Programmed 6-Step Approach of Improved Liposuction-Curettage for Axillary Bromhidrosis
2020-12-22YanqiLIUYanmengPANMinxiaZHANGLiCHENFaweiXUHongfangMAXingHEYingHUGuijuanHEJiaqinCAIWeiqiangTAN
Yanqi LIU ,Yanmeng PAN ,Minxia ZHANG ,Li CHEN ,Fawei XU ,Hongfang MA ,Xing HE,Ying HU,Guijuan HE,Jiaqin CAI,Weiqiang TAN,*
1 Department of Plastic Surgery,Sir Run Run Shaw Hospital,Zhejiang University School of Medicine,3 East Qingchun Road,Hangzhou 310016,Zhejiang Province,People’s Republic of China
2 Department of Plastic Surgery,Fourth Affiliated Hospital,Zhejiang University School of Medicine,N1 Shangcheng Road,Yiwu,Zhejiang 322000,China
ABSTRACT Background Liposuction-curettage is a long-standing and effective treatment for axillary bromhidrosis.However,residual malodor and skin necrosis typically occur following this treatment.Therefore,we improved this method to ensure fewer complications and better outcomes.Here,we have presented our programmed 6-step approach of improved liposuction-curettage.Methods The programmed 6-step approach of improved liposuction-curettage was used to remove the axillary apocrine glands.We used pointed and obtuse cannulas designed for liposuction-curettage.Results Patients treated using the programmed 6-step approach of improved liposuctioncurettage did not experience any serious complications or residual malodor.Conclusion The programmed 6-step approach of improved liposuction-curettage was more effective than traditional surgery with respect to the treatment of axillary bromhidrosis.
KEY WORDS Axillary bromhidrosis; Liposuction-curettage; Programmed 6-step approach
INTRODUCTION
Axillary bromhidrosis is characterized by malodor owing to a genetic predisposition toward profuse apocrine sweat glands distributed in the armpits[1-2].Axillary bromhidrosis is common in adolescents,and the likelihood of postoperative recurrence has been reported to be higher in juvenile patients[3].
The purpose of axillary bromhidrosis treatment is to remove the axillary apocrine glands[4-5].There are many methods used during the treatment of this condition,including drug-based,physical,and surgical therapies.Although liposuction-curettage is a long-standing and effective treatment[6-7],residual malodor and skin necrosis often appear after treatment with this method[8-9].Therefore,we improved this technique to achieve greater effectiveness with fewer complications.Here,we have discussed our a programmed 6-step approach of improved liposuction-curettage.This programmed approach offers many advantages such as a small incision,short operative time,and high success rate.
METHODS
Surgical Technique
The operation was performed using liposuction-curettage cannulas and handles as well as negative-pressure drainage.
The instruments used for liposuction-curettage consisted of two spiral mini handles; two pointed liposuctioncurettage cannulas with diameters of 2.5 mm,each with two suction holes at the tip; two pointed liposuctioncurettage cannulas with diameters of 3 mm,each with three suction holes at the tip; and two obtuse liposuctioncurettage cannulas with diameters of 3 mm,each with three suction holes at the tip (Fig.1).The negativepressure suction device provided approximately 0.08-0.10 atm,enabling the use of a normal negativepressure suction device or liposuction machine.
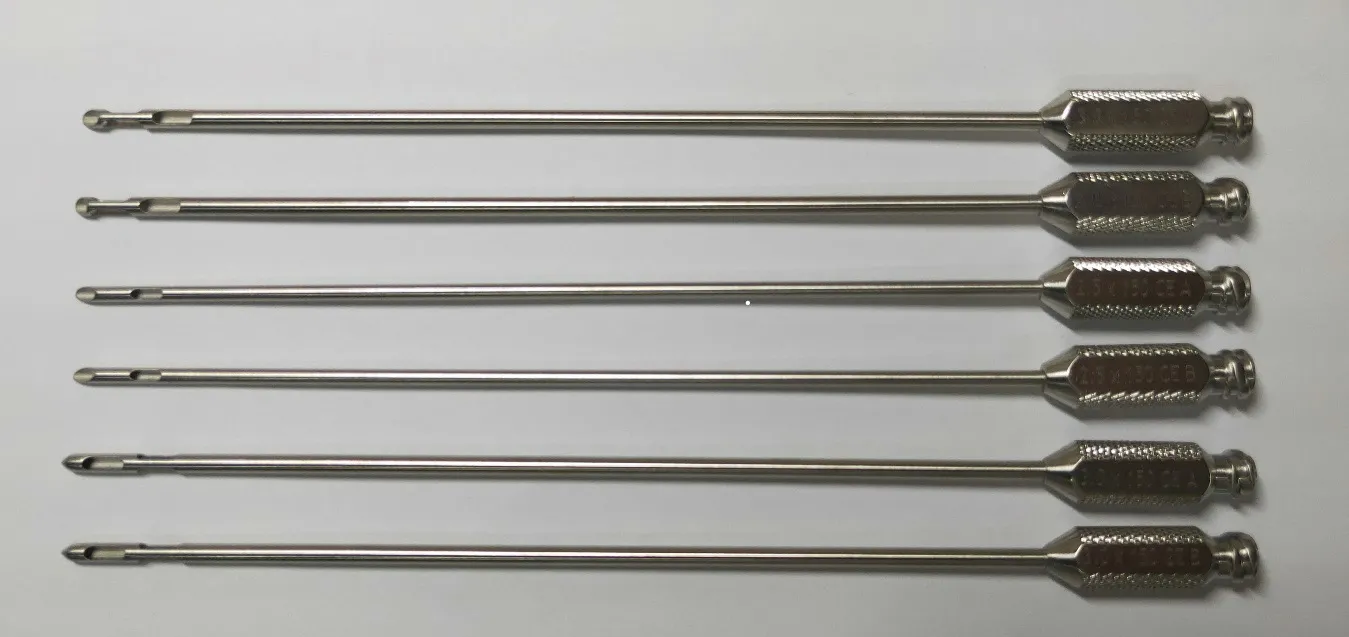
Fig.2 Preoperative marking defining the surgical area

Fig.2 Preoperative marking defining the surgical area
The patient was positioned in the supine position with the upper arms abducted at approximately 150°.The areas containing axillary hair were outlined,and the hair was shaved before surgery.Two tiny stab incisions were made at the inferior and lateral sides of each axilla approximately 0.5-1.0 cm beyond the outline (Fig.2).
Anesthesia
Local anesthesia was induced with a tumescent solution consisting of 500 mL of normal saline,0.5 mL of 0.1%epinephrine,20 mL of 2% lidocaine,and 15 mL of 5%sodium bicarbonate.In total,2-3 bottles were used.Depending on the size of the axillary hair area,300-750 mL of swelling solution was injected (approximately 300,500,and 750 mL in the small-,medium-,and largesized axillary hair areas,respectively,).Infiltration was performed with a 23-G needle according to the following three steps:
(1) Subcutaneous fat layer injection:The tumescent solution was quickly and evenly injected into the subcutaneous fat layer throughout the entire armpit hair area.The injection volume was relatively small.The aim was to ensure a painless operative area,thereby allowing the patient to feel more comfortable during the subsequent operation (Fig.3).

Fig.3 Subcutaneous fat layer injection
(2) Subdermal layer injection:The tumescent solution was injected into the subdermal layer.The needle was clearly visible beneath the skin,reaching the boundary of the layer without exceeding it.In fact,the tumescent area could exceed the edge of the axillary hair area by up to 2 cm.After anesthesia,the subcutaneous layer of the axillary area became firm,and the axillary apex flattened.The objectives were to enhance the anesthesia and separate some of the apocrine glands from the dermis (Fig.4).
(3) Subcutaneous fat layer injection:The tumescent solution was quickly injected into the subcutaneous fat layer and uniform injections were given once the tumescent area was easily identifiable.The goal was to make the tumescent area more solid and easy to curettage(Fig.5).

Fig.4 Subdermal layer injection

Fig.5
Surgical Procedures
We used our programmed 6-step approach of improved liposuction-curettage according to the following method:
(1) Liposuction with compression and curettage via an inferior incision
A pointed cannula with two suction holes was placed in the subdermal tunnel using an inferior incision,with the suction holes in the upward direction and facing the subcutaneous tissue.The cannula was held in one hand while stroking movements were made with the other to compress the skin for effective subdermal scraping(Fig.6).The position of the cannula could be felt with the fingers at this point.Effective subdermal scraping was performed using repeated twitching motions as well as open negative-pressure drainage.The pinhole could be seen under the skin after a few scratches in the same position.Liposuction-curettage was performed according to the protocol discussed hereafter.Radial liposuctioncurettage was thoroughly performed from left to right or right to left.The distance between the two distal tunnels was approximately 0.5-1 cm,and all armpit hair areas were covered.The tip was permitted to reach the boundary or exceed it by up to 0.5 cm,as exceeding it by more than 2 cm could cause pain.At the beginning of the scraping process,no holes were observed.As the liposuction-curettage progressed,the skin flap gradually thinned,and the suction holes under the skin could be seen clearly during the subsequent steps (Fig.6 and 7).When the thinning was very apparent,the first step was considered complete.When the inferior incisions could not be touched,the lateral incisions were supplemented using both liposuction with compression and curettage.

Fig.6 Liposuction with compression and curettage performed via an inferior incision

Fig.7
(2) Liposuction with compression and curettage via a lateral incision
A pointed cannula with two suction holes was inserted through the lateral incision.The method and requirements were the same as those described in step one (Fig.8 and 9).When a lateral incision could not be touched,the inferior incisions were supplemented using liposuction with compression as well as curettage.

Fig.8 Liposuction with compression and curettage performed via a lateral incision

Fig.9
(3) Liposuction-curettage via the inferior incision accompanied by skin pinching
An obtuse cannula with three suction holes was inserted through the inferior incision.The skin was pinched such that it surrounded the cannula using the thumb,index,and middle fingers; meanwhile,radiating,stroking movements were performed according to a specific protocol without any omission (Fig.10).The distance between the two distal tunnels was approximately 0.5-1 cm.During this process,the incisions on the surface of the skin can be clearly seen (Fig.11).When an inferior incision was not able to be touched,the lateral incisions were supplemented using liposuction with compression as well as curettage.

Fig.10 Liposuction with compression and curettage performed via the incision

Fig.11
(4) Liposuction-curettage via the lateral incision with skin pinching
An obtuse cannula with three suction holes was inserted through the lateral incision.The method and requirements were the same as those described in step one (Fig.12 and 13).When a lateral incision could not be touched,the inferior incisions were supplemented using liposuction with compression and curettage.

Fig.12 Liposuction-curettage performed via the lateral incision with skin pinching

Fig.13
(5) Repeated liposuction with compression and curettage
The first and second steps were repeated via the inferior and lateral incisions (Fig.14 and 15).Liposuction with compression and curettage were performed without any omission.The incisions were clearly visible,and the sweat glands were almost completely removed.In the cases without a subcutaneous scarring,there was no need to investigate the thickness of the layer.When subcutaneous scarring was observed,or when previous scraping was insufficient,skin pinching was repeated to surround the blunted cannula until the thicker area was scraped clean.
(6) Management of incisions

Fig.14

Fig.15
A pointed cannula with two suction holes was inserted through one incision while liposuction with compression and curettage was performed on another (Fig.16).All the pointed and obtuse cannulas with three suction holes were crossed via the same incision,and the skin was pinched around the cannula in the surrounding area (Fig.17).By the end of the surgical procedure,the skin was sufficiently thin to be pinched readily,the residual armpit hair was easily pulled out,and the skin color turned from white to purple (Fig.18).The surgery was complete when the axillary glands were removed and the postoperative result was deemed to be effective.
In each step,another incision was used if any part of the surgical area was inaccessible using one incision alone.In this manner,curettage and suction were performed throughout the entire surgical area.

Fig.16 Management of the incisions

Fig.17 Management of the incisions

Fig.18
Postoperative Management
A folded gauze was used to squeeze the armpit area from one side to the other a few times.After squeezing the residual liquid in the axillary region,the stab incisions were covered by dressings without being stitched up.A large cotton ball was unrolled and spread out,thickened layer by layer,wrapped in sterile gauze,and packed into the shape of the armpit hair area (Fig.19).We ensured that the bottom layer was intact.If the layer was not large enough,it could be expanded by pulling.The surgical area was then covered using pressure dressing.Moreover,patients were fitted with a convenient and comfortable one-piece armpit compression garment to provide constant axillary pressure (Fig.20).The patient was advised to avoid elevation of the upper arms,rotation of the shoulder joints,and upper extremity exertion and sweating for one week.
The dressing was changed dressing 7 days after the surgery.If sufficient healing had occurred (as it has in 90% of our current patients),the dressing and axillary garment was removed on the same day,and the wound was covered with sterile dressing for 3-4 days after disinfection.Axillary movement was discouraged for 8-14 days after the operation.After approximately 15 postoperative days,a gradual increase in functional exercise in the form of omnidirectional axillary movement was recommended.

Fig.19

Fig.20
Dressings were changed on postoperative day 7 if wound healing was deemed insufficient.It should be noted that the axillary garment could be removed either on the same day or 1-3 days later depending on whether the wound showed effusion and the skin was well fitted,and the onset of functional exercise could be scheduled accordingly.If effusion was found,the axillary garment was worn for another 3-7 days after the removal of effusion.
RESULTS
Our results showed that the programmed 6-step approach of improved liposuction-curettage for axillary bromhidrosis was more effective at eliminating malodor than traditional surgical methods.No serious complications occurred,except for minimal skin necrosis and localized epidermal injury.Patients with small areas of skin necrosis recovered within 1-3 weeks after frequent dressing changes.Patients with local epidermal injury recovered within 7 days when dressings were changed as needed.Although the growth of axillary hair completely ceased in some patients,the growth was merely reduced in most patients.In addition,neither the patient nor those close to them could detect any bromhidrosis.None of the patients experienced any residual recurrence during the three months of follow-up.
DISCUSSION
The effectiveness of the liposuction-curettage method stems from the fact that it simultaneously treats the subcutaneous fat layer and the portion of the subdermal layer in close proximity to the dermis.As the surgical area only corresponds to 90% of the distribution range of the apocrine glands,extensive removal is warranted[10,11].In our study,a large quantity of tumescent solution was injected beneath the dermis,providing surgical access and ensuring the ease and effectiveness of the first surgical step.
During the first and second steps of our liposuctioncurettage method,the tip and suction holes both faced the dermal layer,and the suction hole could be seen during procedure itself.The other hole was located in the subcutaneous region,thereby facilitating the removal of large apocrine glands in the deep subcutaneous layer[12].During liposuction-curettage,the other hand compressed the skin to enhance the effectiveness of the treatment.As the operation progressed,the outline of the suction hole became clearer.In fact,the first two steps removed most of the sweat glands,thereby greatly enhancing the effectiveness of the surgery[13].During each step,liposuction-curettage could be repeated if any areas had previously been omitted.
In contrast to the traditional negative-pressure drainage method,the third and fourth steps of our approach combined skin pinching and scraping.Since obtuse and pointed cannulas have three holes for scraping,each contact surface between the skin and needle can be scraped,maximizing the efficiency and convenience of each scrape.In our study,the distance between the two sequential radiating channels was 5-10 mm and was clearly visible during the operation.In the fifth and sixth steps,we scraped the thicker areas with suspected residue and the area surrounding the surgical incision,respectively.In doing so,the extent of the scraping was made more comprehensive,and the scraping of any blind spots was avoided to the greatest possible extent.The combination of skin pinching and compression ensured efficiency of the scraping.This was an important aspect of removing the malodor associated with this condition.
After the operation,compression dressing consisting of multilayer,tiled cotton balls wrapped with gauze was used to evenly pressurize the operative area.In line with previous reports,we found that compression packing was able to reduce the incidence of skin necrosis.
Our method offers several distinct advantages,such as small incisions,short operative times,a simple surgical technique,a high success rate,rapid recovery,and a low prevalence of complications[14].Compared with traditional liposuction-curettage,it is conceivable that our programmed 6-step approach of improved liposuctioncurettage and surgical techniques using obtuse and pointed cannulas can complement one another[11].Programmed and organized scraping ensures complete and uniform scraping of the surgical area[15].Liposuction with compression and curettage can effectively remove stubborn sweat glands close to the dermis as well as those in the subcutaneous fat layer.
It should be noted that the incidence of recurrence and residual problems are prominent concerns in patients with axillary bromhidrosis.With respect to the recurrence rate,this study has some limitations.Our data showed that no patients experienced residual recurrence during the three months of follow-up.However,we did not have specific statistics regarding patients who were treated by traditional surgical methods or our improved 6-step liposuction-curettage technique,thereby eliminating the possibility of a quantitative comparison.
CONCLUSIONS
Our improved 6-step approach for liposuction-curettage yielded superior outcomes to those obtained using traditional surgical procedures.The surgical area corresponds to almost 90% of the distribution range of the apocrine glands,which were removed to the greatest possible extent.Moreover,by pinching the skin that surrounded the cannula,effective scraping was achieved in all regions In conclusion,our programmed approach offers numerous advantages,such as a small incision,short operative time,and high success rate.
ACKNOWLEDGMENTS
We would like to thank all members of the Department of Plastic Surgery,Sir Run Run Shaw Hospital,College of Medicine,Zhejiang University for their suggestions regarding this modified approach for the treatment of axillary bromhidrosis.Moreover,we want to thank three nurses from the Department of Plastic Surgery—Xiao-Li Liu,Xiu-Na Shao,and Mei-Ping Zhao—whose efforts were indispensable during the surgery.
FUNDING
The authors would like to disclose that this work was supported by grants from the National Natural Science Foundation of China (No.81671918) and Zhejiang Provincial Medical and Healthy Science Foundation of China (No.2019ZD028 and 2019KY757).
ETHICS DECLARATIONS
Ethics Approval and Consent to Participate
This study received ethical approval from the ethics committees at the Sir Run Run Shaw Hospital and the Fourth Affiliated Hospital,Zhejiang University School of Medicine.All participants provided written informed consent prior to enrolment in the study.
Consent for Publication
All the authors have consented for the publication.
Competing Interests
The authors declare that they have no competing interests.The authors state that the views expressed in the submitted article are their own and not the official position of the institution or funder.
杂志排行

Chinese Journal of Plastic and Reconstructive Surgery的其它文章
- Status Quo and Future Development of Female Genital Cosmetic Surgery (Intimate Surgery)
- The First Case of Free Radial Forearm Skin Flap:A 40-Year Follow-Up Study
- A Case of Digital Superficial Angiomyxoma
- Meteorological Influence on Tissue Expander-Related Major Infection
- Surgical Management for Diabetic Foot Ulcer:A Bibliometric Study
- Foreword from Professor Lee L.Q.Pu