Mediastinoscopic esophagectomy with lymph node dissection using a bilateral transcervical and transhiatal pneumomediastinal approach
2020-08-02YutakaTokairinYasuakiNakajimaKenroKawadAkihiroHoshinTakuyaOkadaToshihiroMatsuiKazuyaYamaguchiKagamiNagaiYusukeKinugasa
Yutaka Tokairin, Yasuaki Nakajima, Kenro Kawad, Akihiro Hoshin, Takuya Okada, Toshihiro Matsui, Kazuya Yamaguchi, Kagami Nagai, Yusuke Kinugasa
1Department of Surgery, Toshima Hospital Tokyo Metropolitan Health and Hospitals Corporation, Tokyo 173-0015, Japan.
2Department of Gastrointestinal Surgery, Tokyo Medical and Dental University, Tokyo 113-8510, Japan.
Abstract We developed a method for mediastinoscopic esophagectomy via a bilateral transcervical and transhiatal approach under pneumomediastinum as a less-invasive radical operation. The right recurrent nerve is first identified using an open approach, and the right cervical paraesophageal lymph nodes and part of the right recurrent nerve lymph nodes are dissected, after which pneumomediastinum is initiated. The upper thoracic paraesophageal lymph nodes and right recurrent nerve lymph nodes are dissected along the right vagus nerve. The dorsal side of the esophagus is dissected along the visceral sheath taking care to avoid thoracic duct injury and is then dissected along the vascular sheath in front of the descending aorta. The esophagus is dissected from the trachea at the caudal side of the aortic arch, and then dissected along the ventral side of the left main bronchus,reaching the pulmonary artery. Finally, the right recurrent nerve lymph nodes around the right subclavian artery are completely retrieved. The left cervical approach is almost the same as that via the right side. The dorsal side of the esophagus is almost dissected along the visceral sheath with a right transcervical approach. The subaortic arch to the left tracheobronchial lymph nodes are dissected using the crossover technique. These lymph nodes are easily dissected by cutting the left and ventral side of the lymph nodes because the caudal side is already dissected in the right transcervical approach. A bilateral (especially right trans-cervico-pneumomediastinal) approach is useful for bilateral upper mediastinal lymph node dissection and esophagectomy.
Keywords: Minimally invasive esophagectomy, cervical approach, esophageal cancer, mediastinoscopic esophagectomy, pneumomediastinum, mediastinoscopic esophagectomy with lymph node dissection
INTRODUCTION
Conventional radical esophagectomy through right thoracotomy is one of the most invasive procedures. It is important to reduce the invasiveness of this procedure.
Conventional radical esophagectomy was previously performed for the treatment of mucosal esophageal cancers for patients diagnosed with not only advanced esophageal cancer but also T1a N0 M0 cStage I according to the Union for International Cancer Control TNM Classification (eighth edition)[1]; however,endoscopic submucosal dissection has come to be performed for patients with T1a N0 M0 cStage I as minimally invasive treatment and the methods have been well established[2].
On the other hand, the esophagectomy with dissection of the mediastinal and abdominal lymph nodes is needed for the treatment of thoracic esophageal cancer with invasion of the submucosal layer or deeper layers. For the abovementioned reason, hybrid surgery consisting of a two-field abdominal-thoracic operation (called the Ivor-Lewis procedure) was developed[3]. In Western countries, abdominal esophageal cancer and esophagogastric junctional cancers are well observed and later histological types are frequently diagnosed as “adenocarcinoma”. Thus, this procedure is considered reasonable because esophageal cancers at these locations are rarely associated with upper mediastinal and cervical lymph node metastasis.Esophageal cancers in the thoracic esophagus are frequently associated with upper mediastinal and cervical lymph node metastasis. Thus, this procedure is not suitable for these esophageal cancers. To resolve this problem, McKeown developed total esophagectomy with three-field lymph node dissection[4].
Currently, radical esophagectomy through right thoracotomy has changed to esophagectomy via a thoracoscopic or laparoscopic approach, including robot assisted surgery, which reduces the invasiveness of the procedure by decreasing the destruction of thoracic and abdominal walls[5-11]. However, this method mandates the use of one-lung ventilation, some destruction of the thoracic wall, or prone positioning.
Conventional transhiatal esophagectomy has been performed and mediastinoscopic esophagectomy has been developed. These procedures are also recognized as types of minimally invasive esophagectomy (MIE)[12-14].However, due to the blind maneuvering in the upper and middle mediastinum that is necessary in this procedure and the difficulty of systematic lymph node dissection, it is usually only applied in limited cases,such as cases of esophagogastric junction cancer, very early-stage cancers, or some cases of advanced thoracic esophageal cancer for the purpose of palliative resection[12].
Recently, we developed and reported the performance of “mediastinoscopic esophagectomy with lymph node dissection (MELD)” under pneumomediastinum using a bilateral transcervical and transhiatal approach, as a method of radical esophagectomy[15-18]. This procedure achieves curative radical esophagectomy with minimal invasiveness. Upper mediastinal lymph node dissection has been performed using bilateral open cervical surgery and a leた transcervical and transhiatal pneumomediastinal approach in some institutions[19,20]. However, in the results of our clinical trial, the right recurrent nerve lymph nodes,the upper thoracic paraesophageal lymph nodes, and the subaortic arch to the leた tracheobronchial lymph nodes could not be completely dissected using the leた transcervical approach alone[17,18]. We are therefore of the opinion that a right cervical pneumomediastinal approach is necessary to achieve the complete dissection of these lymph nodes. We herein describe the surgical technique using a bilateral (especially right cervico-pneumomediastinal) approach.
TECHNIQUE
In the MELD procedure, the right cervical approach is performed first, followed by the left cervical approach and laparoscopic-transhiatal approach.
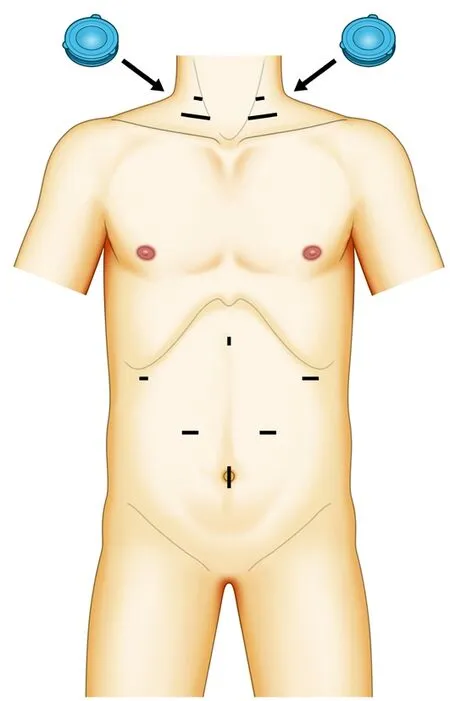
Figure 1. The location of the ports and single-port laparoscopic access devices. This schematic illustration shows single-port laparoscopic access devices in the bilateral cervical area and ports in the abdominal area. A single-port laparoscopic access device with three 5-mm trocars is placed in a triangle configuration. Approximately 3 cm above this device, a 5-mm trocar is inserted as a mediastinoscopic port
Right cervical approach
A right cervical collar incision (approximately 6 cm) is made 3 cm above the right clavicle, and sufficient working space is created between the tracheoesophageal groove and right carotid sheath. The right recurrent nerve is first identified using an open approach and part of the right cervical paraesophageal lymph nodes and the right recurrent nerve lymph nodes between the tracheal wall and the right recurrent nerve are dissected.
After a single-port laparoscopic access device (Lap Protector; Hakko Corporation, Nagano, Japan) is inserted in the wound to exclude the right lobe of the thyroid gland, the cervical wound is sutured over a length of approximately 4 cm. The device is placed at the dorsal side of the sternohyoid and the scapulohyoid muscles at the cranial side, at the inner border of the sternal head of the sternocleidomastoid muscle on the outside, and at the dorsal side of the clavicular head of the sternocleidomastoid muscle on the caudal side. Next, an EZ access (Hakko Corporation, Nagano, Japan), through which three 5-mm trocars are placed in a triangle configuration [Figure 1], is attached. Then, pneumomediastinum (to 8 mmHg) is established with CO2. A 5-mm trocar is inserted as a mediastinoscopic port approximately 3 cm above this device; we can observe the whole forceps movement from the beginning of forceps insertion. A laparoscopic forceps and a LigaSureTMMaryland (Medtronic, Minneapolis, MN) are inserted between the tracheal wall and the internal side of the right recurrent nerve [Figure 2A and B]. The upper thoracic paraesophageal lymph nodes and the right recurrent nerve lymph nodes are dissected along the right vagus nerve with attention paid to avoid injury of the right mediastinal pleura [Figure 3]; then,the proximal portion of the azygos vein and the right bronchial artery are dissected [Figure 4A and B].Next, the dorsal side of the esophagus is dissected along the visceral sheath with attention paid to avoid the injury of the thoracic duct, which is located on the dorsal side of the visceral sheath [Figure 5]. The esophagus is dissected along the vascular sheath in front of the descending aorta, because the visceral sheath becomes unclear on the caudal side of the bifurcation of the trachea [Figure 4 A and B]. During dissection, the proper esophageal artery is double sealed and cut using a LigaSureTMMaryland. Then, the esophagus is dissected from the trachea on the caudal side of the aortic arch. In some cases, the bronchooesophagus muscle is developed and attention should be paid to avoid injury of the membranous portion of the trachea. Next, dissection is performed along the ventral side of the leた main bronchus, reaching to the pulmonary artery, in order to determine the caudal side of the lymph nodes in the subaortic arch to the leた tracheobronchial region, which should be dissected. To make it easy to dissect the leた recurrent nerve lymph nodes, the leた recurrent nerve is exposed in the right transcervical pneumomediastinal approach[Figure 6].
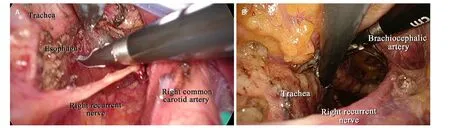
Figure 2. A,B: dissection via a right transcervical approach under pneumomediastinum. The laparoscopic forceps and a vessel sealing system are inserted between the tracheal wall and the internal side of the right recurrent nerve
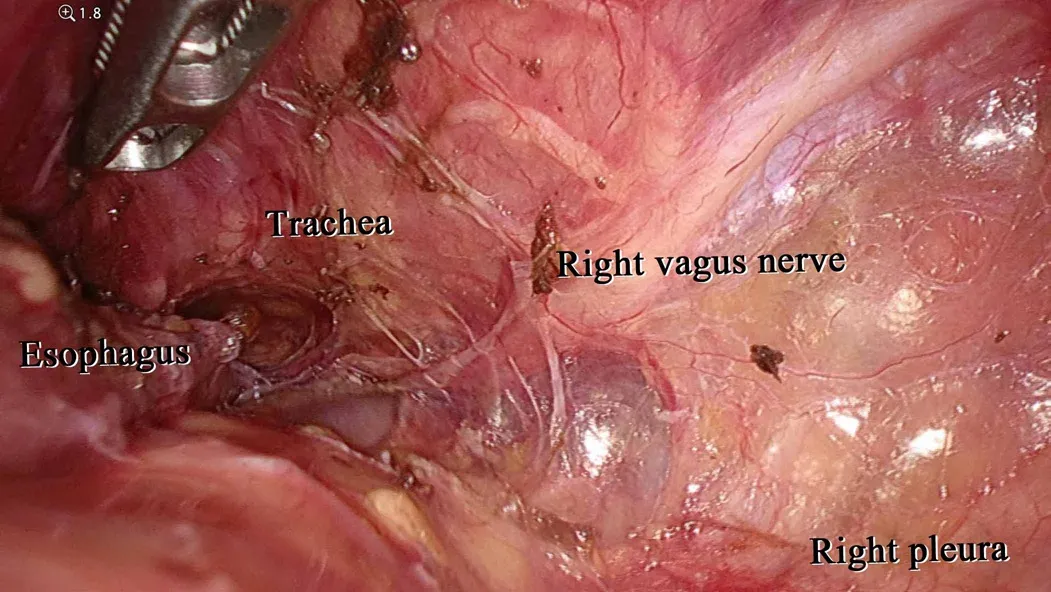
Figure 3. Dissection of the right side of the esophagus via a right transcervical approach under pneumomediastinum. The upper thoracic paraesophageal lymph nodes and right recurrent nerve lymph nodes are dissected along the right vagus nerve with attention paid to avoid injury to the right mediastinal pleura
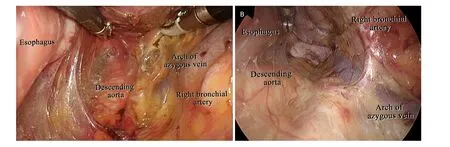
Figure 4. A, B: dissection of the right dorsal side of the esophagus via a right transcervical approach under pneumomediastinum. The proximal portion of the azygos vein and the right bronchial artery is observed along the right mediastinal pleura. The esophagus is dissected along the vascular sheath in front of the descending aorta, because the visceral sheath becomes unclear on the caudal side of the bifurcation of the trachea
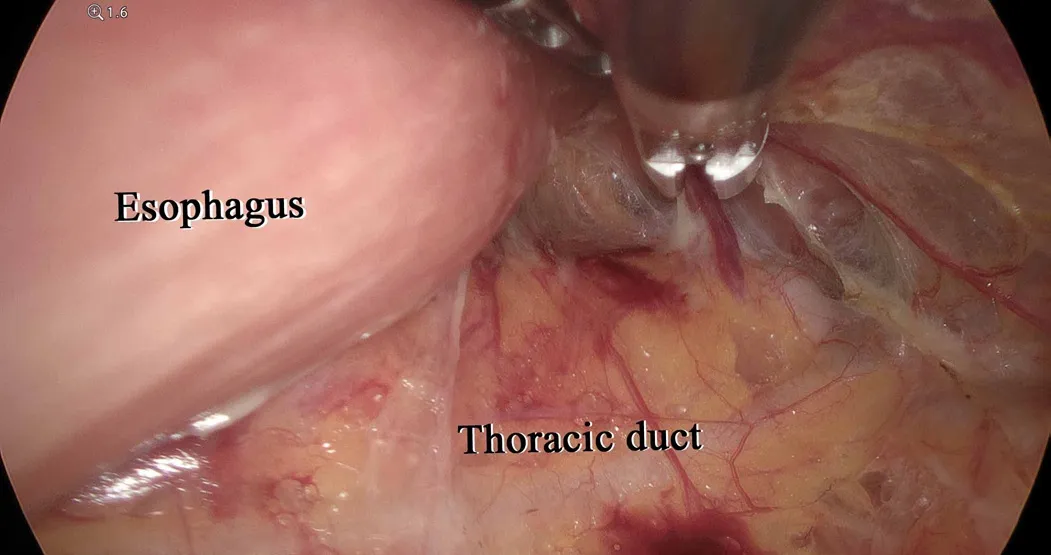
Figure 5. Dissection of the dorsal side of the esophagus via a right transcervical approach under pneumomediastinum. The dorsal side of the esophagus is dissected along the visceral sheath with attention paid to avoid injury to the thoracic duct, which is located on the dorsal side of the visceral sheath
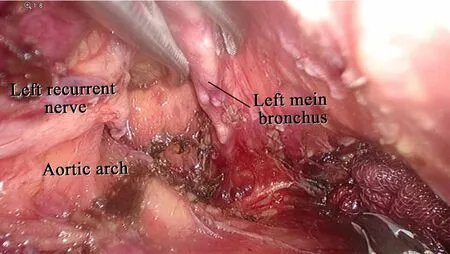
Figure 6. Dissection of the cartilage of the left main bronchus via a right transcervical approach under pneumomediastinum. Dissection of the subaortic arch to the left tracheobronchial lymph nodes is performed along the ventral side of the left main bronchus reaching to the pulmonary artery to determine the caudal side of the lymph nodes in the subaortic arch to the left tracheobronchial region, which should be dissected. To enable the easy dissection of the left recurrent nerve lymph nodes, the left recurrent nerve is exposed via the right transcervical pneumomediastinal approach
Finally, aたer the common carotid artery is pulled outward and the esophagus is pulled to the leた side, the right recurrent nerve lymph nodes around the right subclavian artery are completely retrieved [Figure 7].Under pneumomediastinum, these lymph nodes can be completely dissected.
Left cervical approach
A left cervical collar incision and scope port site are made symmetrically. After identifying the cranial portion of the leた recurrent nerve, which is located on the dorsal side of the inferior part in the leた lobe of thyroid gland, some of the leた cervical paraesophageal lymph nodes and leた recurrent nerve lymph nodes are dissected by the open method.
Aたer a single-port laparoscopic access device is inserted into the wound, the cervical wound is sutured over a length of approximately 4 cm.
The device is placed at the dorsal side of the sternohyoid and the scapulohyoid muscles on the cranial side,at the inner border of the sternal head of the sternocleidomastoid muscle on the outside and at the dorsal side of the clavicular head of the sternocleidomastoid muscle on the caudal side. After attaching an EZ access and inserting a 5-mm trocar as a mediastinoscopic port, leた transcervical pneumomediastinum is applied similarly to the right side. First, the dissected layer on the dorsal side of the esophagus and from the right side is checked and dissection is performed to near the aortic arch with attention paid to avoid injury to the visceral layer. In many cases, the esophagus has already been mostly dissected by the right transcervical approach. Next, the esophagus is dissected from the leた subclavian artery, reaching to the aortic arch.
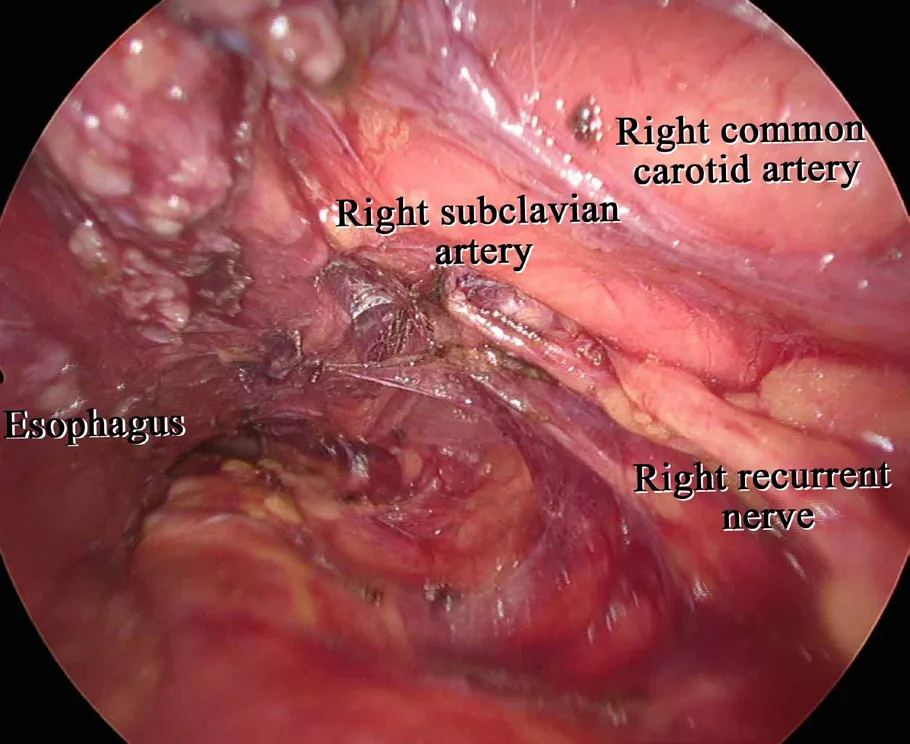
Figure 7. Dissection of the right recurrent nerve lymph nodes via a right transcervical approach under pneumomediastinum. After the right common carotid artery is pulled outward and the esophagus is pulled to the left, the right recurrent nerve lymph nodes around the right subclavian artery are completely retrieved
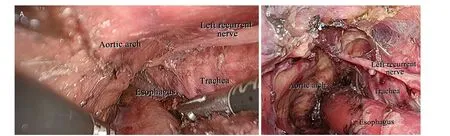
Figure 8. Dissection of the left recurrent nerve lymph nodes via a left transcervical approach under pneumomediastinum. A: the left recurrent nerve lymph nodes are dissected along the dorsal side of the left recurrent nerve; B: the ventral side of the left recurrent nerve lymph nodes are dissected along the left recurrent nerve and the tracheal branch of the left recurrent nerve is preserved as much as possible
The ventral side of the esophagus is dissected from the leた side of the membranous portion of the trachea,the leた main bronchus, and the aortic arch. The leた recurrent nerve lymph nodes are dissected along the dorsal side of the leた recurrent nerve [Figure 8A]. Because of this procedure, the leた recurrent nerve and the ventral side of the leた recurrent nerve lymph nodes are attached to the leた side of the trachea. Because the leた recurrent nerve at the recurrent portion on the aortic arch has already been exposed via the right transcervical approach, the recurrent nerve is easily detected. We think that this method is useful for preventing leた recurrent nerve injury.
Next, the ventral side of the leた recurrent nerve lymph nodes is dissected along the leた recurrent nerve[Figure 8B], and the tracheal branch of the left recurrent nerve is preserved as much as possible[21]. We consider that this method is useful for two reasons: First, appropriate tension can be placed on the left recurrent nerve lymph nodes and the dissection of these lymph nodes can be easily performed because the leた recurrent nerve is attached to the tracheal wall. Second, the branch of the leた recurrent nerve is considered useful for preserving the cough reflex.
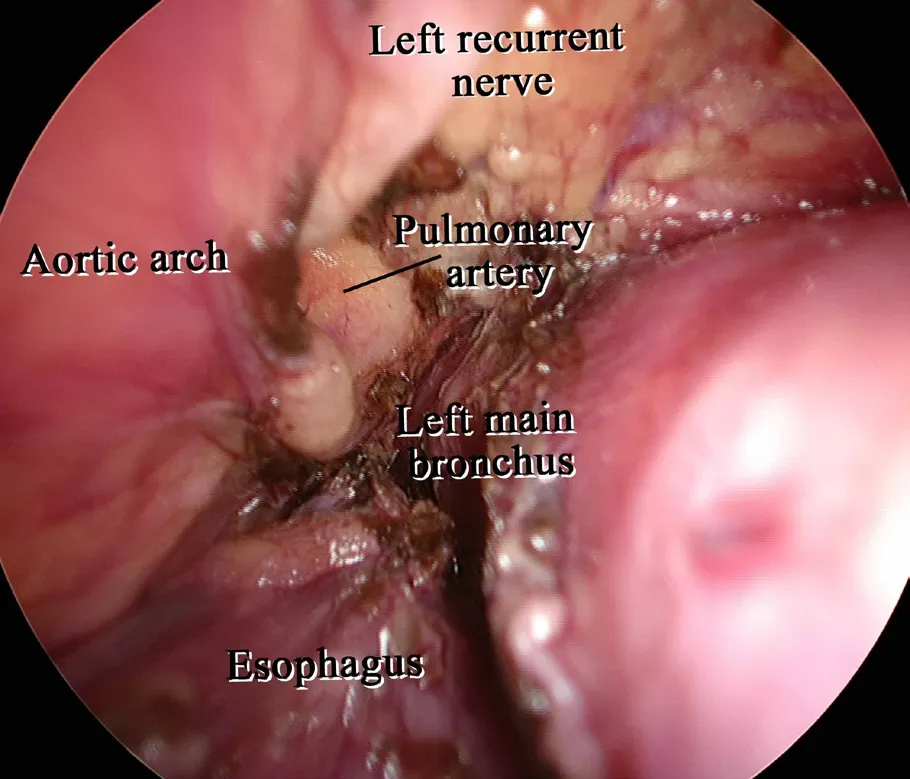
Figure 9. Dissection of the subaortic arch to the left tracheobronchial lymph nodes via a left transcervical approach under pneumomediastinum. These lymph nodes can easily be dissected by cutting only the left and ventral side of these lymph nodes while pulling the esophagus toward the right side because the caudal and dorsal side of these lymph nodes have been already dissected via a right transcervical approach
Dissection of the subaortic arch to the left tracheobronchial lymph nodes
The subaortic arch to the leた tracheobronchial lymph nodes is dissected using the crossover technique, as described previously[15-18]. The crossover technique consists of the transhiatal, right transcervical, and/or leたtranscervical approach and is suitable for dissection in narrow and relatively deep operative fields, as the approach can be made from two directions. We use this technique when dissecting the subaortic arch to the leた tracheobronchial lymph nodes. First, the caudal and dorsal sides of these lymph nodes are dissected via the right transcervical approach. The lymph nodes can then dissected by cutting only their leた and ventral sides with the esophagus pulled toward the right via the leた transcervical approach [Figure 9].
Laparoscopic and transhiatal approach
The ports are located in an inverted trapezoidal shape, as described in Figure 1, in accordance with laparoscopic gastrectomy. Pneumoperitoneum with CO2(to 10 mmHg) is then introduced. After the dissection of the upper abdominal lymph nodes and gastric conduit mobilization, the esophagus is cut at cranial side as much as possible. The suture thread at the cut end of the esophagus is pulled to provide traction for the dissection of the middle to lower mediastinal lymph nodes, including the subcarinal lymph nodes under pneumomediastinum [Figure 10]. In our institute, this is performed using totally endoscopic surgery.We oたen use the ENSEAL® G2 Articulating Tissue Sealer (Ethicon Endo-surgery, Cincinnati, Ohio), which is a curved long bipolar sealer, because the subcarinal nodes are difficult to dissect from abdominal ports.
Range of the operation field in the cervical and transhiatal approach under pneumomediastinum
The dorsal side of the esophagus from the cervical area to near the pulmonary vein is easily dissected via the cervical pneumomediastinal approach. On the other hand, the subcarinal lymph nodes are easily dissected via a transhiatal pneumomediastinal approach rather than a cervical approach. This is for the following reasons. First, these lymph nodes can be easily dissecteden blocwith the esophagus via transhiatal approach but not via a cervical approach. Second, bleeding from the subcarinal lymph nodes connected to the pretracheal lymph nodes cannot be stopped easily via a cervical approach.
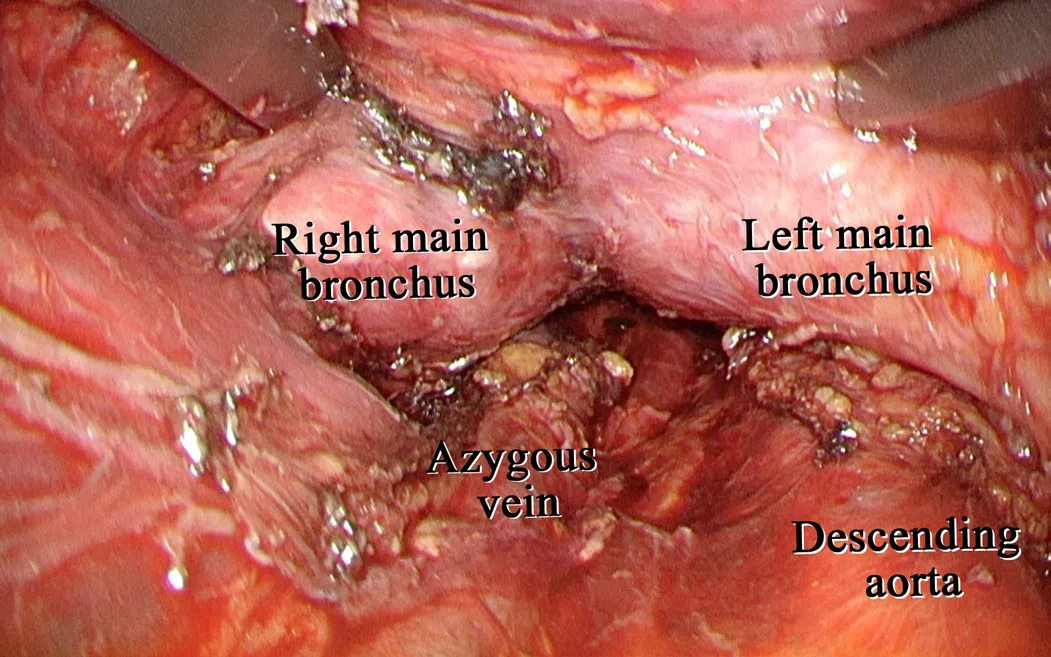
Figure 10. Subcarinal lymph node dissection via a transhiatal approach under pneumomediastinum. The middle to lower mediastinal lymph nodes, including the subcarinal lymph nodes, are dissected under pneumomediastinum via a transhiatal approach
We consider the “crossover technique” to be useful for the dissection of the lymph nodes near the bilateral main bronchus because these lymph nodes are located in the deepest area via both the cervical and transhiatal approaches.
Aたer the pneumomediastinal procedure, the bilateral remnant cervical paraesophageal lymph nodes and supraclavicular lymph nodes are dissected using an open method.
The median total number of dissected lymph nodes in the cervico-mediastinal region identified with a mediastinoscope was 36 (range 22-76) in 10 cases treated using the MELD procedure in our institute.
Postoperative outcomes
This operation using the bilateral cervical approach under pneumomediastinum was performed for 10 cases. The median mediastinoscopic operation time was 312 (299-336) mins and the median blood loss was 476 (203-667) mL. The median postoperative stay was 15.5 (14.0-16.8) days.
DISCUSSION
The MELD procedure is considered to have several advantages over other approaches. First, this procedure does not require one-lung ventilation or a prone position. Second, this procedure requires only bi-cervical and abdominal ports, thus no thoracic wounds are made, and the surgical wounds are very small. Finally,the view via the right transcervical approach under pneumomediastinum is similar to that via the right transthoracic approach.
Concerning the surgical outcomes, the blood loss was slight, and the postoperative stay was short. In addition, dissection of the mediastinal lymph nodes using our MELD procedure was not inferior to that with thoracoscopic esophagectomy[22]. These results and the known benefits thus indicate that this procedure is promising and expected to become prevalent in the near future.
However, this procedure is considered to have some disadvantages as well. This procedure requires a long operation time, and recurrent nerve palsy is more frequently observed than with thoracoscopic esophagectomy[10]. In our institute, recurrent nerve palsy was recognized in about 40% of cases treated with this procedure. However, most cases recovered within six months. We speculate that recurrent nerve palsy occurred for reasons such as extension of the recurrent nerve and crush injury of the recurrent nerve. Evaluating the recurrent nerves and improving the surgical procedure using NIM nerve monitoring systems is expected to help prevent recurrent nerve palsy[23].
We consider dissection of the mediastinal lymph nodes using our MELD procedure to be sufficient.However, whether the mediastinal lymph nodes are truly sufficiently dissected using this approach should be confirmed in the next stage.
CONCLUSION
We conclude that a bilateral cervico-pneumomediastinal approach is useful for performing bilateral upper mediastinal lymph node dissection and esophagectomy.
DECLARATIONS
Authors’ contributions
Conception and design of the study: Tokairin Y, Nagai K
Informed consent of the patients was obtained by Tokairin Y, Nakajima Y, Kawad K, Hoshin A, Okada T,Matsui T, Yamaguchi K
Draたing of manuscript: Tokairin Y
Revision and final manuscript: Tokairin Y, Nagai K
General supervision: Kinugasa Y
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Written informed consent for publication was obtained as appropriate.
Copyright
© The Author(s) 2020.
杂志排行
Mini-invasive Surgery的其它文章
- Cause of recurrent laryngeal nerve paralysis following esophageal cancer surgery and preventive surgical technique along the left recurrent laryngeal nerve
- Current management of gastroesophageal reflux disease in the obese population - a review of the literature
- MlS Al - artificial intelligence application in minimally invasive surgery
- From TATA to single port robotic (SPr) taTME:approaches to distal rectal cancer
- Endoscopic-assisted lCG (EASl) technique for sentinel lymph node biopsy in breast cancer
- Uniportal video assisted thoracoscopic left upper bronchial sleeve lobectomy in a pediatric patient