requirement for informed consent because the data used were collected for administrative purposes without any personal identifiers[15].
Information on temperature and relative humidity was extracted from the Chinese Meteorological Bureau,which provides data on daily 24-h temperature (°C) and relative humidity (%) monitored at meteorological observatories in each city.We considered the 7-day average temperature and relative humidity as variables that may affect tissue expander infection.
Inclusion and Exclusion Criteria
We retrospectively enrolled patients who underwent tissue expander implantation surgery for the first time (ICD-9-CM code:86.93).The primary outcome was major infection after the implantation procedure and before subsequent tissue expander removal or tissue expander replacement surgery (ICD-9-CM codes:85.96,86.05,and 97.89).Patients who did not undergo either tissue expander removal or tissue expander replacement surgery during the study period were excluded (January 1,2014 to December 31,2015).Some patients may have multiple hospital admissions for repeated major infections.To avoid the autocorrelation caused by this situation,we only included the first major infection and considered it as the endpoint.
Major Infection
The extent and severity of tissue expander infection differ among cases.Minor infections can be managed with oral antibiotics prescribed in the clinic and can resolve without other complications[3].Conversely,major infections can increase the length of stay in the hospital and confer a poor prognosis.In this study,we only included major infection as the study outcome,which was defined as tissue expander infection or surgical site infection that required readmission to the hospital for extensive care and treatment[2].The diagnosis of major infection was extracted using the ICD-10 code (T85.7)and the corresponding Chinese diagnosis of the admission diagnosis “tissue expander infection” or “surgical site infection”.We also calculated the readmission days as the time interval between the readmission date and the tissue expander implantation date.For patients with no major infection,the time needed to complete tissue expansion was defined as the readmission days; thus,this information was their censored event time.For patients with major infection,the time between expander implantation and major infection was used to calculate the readmission days (observed event time).
Cox Proportional Hazard Model
The covariates included age,sex,day of week,holiday,incision type,and diagnosis type.Age and sex could directly be extracted from the data source.Each procedure had corresponding incision types.An incision made on a scar is considered type II (clean-contaminated) in China.The diagnosis types were searched from the data source using the keywords of the ICD-10 diagnosis,and divided into three groups according to frequency.“Ear” referred to any ear defect including microtia.“Other” diagnoses included those observed at a less frequency in this study population,such as those requiring breast reconstruction,giant nevus resection,chronic wound repair,and reconstruction after tumor resection.
Most of the plastic surgery departments of the top-ranked hospitals in China do not have clinics and do not admit patients during holidays or weekends.Thus,we included“day of week” and “holiday” into the Cox proportional hazard model.
We also took into consideration the surgical incision type.
The Cox proportional hazard model was used with timedependent covariates in the following form:

where
ai(t) is the hazard function of major infection at expansion daytfor patienti.
a0(t) is the baseline hazard function of major infection at expansion dayt.
x1i(t) is the 7-day average temperature at expansion daytfor patienti.
x2i(t) is the 7-day average humidity at expansion daytfor patienti.
z1iis the indicator variable of age for patienti(“1” for 0-11 years,“2” for 11-17 years,“0” for 18-49 years,“3” for 50-65 years,and “4” for > 65 years).
z2iis the sex of patienti(“1” for male and “0” for female).
z3iis the indicator variable of the diagnosis type for patienti(“0” for ear,“1” for scar,and “2” for other).
z4iis the indicator variable of incision type for patienti(“0” for type Ⅰ (clean),“1” for type Ⅱ (cleancontaminated),“2” for type Ⅲ (contaminated),and“3” for other (infected or not available).
z5i(t) is the day of week at expansion dayt(“1” for weekend and “0” for other).
z6i(t) is the holiday status at expansion dayt(“1” for holiday and “0” for other).
ns(,3) is the distributed lag nonlinear model with 3 degrees of freedom in natural cubic splines.
All analyses were conducted using R programming language (version 3.2.2,R Development Core Team).All statistical tests were two-sided,andP<0.05 was considered statistically significant.
RESULTS
From January 1,2014 to September 31,2015,3,089 patients were enrolled.Of them,8.7% experienced a major infection during the study period.Among the major infections,77 (2.5%) occurred during hospitalization.Of 3,012 patients discharged without a diagnosis of infection,192 (6.4%) were readmitted to the hospital because of a major infection.
Clinical Characteristics and Meteorological Variables
The demographic and clinical characteristics of the patients are shown in Table 1.The mean age of the study population was 15.6 ± 11.3 years,and the mean age of the infected patients was 21.7 ± 15.5 years.Male patients comprised 60.2% of the study population,and the infection rate was not significantly different between men and women (51.7% vs.48.3%).The majority of diagnoses were ear defects (49.8%) and scars (38.8%),and all other diagnoses comprised the remaining 11.4%.The number of patients with major infection in each group was 154,74,and 41,respectively.The incision type of tissue expander implantation surgery was classified as Ⅰ (clean),Ⅱ (cleancontaminated),and Ⅲ (contaminated).The number of patients in each group was 1,995 (64.6%),858 (27.8%),and 41 (1.3%),respectively.The incision type of the remaining 195 (6.3%) patients was not available in the data source.The number of major infections in incision types Ⅰ,Ⅱ,Ⅲ,and not available was 142 (52.8%),94(34.9%),18 (6.7%),and 15 (5.6%),respectively.The average number of readmission days was 90.8.Of the patients with readmission,1,565 (50.7%) were readmitted at 31-90 days after tissue expander implantation and 1,331(43.1%) were readmitted after 91 days.The readmission days of patients with major infection was calculated as the time from tissue expander implantation to infection.A total of 121 (45.0%) cases of major infection occurred within 1 month after surgery,87 (32.3%) occurred within 31-90 days postoperatively,and 61 (22.7%) occurred 91days after expander implantation.
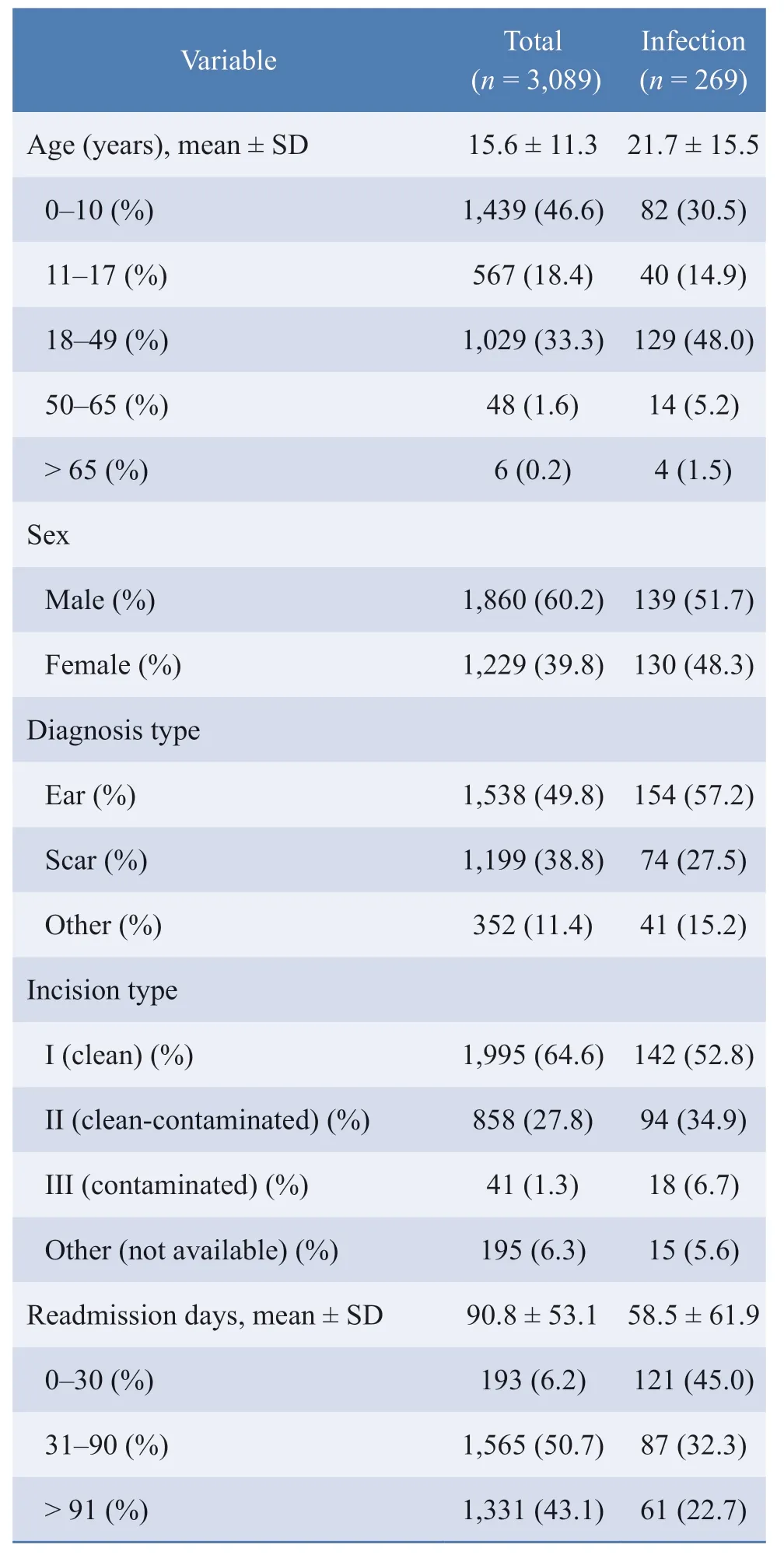
Table 1 Demographic characteristics of patients undergoing tissue expander implantation
The statistics of meteorological variables are listed in Table 2.During the observation,the maximum and minimum daily average temperatures were -25.7 ° C and 35.5 ° C,respectively.The minimum and maximum daily average relative humidity were 8% and 97%,respectively.As the supplemental map shows,this study involved 26 hospitals across China,and the diversity of geography and seasons resulted in large ranges of the meteorological variables.
Major Infection and Meteorological Variables
Table 3 shows the adjusted hazard ratios of infection in patients undergoing tissue expander implantation,from a Cox proportional hazard model.No significant differences among groups were observed in terms of age and sex.With respect to the diagnosis type,the scar and other groups showed a significantly higher risk than the ear defect group.The infection risk insignificantly increased as the incision became more contaminated.The significant hazard ratio of “day of week” and “holiday” was consistent with the hypothesis that plastic surgeons in China tend to not admit patients during holidays and weekends according to hospital policy and clinical convention.
As Fig.1 shows,the optimal daily average temperature was between 22.9 ° C and 26.8 ° C,and the risk of major infection significantly decreased in this range.The minimal infection temperature with a hazard ratio of 0.85 was 24.4 ° C.When the average relative humidity was 37%,the infection risk was minimal with a hazard ratio of 0.86,whereas a ≥ 79% relative humidity significantly increased the risk of infection.
DISCUSSION
To our knowledge,this is the first study to investigate the impact of temperature and relative humidity on tissue expander-related major infection.Our study suggeststhat there may be an optimal range of both temperature(22.9 ° C-26.8 ° C) and relative humidity (< 79%)that can lower the risk of major infection after tissue expander implantation.The hypothesis of this study was derived from other studies that documented seasonal variations in the incidence of complications in different surgeries such as spinal surgery,orthopedic surgery,and appendectomy[13,16-17].This seasonal variation can be explained by the difference in temperature and humidity in certain surgeries[13].
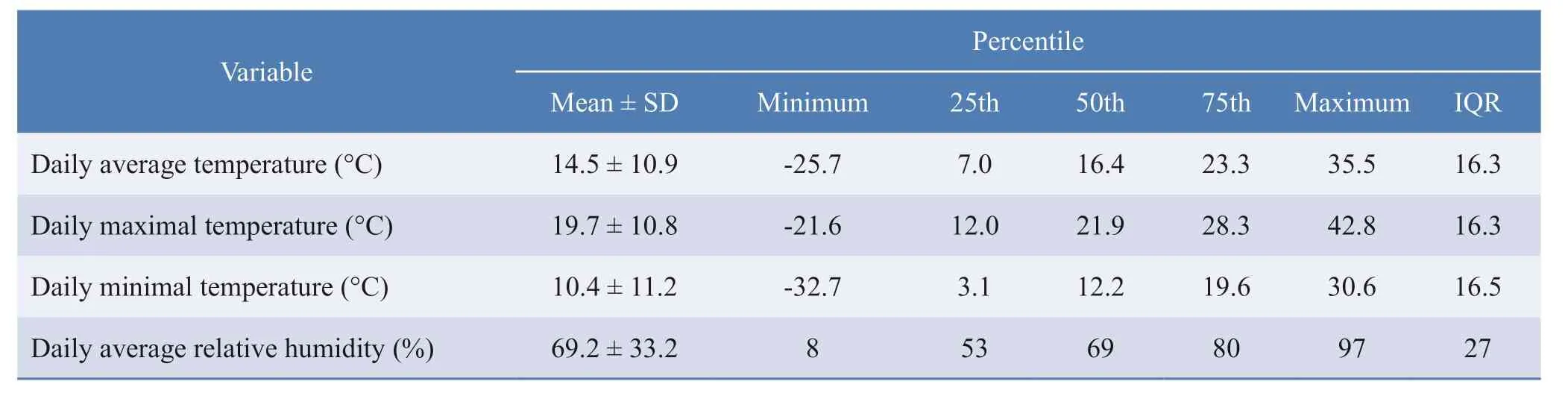
Table 2 Summary statistics of meteorological variables
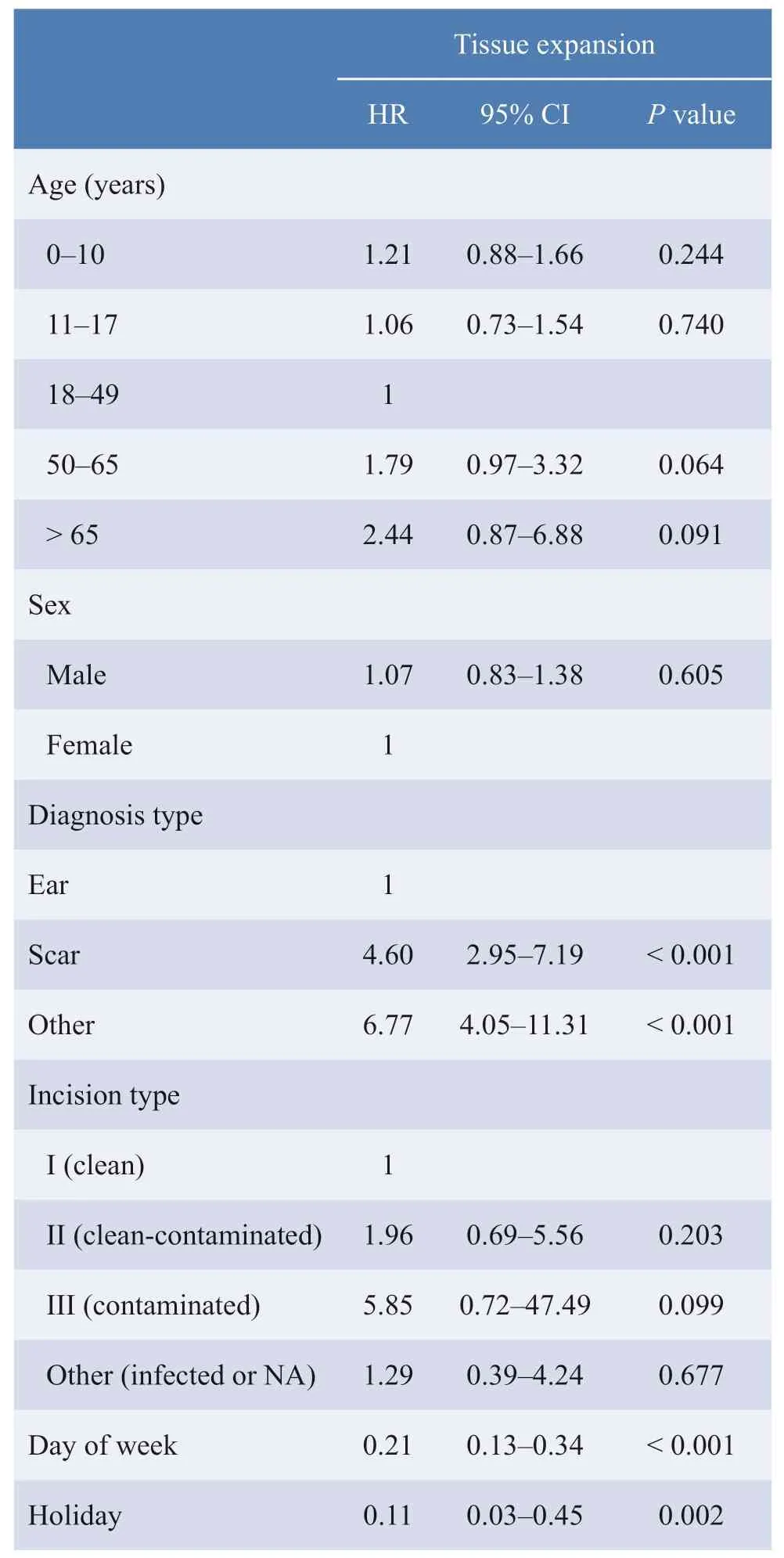
Table 3 Adjusted hazard ratios (HRs) of infection in patients undergoing tissue expansion from a Cox proportional hazard model with time-dependent temperature and humidity,adjusted for age,sex,day of week,holiday,incision type,and diagnosis type

Fig.1 Plot of the hazard ratio (95% confidence intervals in black dashed line) of infection over an average of 7 days (from lag1 to lag7),from a Cox proportional hazard model with time-dependent temperature and humidity,adjusted for age,sex,day of week,holiday,incision type,and diagnosis type
The pathogenesis of tissue expander infection involves the interaction of the host,the expander,and bacterial species.As the expansion requires repeated injections on the patient,the need for a puncture site wound may increase at each injection.
Previous studies have found that most tissue expander infections are caused by pathogenic bacteria from the skin flora,such asStaphylococcus aureus,Staphylococcus epidermidis,andPseudomonas aeruginosa[18].A study on the use of tissue expanders in breast reconstruction also foundS.aureusand Serratia marcescens as the main pathogenic strains[10].In normal circumstances,the human skin flora contains a variety of bacteria that do not cause an infection.However,after tissue expander implantation,the expander may impede local microcirculation,thus increasing the risk of infection.In animal models,subcutaneous foreign bodies significantly reduced the minimalS.aureusinoculum required to cause infection[19].
During the expansion process,puncture on the injection port is regularly performed.Extreme temperature and humidity may affect the major infection rate by breaking the weak balance between host immunity and skin flora after tissue expander implantation.
Numerous researchers have found that the perioperative temperature may affect wound healing[14,16,20-24].In tropical weathers,Staphylococcusspp.,Streptococcusspp.,and enteric bacteria tend to more readily colonize[25].Moreover,gram-negative bacteria on the skin are also reported to more readily colonize in high-temperature and high-humidity environments[26].It has also been found that high humidity weakens the stratum corneum and increases the friction of the skin,whereas dry skin has reduced flexibility and integrity between the epidermis and dermis,thus increasing the susceptibility of the skin to injury[27].
Furthermore,temperature and humidity can exacerbate existing asymptomatic infections.Researchers cultured silicone devices (mammary implants or tissue expanders)at the time of their removal from patients without clinical infection signs or symptoms,and found that 36% were positive for bacteria.The predominant isolate wasS.epidermidis[28].These bacteria grow on the implant surface as a biofilm,which is a dynamic threedimensional biological structure consisting of adherent microorganisms embedded in an extracellular matrix.It may cause persistent low-grade inflammation of the surrounding tissue,leading to capsular fibrosis and subsequent contracture[28-29].When extreme temperature and humidity enhance bacterial colonization,a symptomatic infection may become a major infection.
In this study,we discovered an association between meteorological variables and tissue expander-related major infection.On the basis of our observations,we suggest the optimal ranges of temperature (22.9 ° C-26.8 ° C) and humidity (< 79%) with a potential to lower the risk of infection.Ambient temperature and humidity in hospitals are usually not tightly managed in the ward and are often overlooked by health-care professionals.Temperature and humidity monitoring devices are usually not available in hospital departments outside of the operating theater.Moreover,patients spend most of the time outside the hospital during the expansion process.There are no specific doctors’ orders for patients on how to adjust to the weather.Considering that major infection can be both an emotional and an economic burden for patients,the value of simple interventions,such as regulating ambient temperature and humidity,should be tested in future studies.
This study had several limitations.This was a multicenter retrospective cohort study using a Cox proportional hazard model that adjusted for six covariates.However,as the data source provided only limited information,other known risk factors such as smoking and body mass index cannot be included in this model.Further,our source data do not provide clinical information such as strains of pathogenic bacteria,extent of infection,or the final outcomes of the reconstruction.In the future,prospective cohort studies examining more clinically relevant variables in detail should be performed.
Another limitation of this study was that our result presented a much wider confidence interval with respect to extreme weather.One possible explanation is that the sample size in extreme weather conditions was too small to yield a definite result (see Supplemental Fig.2).In addition,artificial cooling or warming devices used in extreme weathers can cause more variations.Therefore,two surrogate covariates were added to control the use of air conditioner and centralized heating systems during the follow-up period,and the results are shown in Supplemental Table 1.The comparison of the results in Table 3 and Supplemental Table 1 showed that these two covariates did not significantly affect the risk of major infection.In addition,the associations between the other six covariates and major infection were not changed by these two new covariates.However,to further clarify this issue,more accurate data on both bodily and environmental meteorological variables may be needed.Temperature and relative humidity can now be measured using small wireless devices,which are both suitable and convenient for use during exercise or sleep[30].Such tools can provide information to patients after tissue expander surgery concerning the microclimate of the expander,which can guide the maintenance of optimal skin moisture and temperature level.
In summary,this study showed a significant association between meteorological variables and tissue expanderrelated major infection,and that there may be an optimal range of both temperature (22.9 °C-26.8 °C) and relative humidity (< 79%) that can lower the risk of major infection after tissue expander implantation.
ETHICS DECLARATIONS
Ethics Approval and Consent to Participate
N/A
Consent for Publication
All the authors have consented for the publication.
Competing Interests
The authors declare that they have no competing interests.The authors state that the views expressed inthe submitted article are their own and not the official position of the institution or funder.
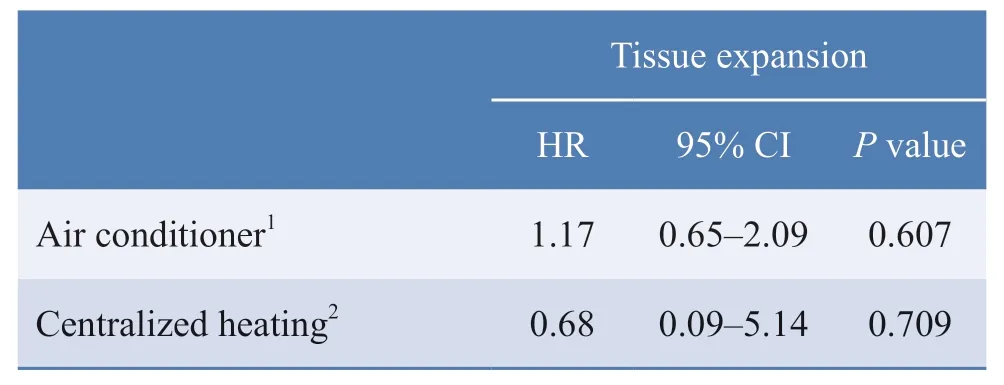
Supplemental Table 1 Adjusted hazard ratios (HRs) of infection in patients undergoing tissue expansion,from a Cox proportional hazard model with time-dependent temperature and humidity,adjusted for age,sex,day of week,holiday,incision type,diagnosis type,air conditioner,and centralized heating
SUPPLEMENTARY MATERIALS
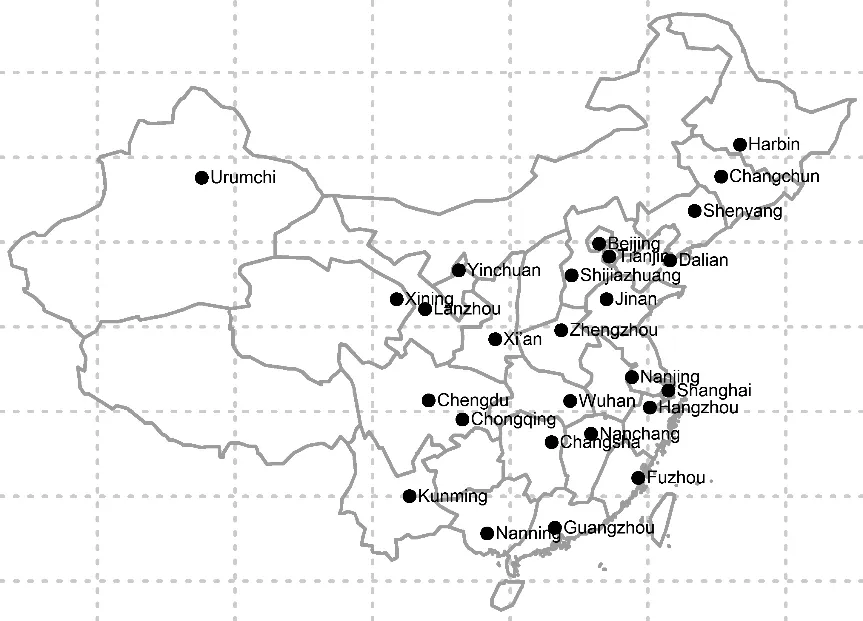
Supplemental Fig.1 Locations of the 26 Chinese cities in this study
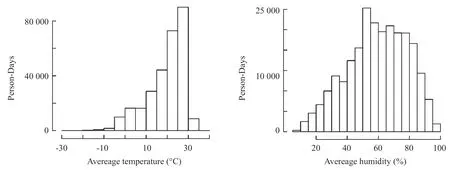
Supplemental Fig.2 Person-days of exposure to different meteorological conditions
杂志排行

Chinese Journal of Plastic and Reconstructive Surgery的其它文章
- Status Quo and Future Development of Female Genital Cosmetic Surgery (Intimate Surgery)
- The First Case of Free Radial Forearm Skin Flap:A 40-Year Follow-Up Study
- A Case of Digital Superficial Angiomyxoma
- Surgical Management for Diabetic Foot Ulcer:A Bibliometric Study
- Programmed 6-Step Approach of Improved Liposuction-Curettage for Axillary Bromhidrosis
- Foreword from Professor Lee L.Q.Pu