Liver fat accumulation measured by high-speed T2-corrected multi-echo magnetic resonance spectroscopy can predict risk of cholelithiasis
2020-10-29HongChenWeiKeZengGuangZiShiMingGaoMenqZhuWangJunShen
Hong Chen, Wei-Ke Zeng, Guang-Zi Shi, Ming Gao, Menq-Zhu Wang, Jun Shen
Abstract
Key words: Magnetic resonance spectroscopy; Cholelithiasis; Liver fat accumulation; Steatosis; Iron
INTRODUCTION
Cholelithiasis is one of the most common and substantial health problems of the digestive system worldwide[1-3]. Although the prognosis of cholelithiasis has improved with advances in surgical and imaging technology, it still constitutes one of the common causes of hospitalization and can lead to cholecystitis, obstructive jaundice, acute pancreatitis, cholangitis, and gallbladder cancer[4]. Clinically, the diagnosis of cholelithiasis is not difficult. However, there has been a considerable effort to identify a surrogate marker to predict the risk of cholelithiasis. Previously, abdominal visceral fat accumulation[5-7]and excessive heme iron consumption[8]were found to be related to a higher risk of gallstone disease. Liver fat accumulation associated with increased body cholesterol synthesis and hypersecretion of biliary cholesterol may also be related to cholelithiasis development[7], and nonalcoholic fatty liver disease (NAFLD) is an independent risk factor for cholelithiasis development[9-11]as well as gallstonerelated diseases with an odds ratio (OR) of 3.6[12].
Currently, liver biopsy is the gold standard for evaluating liver fat accumulation. However, biopsy is an invasive procedure limited by sampling bias and variability among observers and intra-observers; moreover, it may also lead to complications such as bleeding and pseudoaneurysms[13]. Computed tomography (CT)[14]and ultrasonography[15]have been previously used to detect liver steatosis. CT measures liver fat content based on the ratio of Hounsfield units of the liver and kidney parenchyma and detects liver iron overload by showing increased attenuation[16]. However, both CT and ultrasonography have limited accuracy. Moreover, patients undergoing CT examination have the risk of radiation exposure. Recently, magnetic resonance imaging (MRI) has become a noninvasive method for quantifying liver fat content based on the difference between water and fat resonance frequencies[17]. Chemical shift imaging based on the two-point Dixon method has been widely used to analyze fat content by a simple algebraic operation of in-phase and opposed-phase images[18]. However, this method is susceptible to the effect of magnetic field inhomogeneity. The latest modified Dixon technique with six echoes and T2* correction (multi-echo Dixon) can obtain high-quality whole liver 3D proton density fat fraction (PDFF) and R2* maps[19]. However, confounding factors, such as T1 bias and T2* decay, require correction for more accurate quantification[20].
Advanced magnetic resonance spectroscopy (MRS) has been shown to be a robust method for quantifying liver fat and iron accumulation[21-24]. The multi-echo singlevoxel stimulated echo acquisition mode (STEAM) spectroscopy sequence minimizes the influence of T1 relaxation and corrects the T2 effect of different echo times (TEs), and can achieve satisfactory quantification of liver fat and iron[25]. This technique measures the PDFF by the exponential fit of five echoes to infer the area under the fat and water peak at TE = 0 ms, the fraction of liver proton density attributable to liver fat, which is a basic tissue characteristic and a direct method for measuring liver fat content. It can quantify liver fat in a single breath-hold of 15 s and can accurately quantify liver iron with R2 values[22,26]. Nowadays, multi-echo MRS is regarded as the non-invasive gold standard for quantifying liver fat and iron content[27,28]. However, whether liver fat and iron content as assessed by multi-echo MRS are predictive of cholelithiasis remains to be determined.
In the present study, high-speed T2-corrected multi-echo MRS was performed in patients with cholelithiasis to quantify liver fat and iron contents. The purpose of this study was to investigate whether liver fat content measured by PDFF derived from high-speed T2-corrected multi-echo MRS can predict the risk of cholelithiasis.
MATERIALS AND METHODS
Study population
The study was approved by the Institutional Review Board of our hospital (approval No. SYSEC-KY-KS-2020-047). Informed consent from each participant was waived because of the retrospective nature of the study. Patients with cholelithiasis including gallstones or cholangiolithiasis between March 2019 and November 2019 were identified from our hospital database. Patients were included if they had cholelithiasis confirmed by ultrasonography, and underwent liver MRI examination including highspeed T2-corrected multi-echo MRS. The exclusion criteria were as follows: Age < 18 years, alcohol consumption of more than 30 g per day within the preceding 10 years or more than 10 g per day in the previous year, liver cirrhosis caused by drugs or hepatitis virus, chronic liver disease, liver inflammation, liver tumors, history of liver surgery, history of diabetes, medication for hypertension, and malignant tumors of other organs. The age-matched healthy adults were included as controls. The inclusion criteria for the control group were as follows: Age > 18 years and no history of gallbladder disease, liver tumor, liver inflammation, cirrhosis, or liver surgery. The exclusion criteria were: Unavailable information on alcohol consumption and history of advanced cancer, diabetes, or hypertension. Finally, 40 patients with cholelithiasis (aged 54.8 ± 14.6 years, 23 men and 17 women) and 31 healthy controls (aged 50.6 ± 14.3 years, 21 men and 10 women) were included in the study.
MRI protocol
MRI was performed on a 3T MR scanner (MAGNETOM Skyra; Siemens Healthcare, Erlangen, Germany), using an 18-channel phased-array surface coil. MRI sequences included conventional MRI and high-speed T2-corrected multi-echo single-voxel1HMRS. The participants underwent conventional MRI prior to MRS acquisition to position the voxel. This sequence was performed in a single breath-hold of 15 s. The acquisition parameters were as follows: Echo time (TE) = 12, 24, 36, 48, and 72 ms, repetition time (TR) = 3000 ms, and flip angle = 90°. STEAM was used because of its inherently short TE[13]and can provide more consistent fat fraction estimates due to Jcoupling effects compared with the point-resolved spectroscopy (PRESS) model[23]. A total of 1024 sampling points were acquired at a bandwidth of 1200 Hz. The voxel size was 30 mm × 30 mm × 30 mm. An experienced MRI technologist placed the voxel in the right lobe of the liver, avoiding blood vessels, bile ducts, chemical displacement artifacts, and fluctuations. This technique uses signal integrals from water and lipid spectrum fits to estimate T2 decay and assess the equilibrium signal at TE of 0 ms[22]. The obtained MRS data were post-processed inline by using the prototype software package (Siemens Healthcare, Erlangen, Germany), and a spectrum with T2 correction, a table report with the quantitative information (fat fraction, and R2 value of water and fit error), PDFF, and R2 map were obtained automatically[19](Figure 1).
Laboratory and anthropometric evaluations
Serum alanine aminotransferase, gamma glutamyl transpeptidase (GGT), aspartate aminotransferase, total bilirubin, alkaline phosphatase, serum uric acid, serum uric glucose, total cholesterol, triglycerides, serum iron, serum iron saturation, serum ferritin, transferrin, and hemoglobin were measured using standard reagents. Waist circumference (WC) was measured horizontally at the level of the umbilicus on the MR images for each participant. The time between laboratory examination and MR examination was within one week.
Statistical analysis
Numerical variables are presented as the mean ± SD. Fisher’s exact test was used for comparing categorical variables. Data distributions were tested for normality by Shapiro-Wilk test. Mean values were compared between the cholelithiasis group and control group by either Student’st-test (when data were normally distributed) or nonparametric Mann-WhitneyU-test (when data were not normally distributed). Spearman’s correlation was used to analyze the relationship between MRI-based PDFF, R2, and WC. Univariate logistic regression analysis, followed by multivariate logistic regression analysis, was performed to determine independent predictors of cholelithiasis. Receiver operating characteristic curve (ROC) analysis was used to evaluate the performance of significant parameters in discriminating cholelithiasis from healthy controls. The optimal cut-off value was determined according to the Youden index. APvalue < 0.05 indicated statistical significance (two tailed). All statistical analyses were performed using SPSS (Chicago, IL, United States, version 23.0).
RESULTS
Demographic and clinical characteristics of the study population
The demographic and clinical characteristics of the study population are shown in Table 1. In the cholelithiasis group, mean WC ranged from 62.9 cm to 99.1 cm. In the healthy group, WC ranged from 64.6 cm to 93.8 cm. WC was significantly higher in the cholelithiasis group than in the healthy group (85.3 ± 9.0 cmvs81.0 ± 6.9 cm,P= 0.030). Mean GGT level was significantly higher in patients with cholelithiasis than in the healthy group (246.3 ± 317.8 U/Lvs103.8 ± 146.4 U/L,P= 0.037). The normal range of GGT level is 45-125 U/L. There were no significant differences in other biochemical findings between the cholelithiasis group and healthy controls.
FDFF, R2, and liver iron concentration
In the cholelithiasis group, PDFF ranged from 1.5% to 20.6%, and R2 values ranged from 24.4/s to 129.4/s. In the healthy group, PDFF ranged from 0.4% to 11.5%, and R2 values ranged from 17.2/s to 53.7/s. Mean PDFF (5.8% ± 4.2%vs3.3% ± 2.4%,P= 0.001) and mean R2 (50.4 ± 24.8/svs38.3 ± 8.8/s,P= 0.034) values were significantly higher in the cholelithiasis group than in the healthy group. The values of liver iron concentration (LIC) extrapolated from R2 values were calculated based on the known iron calibration equation[29,30]. In the cholelithiasis group, LIC ranged from 0.48 mg/g to 10.01 mg/g dry tissue. In the healthy group, LIC ranged from 0.21 mg/g to 2.18 mg/g dry tissue. Mean LIC values were significantly higher in the cholelithiasis group (2.21 ± 2.17 mg/g dry tissuevs1.22 ± 0.49 mg/g dry tissue,P= 0.034) than in the healthy group (Figure 2).
Correlation and regression analyses
Correlation analysis showed that there was a positive correlation between PDFF and WC (r= 0.502,P< 0.001) and PDFF was positively correlated with R2 (r= 0.425,P< 0.001) (Figure 3 and Table 2). Univariate logistic regression analysis showed that PDFF, R2, WC, and GGT were significantly associated with cholelithiasis (P< 0.05). PDFF, R2, WC, and GGT were chosen for multivariate logistic regression analysis and only PDFF was a significant independent risk factor for predicting cholelithiasis (P= 0.003, OR: 1.79, 95%CI: 1.22-2.62).
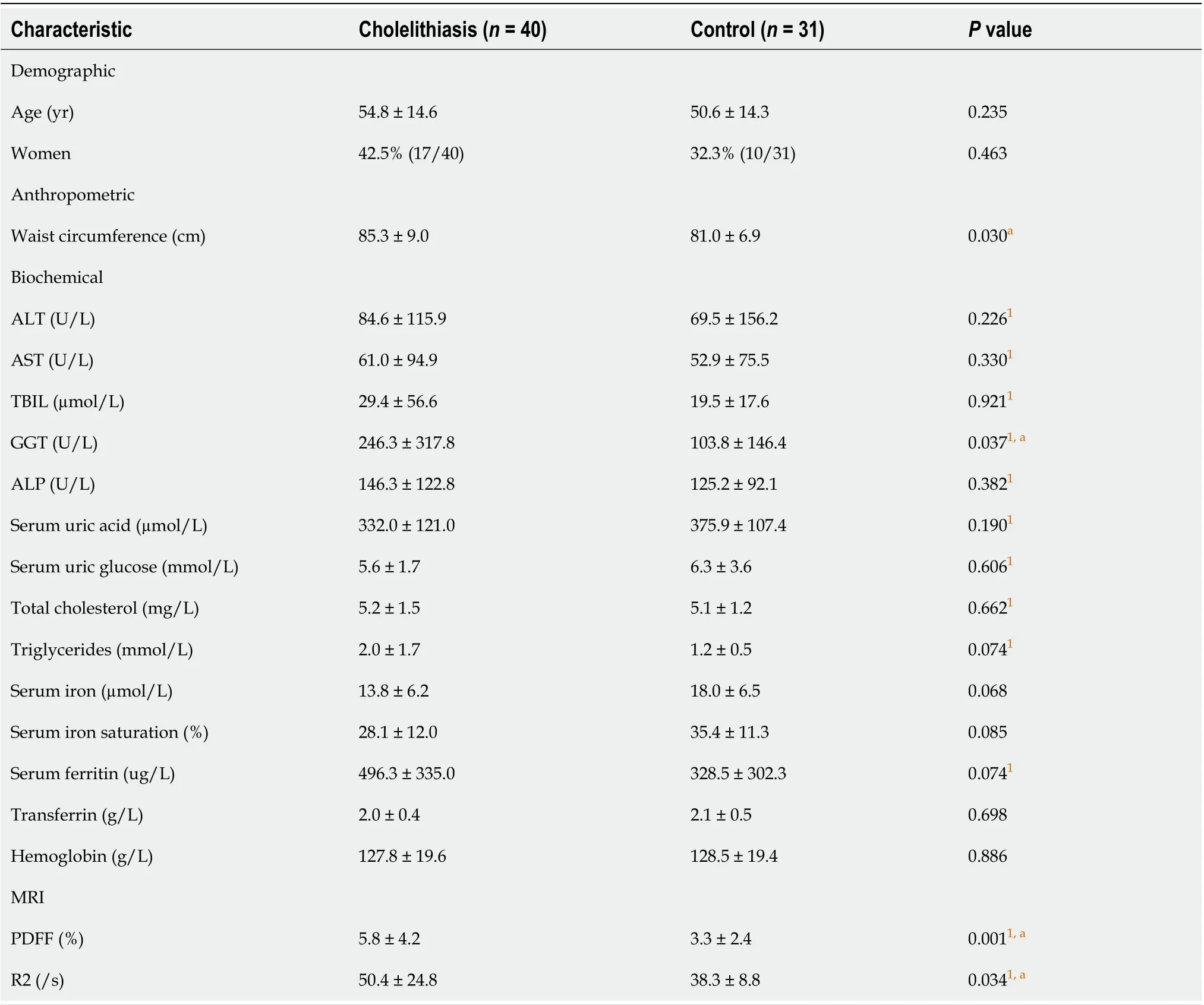
Table 1 Demographic, anthropometric, biochemical, and magnetic resonance imaging parameters in patients with cholelithiasis and healthy controls
ROC analysis
ROC analysis showed that the area under the curve (AUC) of PDFF was 0.723. With an optimal threshold of 4.4%, PDFF had a sensitivity and specificity of 55.0% and 83.9%, respectively, for discriminating cholelithiasis from healthy controls (Figure 4).
DISCUSSION
Our study showed that patients with cholelithiasis had a higher liver fat content and R2 value as assessed by high speed T2-corrected multi-echo MRS. Liver fat fraction rather than R2 or WC was a significant independent risk factor for cholelithiasis. To our knowledge, this is the first study to show that liver fat accumulation is a risk factor for cholelithiasis using quantitative MRS.
There is a high prevalence of liver steatosis in cholelithiasis patients. Roldan-Valadezet al[3]found that approximately half of patients with symptomatic cholelithiasis have liver steatosis histologically, when a cut-off value > 5% in total lipid content of liver biopsies is defined as liver steatosis[31]. It is known that an increase in total cholesterol synthesis in the body can cause tissues to be overloaded with fatty acids, resulting in more lithogenic bile by the overproduction of hepatic cholesterol[10].The increase in cholesterol synthesis and the high secretion of biliary cholesterol might cause the accumulation of liver fat, and may be related to the occurrence of cholelithiasis[6]. Thus, it is important to monitor liver fat content longitudinally in patients with liver fat accumulation. Previously, GGT was shown to be a surrogate indicator for liver fat accumulation in middle-aged adults in China[32]. A large-scale longitudinal cohort study using ultrasound imaging in 283446 Korean adults demonstrated a bidirectional association between liver steatosis and gallstones[33]. Furthermore, Kolleret al[34]demonstrated that NAFLD may represent a pathogenic association between metabolic syndrome and cholelithiasis[34]. Our results showed that patients with cholelithiasis had an average PDFF of 5.8%, which was higher than that in healthy controls. This is consistent with the results of previous findings[3,10,11]. Compared with traditional ultrasound and CT examination, MRS can be used for quantitative detection of mild liver steatosis[17], especially in patients with grade 1 steatosis. PDFF measured by MRS could quantitatively detect liver steatosis in a simple breath-hold of 15 s, which showed a good potential for clinical application.

Table 2 Results of univariate and multivariate logistic regression analyses
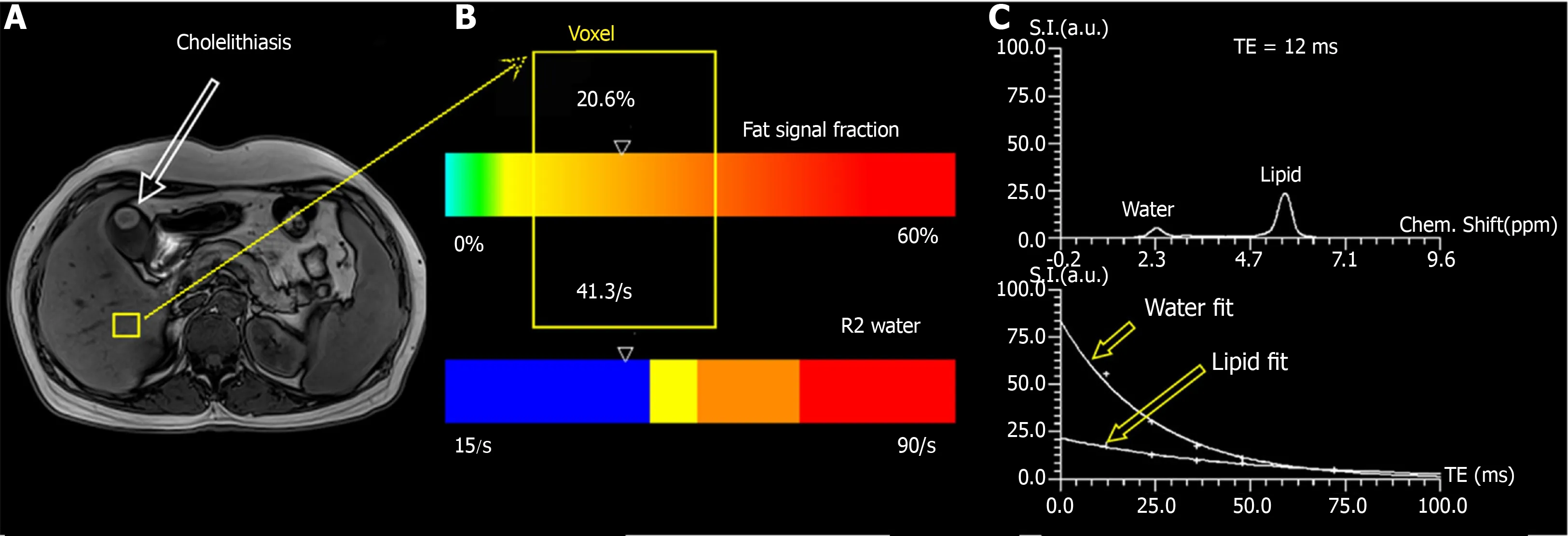
Figure 1 Measurement of proton density fat fraction and R2 values using T2-corrected multi-echo single-voxel 1H-magnetic resonance spectroscopy. A: The voxel of liver (yellow square) is shown in a 43-year-old man with cholelithiasis; B: Results are presented as a colored bar indicating the corresponding values of proton density fat fraction and R2 (yellow box), and the value of PDFF and R2 was 20.6% and 41.3/s, respectively; C: The water and fat spectra for T2 = 12 ms and the exponential decay fit for the five echoes. Upper image: Representative spectrum of water and lipid. Lower image: Graph of T2 decay of water and lipid shows marked differences in decay rate and signal integrals from water and lipid spectrum fits were used to measure T2 decay and estimate the equilibrium signal.
Abdominal visceral fat accumulation is a commonly used measure to predict the risk of cholelithiasis. A multi-ethnic study of atherosclerosis previously showed that WC could provide the best discrimination for NAFLD in the total population[35]. WC has exhibited potential use in monitoring changes in visceral adipose tissue deposits, which convey the greatest health risks[36]. Similarly, previous studies have also shown that WC predicts the risk of developing gallstones in United States men[37]and Chinese adults[5], and was strongly associated with liver fat in women in a white German population[38]. Cholelithiasis and liver steatosis may share a common risk factor such as obesity, which can be assessed quantitatively by WC. In our study, patients with cholelithiasis also had higher WC, and PDFF was positively correlated with WC. Moreover, our study demonstrated that only PDFF was an independent predictor of cholelithiasis by multiple logistic regression analysis with an OR of 1.79 and an AUC of 0.723 in discriminating cholelithiasis from healthy controls. Notably, although WC is an easily achievable indicator of obesity, it is insensitive in the detection of mild liver steatosis. Dinget al[32]also found no significant correlation between WC and the risk of coronary stenosis after multivariable adjustment and liver fat accumulation may be more important in predicting subclinical coronary atherosclerosis than general and abdominal fat accumulation. Previous studies have demonstrated that PDFF derived from MRS had an accuracy of 100% in assessing fat concentration in patients with symptomatic cholelithiasis histologically[3]and could be used for the quantification of varying degrees of hepatic steatosis in histology[39,40]. Taken together, these results highlight the superiority of MRS over morphometric assessment when assessing and monitoring mild liver steatosis in cholelithiasis.

Figure 2 Graphs show proton density fat fraction (A), waist circumference (B), R2 (C), and liver iron concentration (D) values in the cholelithiasis group and healthy controls. Variables are presented as the mean ± standard deviation. PDFF: Proton density fat fraction; WC: Waist circumference; LIC: Liver iron concentration.
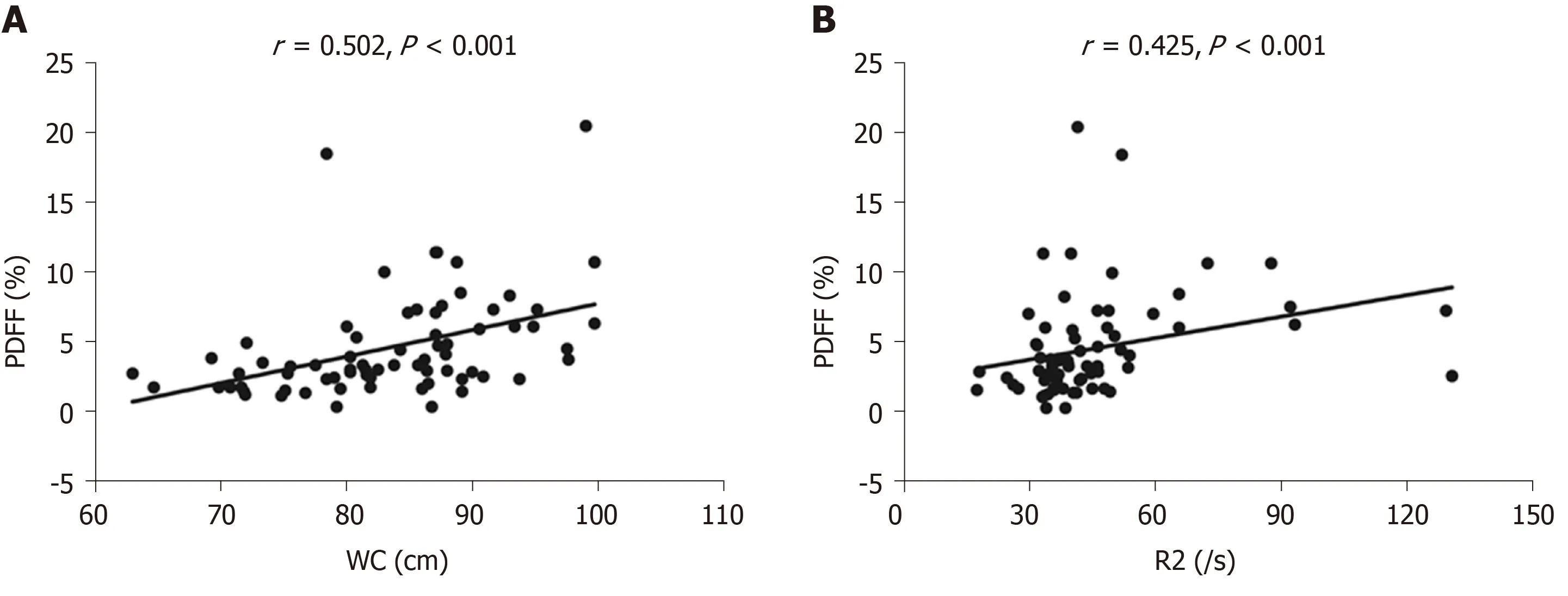
Figure 3 Scatter plots show a correlation between proton density fat fraction and waist circumference (A) and between proton density fat fraction and R2 (B). PDFF: Proton density fat fraction; WC: Waist circumference.
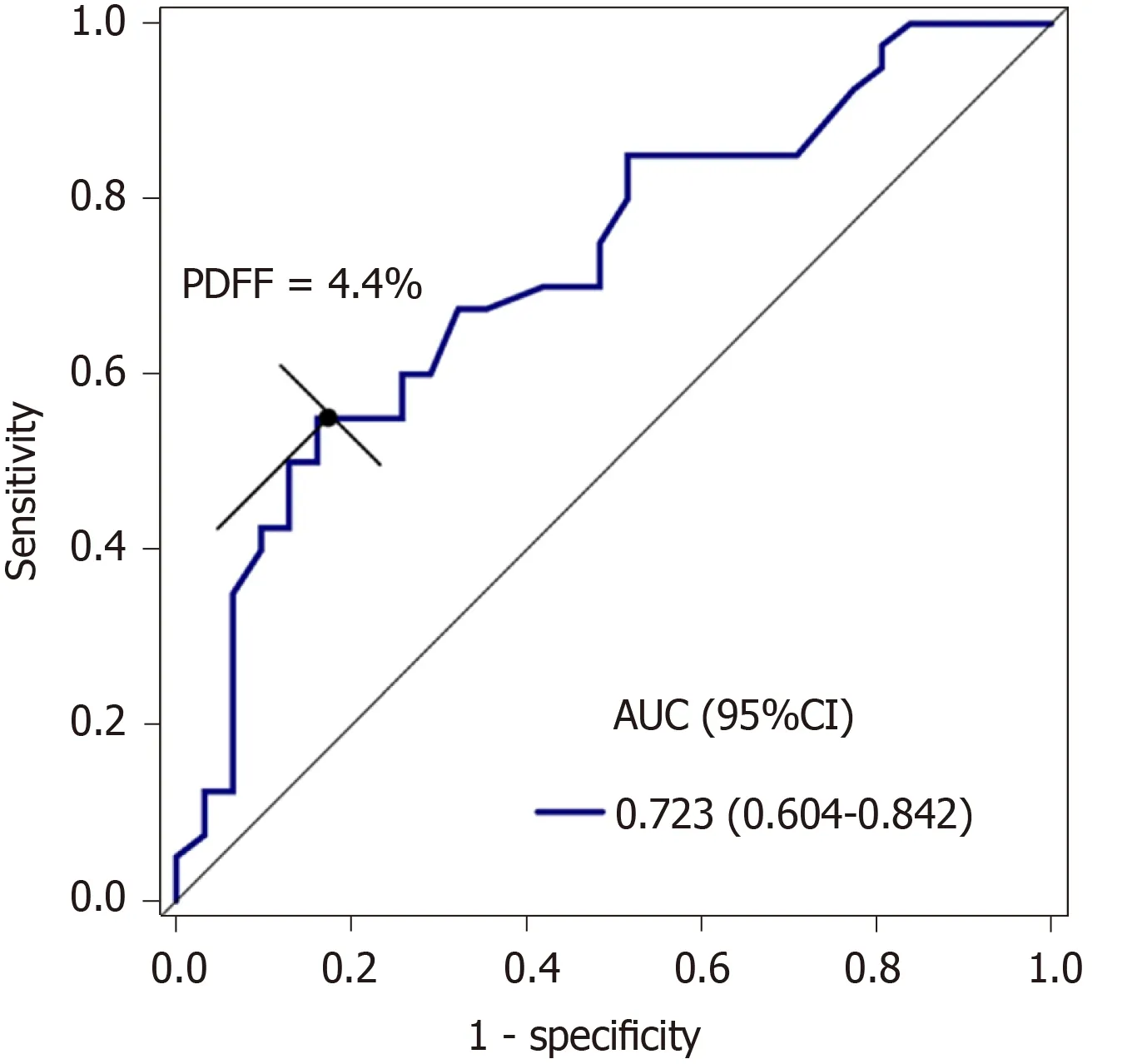
Figure 4 Receiver operating characteristic curve shows that the area under the curve of proton density fat fraction was 0.723 (95% confidence interval: 0.604-0.842) at a cut-off of 4.4% for discriminating cholelithiasis from healthy controls, with a sensitivity of 55.0% and specificity of 83.9%. PDFF: Proton density fat fraction; CI: Confidence interval; AUC: Area under the curve.
In our study, patients with cholelithiasis had a mild magnitude of increase in PDFF and LIC than normal controls. Iron overload has the ability to synergistically upregulate the level of ferritin and fat accumulation in an intact organism,e.g.,Caenorhabditis elegans, thus providing experimental evidence supporting the link between iron and obesity[41]. In addition, a previous study has also demonstrated that liver iron load inuences hepatic fat fraction in dialysis patients who routinely received erythropoiesis-stimulating agents and iron therapy, and iron overload induced by iron therapy may aggravate or trigger NAFLD in dialysis patients[42]. This study confirmed the ability of iatrogenic iron overload in dialysis patients to induce an increase of liver fat fraction and its regression with the normalization of LIC. Taken together, iron products may have an adverse effect on the pathophysiology of NAFLD.
In our study, patients with cholelithiasis also showed higher R2 values. Both R2 relaxometry and R2* relaxometry can be used to determine LIC. R2 relaxometry shows an excellent correlation with the LIC but requires a long imaging time (approximately 20 min). The R2* relaxation method shows excellent reproducibility, but the fact that sequence parameters and image analysis programs differ in many studies has been described as a disadvantage[43]. Liver iron plays an important role in the development of non-alcoholic steatohepatitis (NASH)[38]. Iron overload itself can cause liver cell injury, and any hepatocyte injury can also lead to iron accumulation[44]. The coexistence of increased liver fat can further increase the risk of NASH development, and even promoted the development of liver fibrosis and hepatocellular carcinoma[29,45]. Our study demonstrated a positive correlation between PDFF and R2 value. Similarly, Mamidipalliet al[46]found an association between R2* and PDFF. In their study, a chemical shift-based imaging approach, other than multi-echo T2-corrected MRS, was used to analyze liver fat content. Karlssonet al[26]also demonstrated a positive linear correlation between PDFF and R2* in chronic liver disease after excluding data from patients who had elevated iron levels. However, we measured PDFF using the STEAM model, whereas Karlssonet al[26]measured PDFF using the PRESS sequence[26]. Compared with PRESS, the STEAM model adds a damage gradient to eliminate the residual magnetization vector before each 90° pulse, thereby reducing approximately half of the TE value to obtain the attenuation curve of water and fat. This sequence allows for clearer separation of water and lipid in the spectrum signal[23,47]and provides a more consistent fat fraction estimate compared to PRESS[47]. A previous study demonstrated that liver fat content was an influential covariate of liver R2* value in a population with NAFLD, regardless of field strength[48]. T2-corrected MRS has been shown to more accurately simulate the variable T2 effects as evaluated using eight lipid phantoms doped with iron and is considered an accurate and repeatable method for noninvasive liver lipid quantification[22]. Collectively, MRS can be used as a quantitative tool to simultaneously monitor the liver fat content and hepatic iron overload[29].
Our study has some limitations. First, the sample size was relatively small as patients were recruited from one institution. A large population from multiple centers is needed for further validation of our findings. Second, liver biopsy was not performed in our study. Previous studies have shown that there is a correlation between MRS-PDFF and lipid content, and MRS-PDFF can reliably replace liver biopsy to evaluate liver fat content[3]. Although MRS cannot determine the size of fat droplets, it does determine the total amount of liver fat. Moreover, liver biopsy is unsafe and unethical in healthy participants. Third, MRS assesses liver PDFF and R2 in a single voxel. Measurement of fat and iron content from the entire liver might be suitable for heterogeneous liver steatosis. In such circumstances, multiple region of interests of MRS placed in different lobes of the liver can be adopted as a potential solution.
In conclusion, our study has demonstrated that PDFF measured by high speed T2-corrected multi-echo MRS is associated with cholelithiasis and is an independent risk factor for cholelithiasis. High speed T2-corrected multi-echo MRS can be used to detect liver fat accumulation to predict the risk of cholelithiasis development.
ARTICLE HIGHLIGHTS

Research conclusions
PDFF measured by high speed T2-corrected multi-echo MRS is associated with cholelithiasis. MRS can be used as a quantitative tool to simultaneously monitor the liver fat content and hepatic iron overload.
Research perspectives
This study describes that PDFF derived from high speed T2-corrected multi-echo MRS can predict the risk of cholelithiasis. MRS can quantitatively detect liver steatosis in a simple breath-hold of 15s, which holds a good potential for clinical application.
杂志排行

World Journal of Gastroenterology的其它文章
- Tumor necrosis factor alpha receptor 1 deficiency in hepatocytes does not protect from non-alcoholic steatohepatitis, but attenuates insulin resistance in mice
- Resveratrol alleviates intestinal mucosal barrier dysfunction in dextran sulfate sodium-induced colitis mice by enhancing autophagy
- Acute liver failure and death predictors in patients with dengue-induced severe hepatitis
- Surveilling Russell body Helicobacter pylori-negative gastritis: A case report and review of literature
- Tumor microenvironment in primary liver tumors: A challenging role of natural killer cells
- Exploring the food-gut axis in immunotherapy response of cancer patients