Campylobacter jejuni enterocolitis presenting with testicular pain:A case report
2020-09-10MasahiroSanagawaTsuneakiKenzakaSayakaKatoIchikoYamaokaShouichiFujimoto
Masahiro Sanagawa, Tsuneaki Kenzaka, Sayaka Kato, Ichiko Yamaoka, Shouichi Fujimoto
Masahiro Sanagawa, Sayaka Kato, Department of Internal Medicine, Miyazaki Seikyo Hospital,Miyazaki 880-0824, Japan
Tsuneaki Kenzaka, Department of Internal Medicine, Hyogo Prefectural Tamba Medical Center,Hyogo 669-3495, Japan
Tsuneaki Kenzaka, Division of Community Medicine and Career Development, Kobe University Graduate School of Medicine, Hyogo 652-0032, Japan
Ichiko Yamaoka, Department of General Surgery, Miyazaki Seikyo Hospital, Miyazaki 880-0824, Japan
Shouichi Fujimoto, Department of Hemovascular Medicine and Artificial Organs, Faculty of Medicine, University of Miyazaki, Miyazaki 889-1692, Japan
Abstract
Key words:Campylobacter;Colitis;Testicular pain;Ileocecal inflammation;Related pain;Case report
INTRODUCTION
Campylobacter jejuniis the most common bacterial enteropathogen, and infections with this organism are typically accompanied by abdominal pain, vomiting, diarrhea, and fever.In contrast,Campylobactercolitis has been reported to cause various extraintestinal symptoms[1].Approximately 40% of patients withCampylobactercolitis present with musculoskeletal symptoms, 15% present with ocular symptoms, and 17%present with urinary tract symptoms.Urinary tract symptoms can include urethral inflammation, which may cause frequent urination and pain during urination[1].In this report, we document a case whereCampylobactercolitis was accompanied by testicular pain.
CASE PRESENTATION
Chief complaint
A 51-year-old man presented to our hospital with bilateral testicular pain.
History of present illness
He had eaten raw chicken (sashimi, in Japanese) a few days before the onset of his symptoms.The testicular pain onset was gradual, beginning in the morning prior to his visiting the hospital.Throughout the day, his testicular pain had spread to his entire back and abdomen and had increased in intensity, leading him to visit our hospital that evening.He also experienced fever, headache, and general joint pain, but no nausea or diarrhea.
History of past illness
The patient did not have a history of significant past illnesses.
Physical examination
Physical examination revealed a body temperature of 38.1 °C, a heart rate of 109 beats/min, a blood pressure of 138/76 mmHg, and a respiratory rate of 20 breaths/min.He exhibited mild tenderness over a wide area, which centered in his right lower abdomen.However, his scrotum did not exhibit any abnormal findings,such as redness, swelling, warmth, or tenderness.
Laboratory examinations
Blood tests showed slight increases in his white blood cell count [12360 cells/µL,(neutrophils:81.9%)] and C-reactive protein level (1.26 mg/L);no abnormalities were detected in the patient’s urinalysis.
Imaging examinations
Abdominal computed tomography imaging revealed thickening of the ileocecal walls(Figure 1), but his scrotal area appeared normal (Figure 2).
FINAL DIAGNOSIS
Campylobactercolitis.
TREATMENT
The patient was hospitalized and treated with fasting, fluid replacement, and 1 g of ceftriaxone, administered intravenously every 24 h.On the night of his admission, he developed watery diarrhea;a stool sample was submitted for culturing.
OUTCOME AND FOLLOW-UP
His fever and testicular pain resolved on post-admission day 3;he was discharged on day 6.After discharge, his stool culture results were reported and revealed the presence ofC.jejuni, confirming theCampylobactercolitis diagnosis;his urine culture was negative for the presence of bacteria.
DISCUSSION
Here, we report, to the best of our knowledge, the first case ofCampylobactercolitis accompanied by testicular pain.Clinicians should be particularly aware of the fact thatCampylobactercolitis often presents with extraintestinal symptoms[1].The more common symptoms of the disease include abdominal pain, vomiting, diarrhea, and fever.In addition, about 40% of patients present with musculoskeletal symptoms,which may include Reiter's syndrome-like arthritis[1].Further, patients may manifest both eye and urinary tract symptoms[1].The urinary tract symptoms, caused by urethral inflammation, include increased urinary frequency and dysuria[1];however,previous reports have not suggested that this inflammation induces testicular pain.
The differential diagnosis for testicular pain includes testicular torsion,epididymitis/orchitis, testicular infarction, and scrotal edema[2].In addition, a few reports have documented testicular pain associated with appendicitis[3-5], but none have reported testicular pain associated with ileocecal inflammation.The testicular pain associated with appendicitis is thought to be related to the tenth thoracic spinal nerve, which innervates both the appendix and the testes[6].In the present patient,because ileocecal inflammation is a hallmark ofCampylobactercolitis, the inflammation may have spread from the ileocecal region to the appendix.
Given the absence of physical findings, such as scrotal tenderness, and the normal urinalysis results, we surmise that the patient’s testicular pain was caused by inflammation of the appendix.This hypothesis is supported by the simultaneous resolution of the testicular pain and the resolution of his colitis symptoms, which included fever, abdominal pain, and diarrhea.The testicular pain appeared as an early symptom, before the onset of diarrhea.This is similar to the onset of appendicitis,which may include related (indirect) epigastric and/or testicular pain.Campylobactercolitis is often preceded by extraintestinal symptoms, such as fever and headache, and the onset of diarrhea is often delayed.The inflammation that is often present in the ileocecal area is presumed to cause the delayed onset of diarrhea[7].In the present patient, the reported testicular symptoms were bilateral, but the location of the pain may have been unclear because it was related, rather than direct, pain.
CONCLUSION
This is the first report of testicular pain associated withCampylobactercolitis.Given thatCampylobactercolitis causes ileocecal inflammation, our case suggests that ileocecal inflammation may indirectly cause testicular pain.Thus, ileocecal inflammation should be considered in the differential diagnosis of patients with testicular pain.
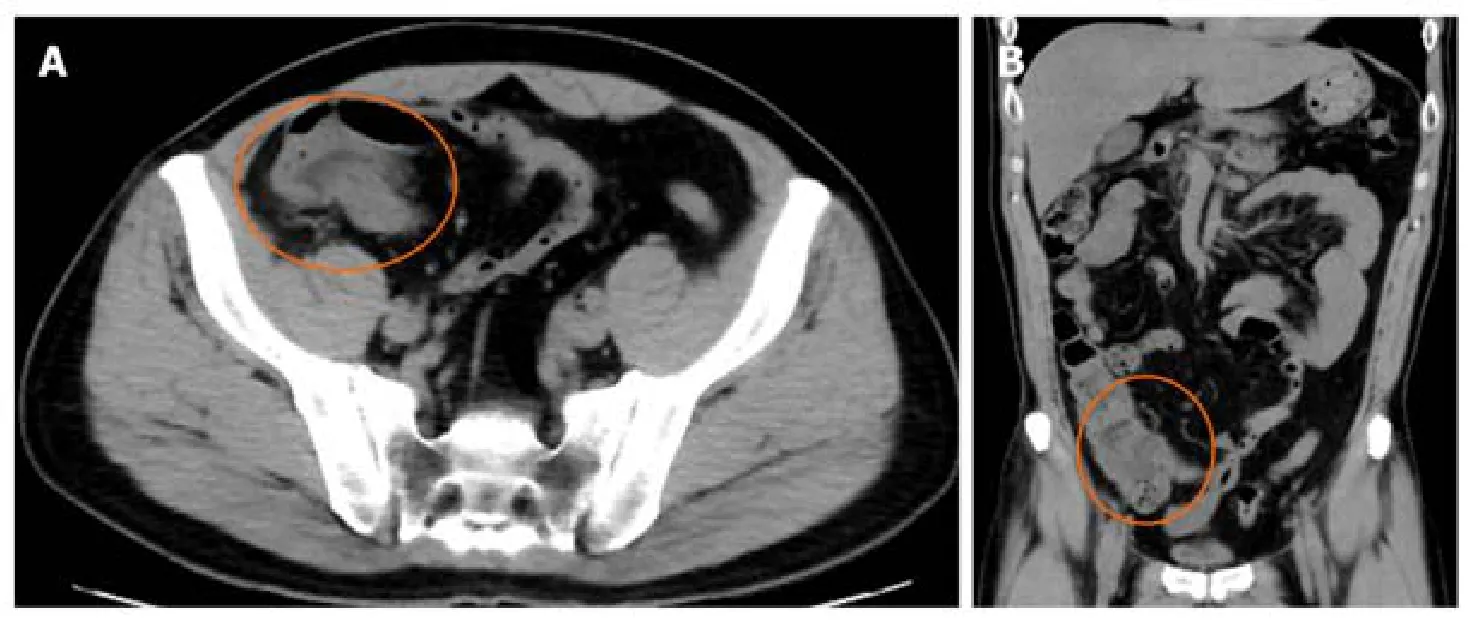
Figure 1 Computed tomography scans of the abdomen.
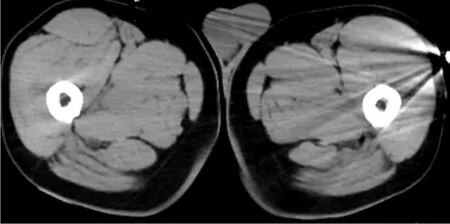
Figure 2 Computed tomography scans of the scrotum.
杂志排行

World Journal of Clinical Cases的其它文章
- Impacts and challenges of United States medical students during the COVID-19 pandemic
- Recent advances in the management of gastrointestinal stromal tumor
- Medical research during the COVID-19 pandemic
- Progress of intravoxel incoherent motion diffusion-weighted imaging in liver diseases
- Typical and atypical COVID-19 computed tomography findings
- Review of possible psychological impacts of COVID-19 on frontline medical staff and reduction strategies