A case of recurrent PMT caused by poor atrial pacing
2020-07-31JianChen
Jian Chen
Shanghai Jiaotong University Medical College Affiliated Xinhua Hospital Chongming Branch
Keywords:Poor atrial pacing Ventricular retrograde conduction Pacemaker mediated tachycardia
ABSTRACT Pacemaker mediated tachycardia (PMT) can occur in patients with DDD pacemaker implantation, and PMT in narrow sense is a kind of circular motor tachycardia, which is often caused by ventricular atrial retrograde conduction. This paper reports a case of patients with high atrial pacing value in the early stage of pacemaker implantation, resulting in atrial retrograde conduction and recurrent PMT, Almost non-stop. Although the pacemaker has the PMT automatic termination procedure, PMT is still a short array of repeated attacks due to the presence of poor atrial pacing, resulting in the patients with shortness of breath, lower extremity edema and other heart failure symptoms. Finally, PMT was stopped by prolonging PVARP, and its lower starting frequency was slowed down to 50bpm, and AV interval was kept unchanged for 250ms, so as to reduce the release of atrial pulse and encourage the emergence of self selling down-propagation excitation. The proportion of atrial and ventricular pacing was significantly reduced, which not only saved the electric energy of pacemaker, but also conformed to the physiology. In a narrow sense, pacemaker mediated tachycardia (PMT) is a kind of circular motor tachycardia, which is often caused by reverse ventricular conduction. Repeated attacks for a long time may affect the patient's heart function. Although most modern pacemakers have PMT automatic termination procedures, they are still relatively passive in the presence of some induced factors. Finally, it is necessary to extend PVARP to truly terminate and prevent PM. A case of recurrent PMT due to poor atrial pacing is reported.
1. Medical history
The patient, 74 years old male, was admitted to the hospital for one week because of repeated palpitation and shortness of breath. Physical examination: clear mind, slightly soft spirit, no dry and wet rales in auscultation of both lungs. Cardiac auscultation: the heart rate is about 120 times, the rhythm is irregular, the mitral valve area can hear and II systolic blowing noise, no pericardial friction sound. Blood pressure: 110 / 75mmgh. Slight edema of both lower limbs. 20 days ago, the patient was implanted with a dual chamber pacemaker of baiduoli company because of "sinus bradycardia, sinus arrest and syncope once". Initial setting: pacing mode DDD; upper limit frequency: 130bpm; lower limit frequency: 60bpm; PAV (AV interval of pacing): 250ms; PVARP (post ventricular atrial refractory period): 165ms; PMT protection: on; VA: 350ms. 24-hour Holter showed that intermittent atrial pacing was poor (but rarely normal atrial pacing), atrial perception function, ventricular pacing and perception function were normal. When the atrium can be captured normally by the atrial pulse, it can transmit down the atrium with P-V interval of 230ms in ap-vs mode. (Fig. 1) pacemaker mediated tachycardia may occur repeatedly due to poor atrial pacing (Fig. 2, Fig. 3). So far, the cause of adverse symptoms is basically clear, which is caused by the repeated occurrence of pacemaker mediated tachycardia.
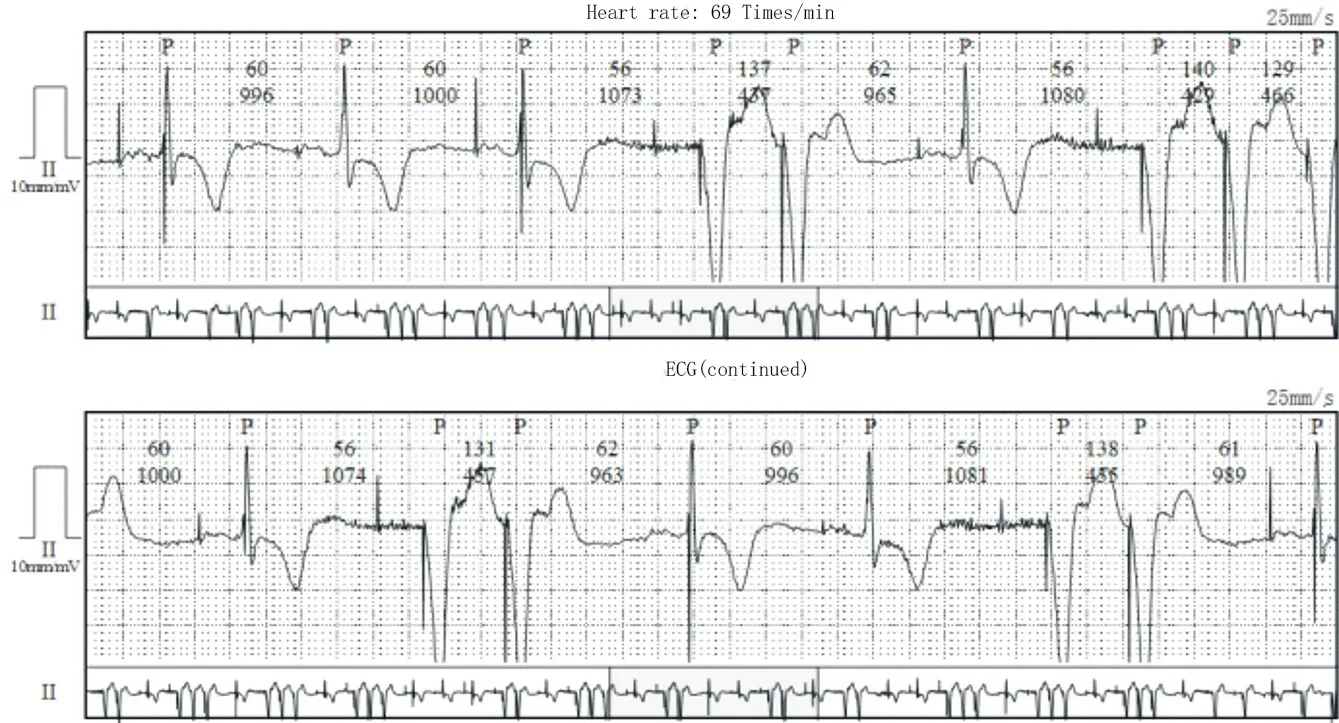
Fig. 1 (continuous recording of DCG segment shows intermittent atrial capture, but at the time of atrial capture, reentrant heart beat and short PMT caused by ventricular atrial retrograde transmission can be seen)
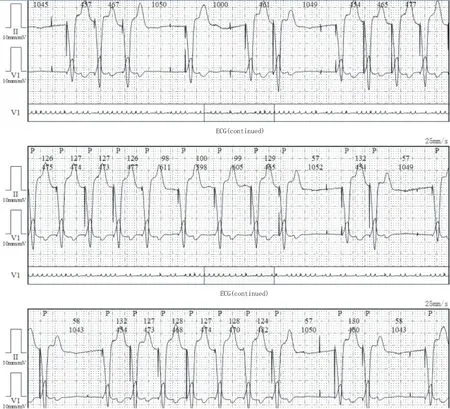
Figure 2 (continuous recording of DCG segments shows repeated PMT episodes due to repeated atrial capture)
2. Discussion
Pacemaker mediated tachycardia (PMT) can occur in patients with DDD pacemaker implantation, while PMT in narrow sense is a kind of annular motor tachycardia (ELT), which is often caused by the reverse ventricular and atrial transmission. The retrograde P wave can be sensed by the atrial circuit, and then trigger ventricular pacing. At the same time, the reverse P wave can trigger ventricular pacing again, which leads to tachycardia again and again. [1] Its frequency depends on the time of the AV reversal and the programmed sav interval, but generally it does not exceed the upper limit frequency [2] about 60% of patients with sick sinus syndrome (SSS) and 40% of patients with atrioventricular block (AVB) have the AV reversal, so about 50% of patients implanted with DDD pacemaker may produce PMT [3]. It is easy to induce the occurrence of PMT in all cases, including: atrial pacing is poor, atrial perception is poor or excessive, ventricular premature beat is accompanied by ventricular atrial retransmission, atrial premature is accompanied by long PR interval, AV interval setting is too long, AV search and so on [3]. In this case, atrial depolarization did not occur due to poor atrial pacing. Therefore, the reverse atrium conduction after ventricular pacing has the opportunity to make the atrium depolarize again and produce retrograde P wave. At the same time, due to the close relationship between the time of retrograde P and the PVARP, when the retrograde P continues to be located behind the PVARP, the tachycardia will continue to have more beats (more than a dozen beats); when the retrograde P wave is located within the PVARP, or because the amplitude of the retrograde P wave in the cavity is small and cannot be perceived by the atrial circuit [4], the tachycardia will not form or last for a short time (only a few beats), So the number of sustained beats in tachycardia will be different. At the same time, it was found that the tachycardia with more beats would be accompanied by several prolongations of A-V interval before the end of tachycardia. This is the feature of the pacemaker PMT automatic termination program of baiduoli company [5]. The frequency of 8 tachycardia heart beats detected reached the PMT detection frequency, and 8 times of vp-as interval was less than the set VA interval, and the average difference of 8 vp-as interval was less than the standard range of PMT stability. The pacemaker would observe whether the subsequent VA interval was fixed by prolonging the AV interval several times. If it was fixed, the diagnosis was established, and then PVARP was extended once, so that the retrograde P wave fell into PVARP and PMT was terminated. However, although this case has the protection of PMT automatic termination program, short array pacing tachycardia still occurs repeatedly (equivalent to the short array ventricular tachycardia originated from the location of frequent ventricular pacing electrode) due to the persistence of poor atrial pacing, which will produce hemodynamic changes and lead to heart failure symptoms such as shortness of breath, lower extremity edema, etc. Because the chest radiograph shows that the atrial electrode is in a good position, it is considered that the loss of atrial capture is caused by the increase of early atrial pacing threshold [6], which can be captured after the increase of atrial output through programmed control. However, compared with the power consumption, it may shorten the service life of the pacemaker. Therefore, it was decided to extend PVARP properly. When it was extended to 290ms, PMT would not occur, although there was still room to room retransmission during ventricular pacing. The most study results showed that the increase of cumulative ventricular pacing ratio, especially when cum% VP (cumulative ventricular pacing ratio) was more than 40%, could lead to a significant increase of the main end point events (heart failure, mortality rate) [7,8]. Some studies have also shown that there are many drawbacks in atrial pacing [9]. A review of the patients' previous Holter showed that when the atrial capture was successful, the P-V interval of 230ms could be passed down to the ventricles, so the lower pacing frequency was slowed down to 50bpm, and the AV interval remained unchanged for 250ms, so as to reduce the release of atrial pulse and encourage the occurrence of sinus down-propagation. After reexamination of DCG, it was found that most of them were self transmitted sinus beats (i.e. as-vs mode) and atrial pacing ventricles were self transmitted (i.e. ap-vs mode). The proportion of atrial and ventricular pacing was significantly reduced, which not only saved the electric energy of pacemaker, but also met the physiological requirements. At this point, the patient's palpitation, shortness of breath and other symptoms were immediately improved. Although most modern pacemakers have PMT automatic termination procedures, they are still relatively passive in the presence of some induced factors. Finally, through programmed control, fixed extension of PVARP can truly terminate and prevent PMT, and fundamentally solve the problem.
杂志排行

Journal of Hainan Medical College的其它文章
- Meta analysis of Masquelet technology and Llizarov technology in the treatment of infectious bone defects
- Establishment and evaluation of Type 2 Diabetes Mellitus andits complications induced by low dose of multiple streptozotocin
- Effect of TGIF1 expression on epithelial cadherin and Twist1 protein expression in breast cancer cells
- Acupuncture for post-stroke dysphagia: An overview of systematic reviews
- Study on novel coronavirus pneumonia (COVID-19) mechanism by Huashi Baidu Formula based on network pharmacology
- Experience of Professor Shao Mingxi in treating knee osteoarthritis based on "Bin Si Xue" acupuncture