Serum ceruloplasmin can predict liver fibrosis in hepatitis B virusinfected patients
2020-08-24NaLingKangJieMinZhangMengXinLinXuDongChenZuXiongHuangYueYongZhuYuRuiLiuDaWuZeng
Na-Ling Kang, Jie-Min Zhang, Meng-Xin Lin, Xu-Dong Chen, Zu-Xiong Huang, Yue-Yong Zhu, Yu-Rui Liu, Da-Wu Zeng
Abstract
Key words: Ceruloplasmin; Liver fibrosis; Chronic hepatitis B infection; Serum alanine aminotransferase; Noninvasive model; Receiver-operating characteristic
INTRODUCTION
Approximately 292 million people have experienced hepatitis B virus (HBV) infection worldwide; nonetheless, less than 5% of those infected received antiviral therapy[1]. Chronic HBV infection can cause fibrosis, which can eventually develop into hepatocellular carcinoma[2]. Therefore, timely diagnosis of liver fibrosis is instrumental for commencing anti-HBV treatment, which will ultimately control the progression of liver injury and improve the patient prognosis[3]. Assessment of serum alanine aminotransferase (ALT) level is a relatively inexpensive biochemical test that is widely used to detect liver injury. However, recent evidence suggests that some patients with normal ALT can also suffer from severe liver fibrosis[4-6].
Published guidelines for HBV management recommend that antiviral therapy be offered to chronic HBV-infected individuals with persistently normal ALT (PNALT) upon significant histological alterations[7-9]. Liver biopsy (LB) is a standard procedure in diagnosing hepatic fibrosis; however, its invasiveness increases the risk of complications[10-12]. FibroScan is another feasible alternative to LB due to its excellent diagnostic value in liver fibrosis[13-15]. However, its high cost and limitations in immune-tolerant HBV-infected individuals hinder its wide clinical application. The aspartate aminotransferase (AST)-to-platelet (PLT) ratio index (APRI) and fibrosis-4 score (FIB-4) have been recommended as noninvasive predictive indexes to assess liver fibrosis[16]. However, recent research showed that APRI and FIB-4 had poor diagnostic value for assessing the improvement of liver fibrosis during anti-HBV therapy[17]. Further, APRI and FIB-4 could not precisely estimate the stages of fibrosis in HBVinfected individuals with PNALT[18]. Therefore, it is essential to develop a novel predictive index to diagnose hepatic fibrosis in HBV-infected individuals with PNALT.
Serum ceruloplasmin (CP), a glycoprotein secreted by hepatocytes, carries more than 95% of the circulating copper in a healthy human. Studies have shown that CP has a strong antioxidant function and suppresses lipid peroxidation by eliminating superoxide anions[19,20]. Further, abnormal CP levels have been implicated in other pathological conditions[21]. Our previous data showed that CP was negatively correlated with liver fibrosis, suggesting that CP is a useful marker to diagnose liver fibrosis in CHB individuals[22-24]. Nonetheless, the association between CP and hepatic fibrosis among HBV-infected individuals with PNALT remains poorly understood[23]. Therefore, our purpose was to develop a novel panel to noninvasively predict hepatic fibrosis among HBV-infected individuals with PNALT using the CP levels. For this purpose, we routinely collected clinical data in a multicenter and cross-sectional study to develop such a model [ceruloplasmin hepatitis B virus (CPHBV)]. Next, we compared the diagnostic value of the new panel with that of previously established parameters like APRI, FIB-4, the gamma-glutamyl transpeptidase-to-PLT ratio (GPR), S-index, and Forn’s index[25-29].
MATERIALS AND METHODS
Study population
Two hundred and seventy-five HBV-infected individuals with PNALT were retrospectively assessed between June 2010 and November 2019 from three affiliated hospitals of Fujian Medical University [First Affiliated Hospital, Mengchao Hepatobiliary Hospital (Xihong Branch of the First Affiliated Hospital), and The First Hospital of Quanzhou]. A portion of our patient cohort was previously investigated in former studies. In particular, 15.1% of the patients were investigated in Zenget al[22], 2013 and 31.1% of the patients were investigated in Zenget al[23], 2016. All treatmentnaive patients had been HBsAg-positive for more than 6 mo. All exclusion criteria presented in our previous paper were applied in this study[23]. All individuals were randomly stratified into a training and validation group. This study was approved by the Institutional Review Board of Fujian Medical University, and the need for informed consent was waived due to the retrospective nature of the study.
Quantification of liver fibrosis
Liver specimens were obtained using 16-gauge modified aspiration needles (TSK Laboratory, Tochigi, Japan). Qualified liver specimens (a length of more than 1.5 cm and 6 portal tracts) were obtained, fixed in 4% formalin, embedded in paraffin, and processed with hematoxylin-eosin-safran, and Masson’s trichrome according to the standard protocols. Liver fibrosis staging (F0-F4) was carried out according to the METAVIR scoring system by a pathologist blinded to the patients’ data. Significant fibrosis was defined as F ≥ 2, advanced fibrosis as F ≥ 3, and cirrhosis as F = 4, as detailed previously[30].
Serum CP and other clinical parameters
The serum CP was examined by use of the nephelometric immunoassay kit (BN II System, Siemens Healthcare Diagnostics GmbH, Eschborn, Germany). Quantitative HBsAg was tested by use of the Elecsys HBsAg II quant assay (Roche Diagnostics, Mannheim, Germany) or the Abbott ARCHITECT assay (Abbott Laboratories, Chicago), and HBV-DNA was examined by use of quantitative polymerase chain reaction assay (PG Co, Shenzhen, China). Other routine biochemical parameters were assayed using an automatic biochemistry analyzer. Laboratory tests were assessed 1 wk prior to the LB procedure.
Statistical analysis
The Student’st-test was utilized to investigate differences in continuous variables with a normal distribution. We performed the Mann–Whitney test to investigate the differences in continuous variables with a non-normal distribution. The chi-square test was used to detect differences in categorical data. The Spearman test for correlation analyses was applied. Univariate and multivariate regression analyses were applied to select independent parameters linked with significant liver fibrosis. Receiver operating characteristic curve analysis was carried out to obtain the best cut-off value of CP for liver fibrosis. Diagnostic accuracy was obtained by the area under the curve (AUC). To compare the AUC of CPHBV with that of five noninvasive models (APRI, FIB-4, GPR, Forn’s index, and S index), theZtest was applied. Statistical analyses were applied by use of SPSS v23.0.
RESULTS
Demographic and clinical characteristics
Among a total of 275 enrolled patients (mean age = 40.25 ± 9.65 years), 194 (70.5%) were men and 81 (29.5%) were women (Table 1). Further, 54.5% of the patients presented with at least moderate fibrosis (F ≥ 2) and 19.3% had liver cirrhosis (F4). Analysis of the demographic and clinical features did not reveal significant differences between the training and validation groups (P> 0.05, Table 1).
Diagnostic value of CP for detecting different stages of liver fibrosis among HBVinfected individuals with PNALT
Serum CP levels revealed an inverse correlation with hepatic fibrosis (r= -0.6). The AUCs were 0.774 for F ≥ 2, 0.812 for F ≥ 3, and 0.853 for F4 (Table 2). Further, the best diagnostic CP values were 203.5 mg/L for F ≥ 2, 190.5 mg/L for F ≥ 3, and 182.5 mg/L for F4 (Table 2).
Development of a novel panel for liver fibrosis
Next, we analyzed the correlation between various biochemical parameters and significant fibrosis (Table 3). Univariate analysis revealed that the CP, albumin, gamma glutamyl transpeptidase, total cholesterol, cholinesterase, HBsAg, and PLT levels were different between individuals with non-significant and significant fibrosis (P< 0.05). These variables were then subjected to multivariate regression. CP, PLT, and HBsAg were identified as independent predictors. Using these parameters, a novel diagnostic model named CPHBV was developed to evaluate significant fibrosis in HBV-infected individuals with PNALT as follows: 37.122-10.072 × log CP (mg/L) - 4.291 × log PLT (109/L) - 0.958 × log HBsAg (IU/mL).
Accuracy of the new index in assessment of F ≥ 2, F ≥ 3, and F4
We then analyzed the diagnostic value of the CPHBV model for detecting F ≥ 2, F ≥ 3, and F4 (Table 4). The AUC of CPHBV for predicting F ≥ 2 was 0.842. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were 81.1%, 71.9%, 76.9%, and 76.7%, respectively, in the training group, and 72.4%, 80.3%, 82.1%, and 70.0% in the validation group. The AUC of CPHBV for the evaluation of significant fibrosis showed a comparable predictive value between the training and validation groups (Z = 0.746,P= 0.46). Upon using our model to assess advanced fibrosis and cirrhosis, the AUC, sensitivity, specificity, PPV, and NPV were 0.92, 90.9%, 78.7%, 66.7%, and 94.9%, respectively, for F ≥ 3, and 0.904, 96.2%, 71.4%, 43.9%, and 98.8% for F4 in the training group (Table 4).
Comparison of CPHBV with other noninvasive models
We compared the AUCs among six panels for the evaluation of significant fibrosis (Table 5, Figure 1). The CPHBV model had a significantly higher AUC value for significant fibrosis in HBV-infected individuals with PNALT than APRI, FIB-4, GPR, Forn’s index, and S-index (Table 5).
DISCUSSION
We previously demonstrated that serum CP was a potential biomarker to predict hepatic fibrosis in HBV-infected individuals[22,23]. In this multi-center study, we further confirmed the valuable role of CP as a strong indicator to assess hepatic fibrosis in HBV-infected individuals with PNALT. In particular, our results demonstrated that serum CP had an inverse correlation with liver fibrosis. Therefore, we were able to develop the CPHBV index to predict different stages of fibrosis (i.e., significant,advanced, and cirrhosis). Further, we validated the specificity and sensitivity of the CPHBV model and compared its prognostic value to that of previously established models. Remarkably, the newly developed CPHBV model had a significantly better predictive value for significant fibrosis than the APRI, FIB-4, and GPR, scores as well as Forn’s index and the S-index. To our knowledge, this is the first effort to developsuch a model and validate its valuable role for assessing significant fibrosis in HBVinfected individuals with PNALT.

Table 1 Demographic characteristics and clinical features in our patient cohort

Table 2 Accuracy of serum ceruloplasmin in diagnosing F ≥ 2, F ≥ 3, and F = 4 as measured by area under the receiver operating characteristic curve (n = 138)

Table 3 Clinical parameters associated with significant fibrosis in the training group (138 patients)

Table 4 Diagnostic value of ceruloplasmin hepatitis B virus in the training and validation groups
ALT is a valuable biomarker for the detection of hepatic damage,i.e., normal serum ALT typically indicates the absence of liver injury. However, this is not the case in chronic HBV patients with PNALT. Previous studies demonstrated that more than 30% of HBV-infected individuals with PNALT present with significant liver fibrosis[31,32]. Indeed, our results demonstrated that 54.5% of HBV-infected individualswith PNALT had significant fibrosis, and their CP levels had an inverse correlation with hepatic fibrosis. In addition, multivariate analyses identified CP, HBsAg, and PLT as potential biomarkers that were independently correlated to liver fibrosis. In HBV-infected individuals with PNALT, analysis of the AUCs indicated that the serum CP had a reasonable diagnostic value to assess F ≥ 2, F ≥ 3, and F4. These results were in accordance with previous studies that suggested the potential function of CP for diagnosing fibrosis among HBV-infected individuals[22,23]. The detection of PLT levels has repeatedly been used to predict liver fibrosis[33]. Further, our previous research demonstrated that quantitative measurement of the HBsAg level can distinguish patients with active liver injury from immune tolerant HBV-infected individuals[34]. Although the mechanisms underlying the negative correlation between the serum HBsAg and fibrosis stages remain unclear, it is reasonable to speculate that host immune responses to HBV may result in liver damage, which can lead to a reduction in the HBsAg level. Taken together, our study enabled the identification of three serum biomarkers that were negatively associated with liver fibrosis, which enabled us to develop the CPHBV model.
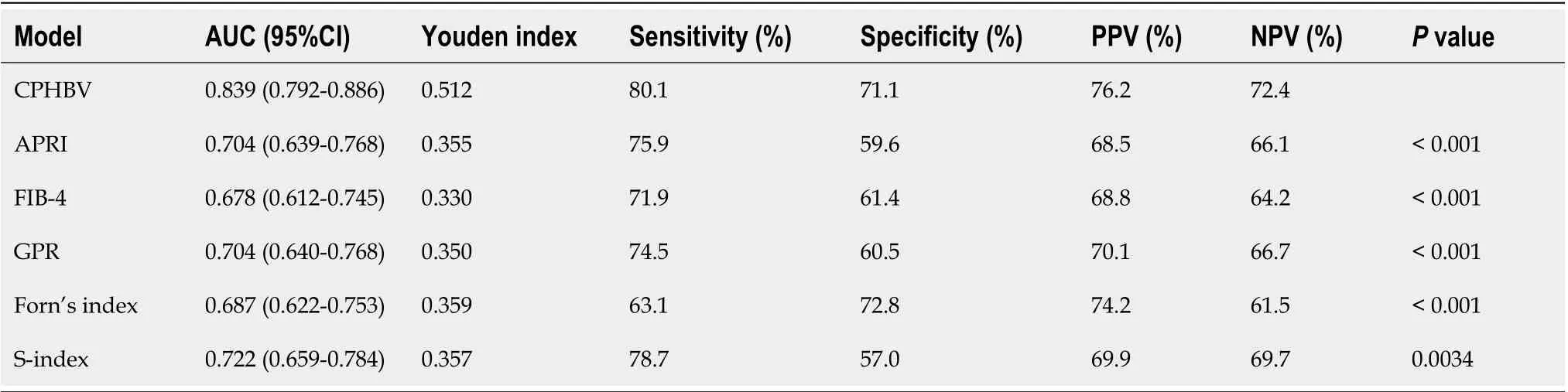
Table 5 Comparisons of ceruloplasmin hepatitis B virus with other predictive models for assessing F ≥ 2 (n = 275)
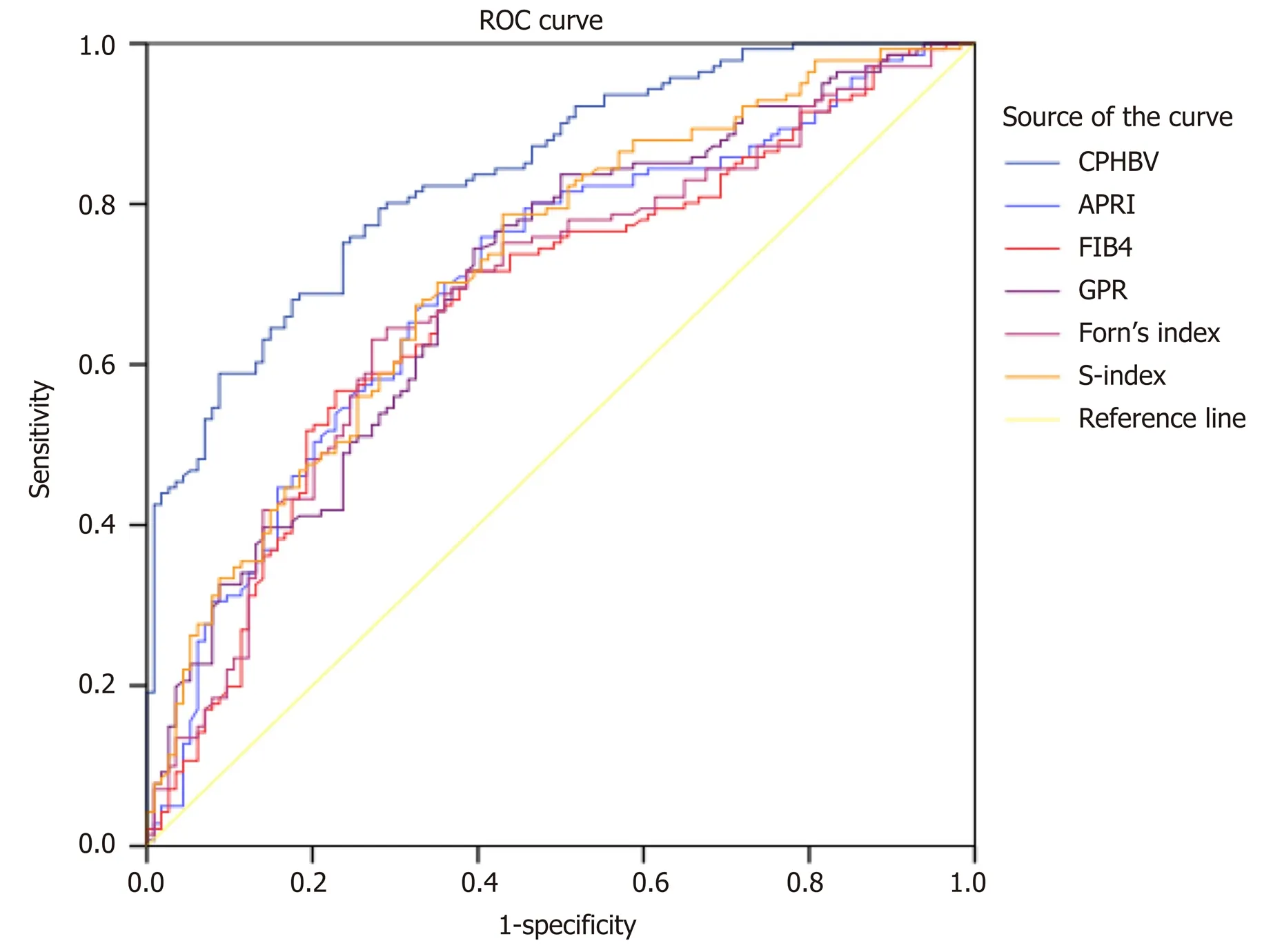
Figure 1 Receiver operating characteristic curves for the noninvasive models in all the study subjects. CPHBV: Ceruloplasmin hepatitis B virus; APRI: Aspartate aminotransferase-to-platelet ratio index; FIB-4: Fibrosis-4; GPR: Gamma-glutamyl transpeptidase-to-platelet ratio.
The CPHBV model consists of three routinely assessed and relatively inexpensive biochemical parameters (CP, HBsAg, and PLT), which can be beneficial for resourcelimited institutions to accurately detect liver fibrosis. CPHBV enabled the correct identification of patients with significant fibrosis and cirrhosis with an area under the receiver operating characteristic curve of 0.842 and 0.920, respectively. A CPHBV value less than 0.034 had an NPV of 76.7% to exclude significant fibrosis with a sensitivity of 81.1%. Among the 64 patients who did not have significant fibrosis, 18 (28.1%) will present with a CPHBV value higher than 0.0304. For patients with a score below 0.553, 80 (98.8%) out of 81 patients will not develop cirrhosis. Applying a higher cutoff value of 0.553, 32 (28.6%) of 112 without cirrhosis would be classified incorrectly (Supplementary Table 1 and 2). So, our study showed that the use of the CPHBV model will enable the accurate determination of patients in urgent need of antiviral treatment. Although this novel model was developed to diagnose significant fibrosis, it can also be used for diagnosing advanced fibrosis and cirrhosis.
Numerous novel noninvasive models to diagnose liver fibrosis have emerged. The APRI and FIB-4 scores were recommended to evaluate hepatic fibrosis by the HBV practice clinical guidelines. However, recent research showed that APRI and FIB-4 had low predictive performance in chronic HBV patients with PNALT (AUCs of 0.518 and 0.597, respectively)[18]. In this study, the AUC of FIB-4 or APRI for F ≥ 2 in HBVinfected individuals with PNALT was lower than that for the CPHBV model (P< 0.001). GPR is another novel predictive index for significant fibrosis in HBV-infected patients in the West African population[27]. GPR was found to be useful in our Chinese patient cohort but the predictive value of the novel CPHBV panel significantly surpassed that of GPR. Forn’s index was applied to diagnose liver fibrosis in CHB individuals[35]. However, the diagnostic value of Forn’s index for significant fibrosis in HBV-infected individuals with PNALT was rather limited (AUC = 0.687). The S-index was specifically designed to assess significant fibrosis in CHB individuals and had superior diagnostic accuracy compared to the APRI and FIB-4[36]. Nevertheless, CPHBV was superior to the S index in our patient cohort (0.839vs0.722, P = 0.0034). Taken together, the newly developed CPHBV model had better performance in identifying significant fibrosis than APRI, FIB-4, GPR, Forn’s index, and S index, at least in our patient cohort.
This study had a few limitations. First, CPHBV was developed and evaluated in a multicenter cross-sectional study. Therefore, future prospective multicenter studies will be needed to verify the diagnostic value of CPHBV. Second, we used cutoff ALT values < 40 IU/mL as the upper limit of normal for ALT in this study. However, in accordance with the current guidelines, ALT is estimated to be 35 IU/mL in healthy men and 25 IU/mL in healthy women[7]. Third, we used CP values tested at one time point to construct our model. Future studies should follow up with the participants to validate our results at different time points. Fourth, transient elastography (Fibroscan), the enhanced liver fibrosis test, and Wisteria floribunda agglutinin-positive Mac-2 binding protein(WFA + -M2BP) were as well accurate diagnostic tests for monitoring regression of fibrosis in patients with chronic HBV infection[37-41]. However, we did not perform the comparison because of the unavailable equipment at the time of data collection and serum indicators, such as hyaluronic acid, procollagen III aminoterminal peptide, metalloproteinase 1, and WFA + -M2BP are not routinely tested in our hospital.
In conclusion, serum CP is a routinely investigated biochemical index that negatively correlates with hepatic fibrosis and a potential marker to diagnose liver fibrosis in HBV-infected individuals with PNALT. The CPHBV model was found to be more efficient than the previously reported noninvasive models in diagnosing significant fibrosis among HBV-infected individuals with PNALT. The use of CPHBV might reduce the clinical need for LB in the future.
ARTICLE HIGHLIGHTS
Research background
Chronic hepatitis B virus (HBV)-infected individuals with persistently normal serum ALT (PNALT) levels can suffer from severe liver fibrosis. Therefore, those patients can be prioritized in commencing the antiviral therapy. The timely diagnosis of liver fibrosis and initiation of anti-HBV treatment can control the disease progression and improve the patient prognosis. Serum ceruloplasmin (CP) is negatively correlated with liver fibrosis and thus it may serve as a predictive marker for liver fibrosis among HBV-infected individuals with PNALT.
Research motivation
Our previous data demonstrated that CP was negatively correlated with liver fibrosis in CHB individuals. Nonetheless, the association between CP and hepatic fibrosis among HBV-infected individuals with PNALT remains poorly understood.
Research objectives
We aimed to develop a predictive model combining serum CP to predict hepatic fibrosis among HBV-infected individuals with PNALT.
Research methods
Two hundred and seventy-five HBV-infected individuals with PNALT were retrospectively assessed between June 2010 and November 2019 from three affiliated hospitals of Fujian Medical University [First Affiliated Hospital, Mengchao Hepatobiliary Hospital, and The First Hospital of Quanzhou]. The association between CP and fibrotic stages was statistically analyzed. A predictive index that included CP was constructed to predict significant fibrosis and compared to previously established parameters like the aspartate aminotransferase (AST)-to-platelet (PLT) ratio index (APRI), Fibrosis-4 score (FIB-4), gamma-glutamyl transpeptidase-to-PLT ratio (GPR), Forn’s score, and S-index.
Research results
We found that serum CP had an inverse correlation with liver fibrosis among HBVinfected individuals with PNALT. The CPHBV model was developed using CP, PLT, and HBsAg levels to predict various stages of fibrosis among HBV-infected individuals with PNALT. CPHBV was superior to previously reported models like APRI, FIB-4, GPR, Forn’s index, and S index.
Research conclusions
Serum CP is a routinely investigated biochemical parameter that negatively correlates with hepatic fibrosis and can be a potential marker to diagnose liver fibrosis in HBVinfected individuals with PNALT. The CPHBV model could accurately predict liver fibrosis in HBV-infected individuals with PNALT. Therefore, CPHBV may efficiently predict liver fibrosis, which can reduce the need for liver biopsy before commencing antiviral treatment.
Research perspectives
CPHBV was developed and evaluated in this multicenter cross-sectional study, thus providing a solid foundation for future prospective studies to validate the diagnostic value of this model.
杂志排行

World Journal of Gastroenterology的其它文章
- Histopathological landscape of rare oesophageal neoplasms
- Details determining the success in establishing a mouse orthotopic liver transplantation model
- Modified percutaneous transhepatic papillary balloon dilation for patients with refractory hepatolithiasis
- Acceptance on colorectal cancer screening upper age limit in South Korea
- Transarterial chemoembolization with hepatic arterial infusion chemotherapy plus S-1 for hepatocellular carcinoma
- Intestinal NK/T cell lymphoma: A case report