Coexistence of ovarian serous papillary cystadenofibroma and type A insulin resistance syndrome in a 14-year-old girl:A case report
2020-09-10FangFangYanBingKunHuangYinLingChenYanZhenZhuangXueYeYouChangQinLiuXueJunLi
Fang-Fang Yan, Bing-Kun Huang, Yin-Ling Chen, Yan-Zhen Zhuang, Xue-Ye You, Chang-Qin Liu, Xue-Jun Li
Fang-Fang Yan, Bing-Kun Huang, Yin-Ling Chen, Chang-Qin Liu, Xue-Jun Li, Department of Endocrinology and Diabetes, The First Affiliated Hospital of Xiamen University, Xiamen 361003, Fujian Province, China
Yan-Zhen Zhuang, Xue-Ye You, Department of Pathology, The First Affiliated Hospital of Xiamen University, Xiamen 361003, Fujian Province, China
Abstract
Key words:Type A insulin resistance syndrome;Ovarian serous papillary cystadenofibroma;Acanthosis nigricans;Treatment;Case report
INTRODUCTION
Type A insulin resistance syndrome (TAIRS), which is similar to Rabson-Mendenhall syndrome and Leprechaunism syndrome, is a rare disorder caused by mutations in the gene encoding the insulin receptor[1].It is usually diagnosed in lean adolescent girls accompanied by hirsutism, oligomenorrhea, acne, and acanthosis nigricans.In contrast to Rabson-Mendenhall syndrome and Leprechaunism syndrome, which are characterized by several phenotypes including intrauterine and postnatal growth retardation, dysmorphic features, and early mortality, TAIRS is relatively mild.Ovarian serous papillary cystadenofibroma is also an infrequent disorder that contains both epithelial and fibrous stromal components and is mainly found in women aged from 15 years to 65 years.Here, we present an unusual case of TAIRS coexisting with an ovarian cystadenofibroma in a 14-year-old girl.To the best of our knowledge, this is the first case to report such a combination.
CASE PRESENTATION
Chief complaints
A 14-year-old girl was transferred to our outpatient department with symptoms including hirsutism and acanthosis nigricans, which had been noted since the age of 10 years.Her birth weight was 2.75 kg at a gestational age of 40 wk.Secondary sex characteristics and accelerated growth occurred from the age of 13 but without menarche.
Physical examinations upon admission
Physical examination revealed that her body mass index was 18.1 kg/m2.The Ferriman-Gallwey score was 19 (average 5).Clinical symptoms, laboratory indices,and treatment of the patient during 2018-2019 are shown in Figure 1.Evidence of acanthosis nigricans was observed in the neck and axillae (Figure 2A-C).Examination of the genitalia disclosed a mild clitoromegaly.
Laboratory examination
A 75-g oral glucose tolerance test (OGTT) showed that plasma glucose was 5.7, 10.8,13.8, and 16.7 mmol/L at 0, 0.5-, 1-, and 2-h, respectively.Serum insulin concentrations were 1220.6, 2594.9, 3649.9, and 6958.3 pmol/L, respectively.Hemoglobin A1c(HbA1c) level was 8.3%.Hormone tests showed an elevated testosterone level at 82.85 ng/mL, (reference range 14-76 ng/mL).Molecular analysis showed a heterozygous missense mutation on exon 20 of the insulin receptor gene (Arg1201Trp) (Figure 3A).Furthermore, the patient’s phenotype matched the common genotypes of the mutation occurring in the insulin receptor gene.Chromosome test revealed a 46, XX karyotype.

Figure 1 Clinical symptoms and laboratory indices in the 14-year-old girl patient.
Imaging examination
No masses were identified on abdominal palpation.Pelvic sonography showed an 8.0 cm × 6.3 cm cystic lesion that extended to the upper right uterus, which appeared to originate from the ovary (Figure 2D).In addition, the cystic lesion included a larger quasi-circular anechoic area (1.4 cm × 1.2 cm) (Figure 2E).There was no free or circumscribed fluid in the pelvis.Patient was suspected to have an ovarian tumor.
Family history
Her father was diagnosed with type 2 diabetes by the 75-g OGTT (fasting glucose, 14.3 mmol/L and postprandial, 26.7 mmol/L).He did not show any common clinical features of TAIRS.His blood glucose was well controlled with metformin 500 mg three times a day.Her mother’s glucose level was normal by 75-g OGTT (Table 1).Fasting plasma glucose and fasting insulin level in her younger brother were 4.27 mmol/L and 212.67 pmol/L, respectively.The family history of diabetes is shown in Figure 4.Her father underwent genetic analyses and showed a heterozygous missense mutation on exon 20 of the insulin receptor gene (Arg1201Trp) (Figure 3B).Her mother was normal in the genetic analyses (Figure 3C).
FINAL DIAGNOSIS
Based on her clinical features, blood glucose, and insulin level, the patient was diagnosed with TAIRS.Final histopathological diagnosis of postsurgical tissue showed a right ovarian serous papillary cystadenofibroma accompanied by focal interstitial hyperplasia (Figure 2F and G).
TREATMENT
The patient took metformin for over 6 mo to treat TAIRS.Furthermore, laparoscopic resection (bilateral) of the ovarian lesion and laparoscopic intestinal adhesiolysis were performed under general anesthesia.
OUTCOME AND FOLLOW-UP
Fasting insulin level decreased to 857.84 pmol/L and HbA1c level dropped to 7.0%.Menstruation was not recorded during or after treatment.The patient had an uneventful recovery.Outpatient follow-up indicated that the patient was following the doctor’s advice by controlling her diet, taking her daily medicine, and exercising.

Table 1 Glucose and insulin levels of parents

Figure 2 Clinical characteristics, genetic diagnosis, and histopathological diagnosis in this patient.

Figure 3 Heterozygous mutation of the insulin receptor was observed in the patient and her father, as detected by Sanger sequencing(A-C).
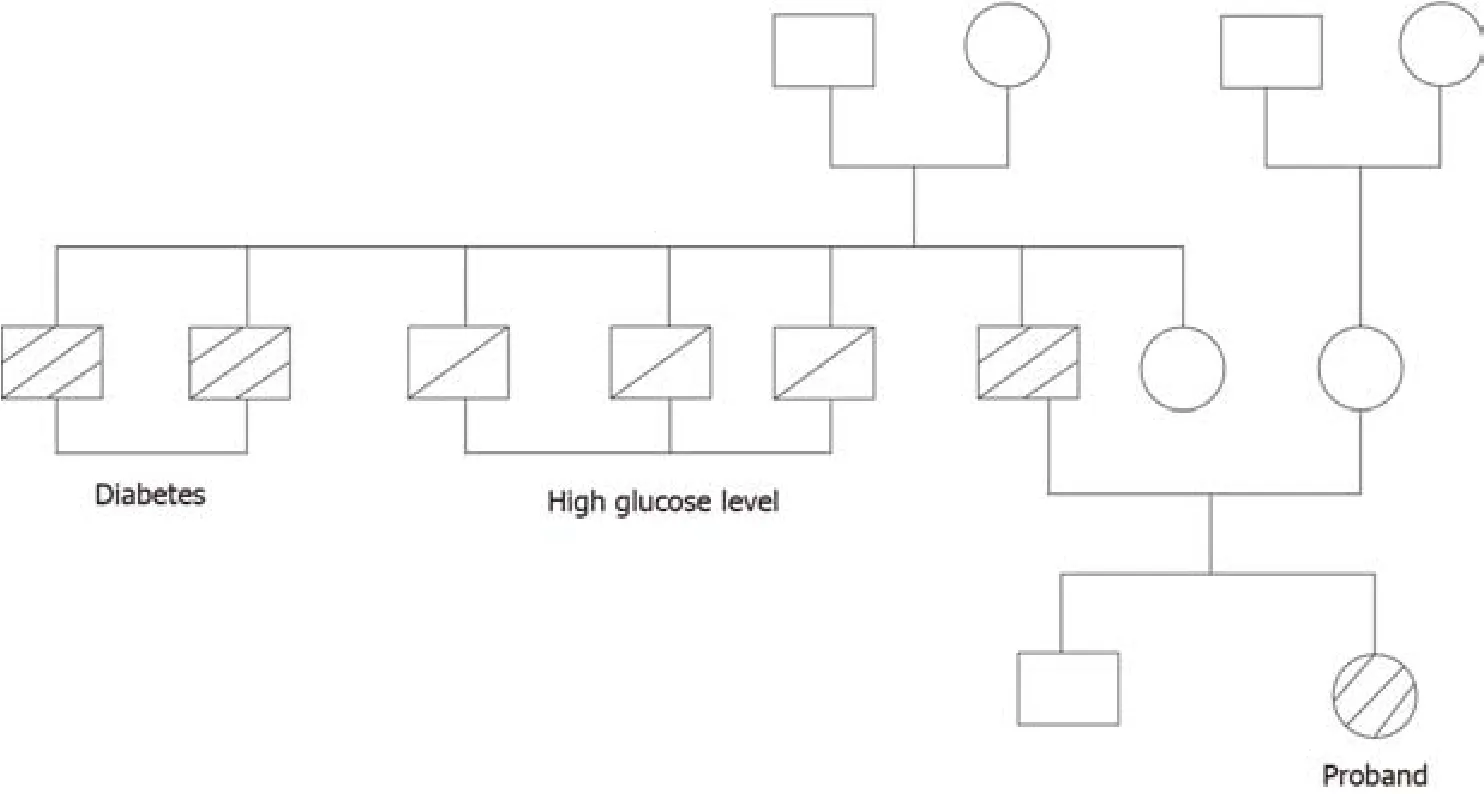
Figure 4 Family history of diabetes.
DISCUSSION
In this study, we report the first case of TAIRS coexisting with an ovarian serous papillary cystadenofibroma.TAIRS is one of three severe insulin resistance syndromes and is relatively mild.The patient showed hyperandrogenism, hyperinsulinemia,acanthosisnigricans, hirsutism, and diabetes mellitus but without the dysmorphic characteristic of leprechaunism or Rabson-Mendenhall syndrome.Moreover, genetic screening identified a single heterozygous mutation involving the tyrosine kinase domain in the β subunit of the insulin receptor gene.To date, more than 100 diseasecausing mutations have been identified[2], and the phenotype usually varies in patients with different gene mutations[3].The Arg1201Trp mutation that was identified in our patient has previously been reported in patients with severe syndromes of insulin resistance, such as leprechaunism and Rabson-Mendenhall syndrome[3-6],but has not been found in patient with TAIRS.Thus, the phenotype attributed to the mutation of the same gene locus can also be inconsistent.
There is a lack of large-scale, long-term, randomized controlled studies focusing on the treatment and prognosis of TAIRS to guide treatment choice in clinical practice.Treatment of TAIRS is usually empirical and lacks evidence.Many medications,including metformin, thiazolidinediones, acarbose, and leptin, have been used in patients with severe insulin resistance syndrome[7-10].In China, metformin is the only oral antidiabetic agent approved for use in patients under the age of 14 years.In our case, the patient was treated with metformin for 6 mo, and fasting serum insulin level decreased from 1220.55 pmol/L to 857.84 pmol/L, and HbA1c level decreased by 1.3%.This indicated that metformin had a partial effect and can improve insulin sensitivity to a certain degree, as reported previously[11].Despite acceptable control during adolescence, long-term metabolic control has been reported to be poor and diabetes complications are frequent in TAIRS patients[10,12].Therefore, other than metformin, several future-proof treatments such as metreleptin, sodium–glucose cotransporter 2 inhibitor, and incretin[10,13]should be introduced during childhood.
Ovarian cystadenofibroma accounts for 1.7% of all benign ovarian tumors[14]that originate in the epithelium, which are classified as serous, endometrioid, mucinous,clear cell, and mixed categories.Ovarian cystadenofibroma is usually asymptomatic and is found incidentally, as in our case.A cystadenofibroma may show a solitary cyst or a multiloculated cystic mass, with solid nodules or papillary projections, and almost half of cases demonstrate increased vascularity on ultrasonography[15].Clinically,because ovarian cystadenofibroma is a multicystic mass with solid components,preoperative differential diagnosis is important to distinguish it from malignant neoplasms.A computed tomography scan also provides limited information in the evaluation of this tumor.A frozen section diagnosis may be helpful in these cases and may help to avoid an extensive surgical procedure.The patient in this study had two rarely diagnosed conditions.It is unknown whether there is a correlation between these two rare diseases.Insulin can activate both the insulin receptor and insulin-like growth factor receptor, particularly at high concentrations, to promote tumor cell proliferation and migration, which possibly plays a critical role in tumor development and progression[16,17].Previous studies suggest that exogenous insulin exposure is significantly associated with an increased incidence of cancer[18].Although a high insulin level may be related to ovarian serous papillary cystadenofibroma onset and/or progression, the mechanism remains unclear.Further study is required to determine the mechanistic details associated with the connection between TAIRS and ovarian cystadenofibroma.
In this report, we highlight the rare coexistence of TAIRS and an ovarian serous papillary cystadenofibroma.However, this study also had some limitations.First,there was an over 1-mo delaying in treating TAIRS as the patient underwent surgery.Second, the patient’s ovarian cysts were surgically treated more than 1 year after diagnosis.
CONCLUSION
We report the first case of TAIRS coexisting with an ovarian serous papillary cystadenofibroma in a 14-year-old girl.We found that metformin had partial efficacy in TAIRS and improved insulin sensitivity to a certain extent.With respect to the ovarian serous papillary cystadenofibroma, cystectomy should be performed after puberty to prevent the risk of tumor development in the ovaries.The clinicopathological results support the notions that insulin may play a critical role in tumor development and progression.
ACKNOWLEDGEMENTS
We would like to thank all of the patient, doctors, nurses, and technicians involved at our center for their dedication to the study.
杂志排行

World Journal of Clinical Cases的其它文章
- Impacts and challenges of United States medical students during the COVID-19 pandemic
- Recent advances in the management of gastrointestinal stromal tumor
- Medical research during the COVID-19 pandemic
- Progress of intravoxel incoherent motion diffusion-weighted imaging in liver diseases
- Typical and atypical COVID-19 computed tomography findings
- Review of possible psychological impacts of COVID-19 on frontline medical staff and reduction strategies