Meta analysis of Masquelet technology and Llizarov technology in the treatment of infectious bone defects
2020-07-31HaoTianHuaWenYuZhaoWenBoBaiLeiZhangXinWeiWang
Hao-Tian Hua, Wen-Yu Zhao, Wen-Bo Bai, Lei Zhang, Xin-Wei Wang✉
1. Henan University of Traditional Chinese Medicine, Zhengzhou 450046, China 2. Shaanxi University of Traditional Chinese Medicine, Xianyang 712046, China 3. Henan Provincial Orthopedic Hospital, Luoyang 471002, Henan, China
Keywords:Masquelet technique Llizarov technique Infectious bone defect Meta analysis
ABSTRACT Objective: To systematically evaluate the clinical efficacy and safety of Masquelet technology and Llizarov group technology in the treatment of infectious bone defects by meta-analysis. Methods: The computer searched China Knowledge Network (CNKI), Wanfang, VIP, Chinese Biomedical Literature Database (CBM), Pubmed, Medline, Cochrane Llibrary databases. The retrieval time was from the time of the establishment of the database to January 2020. According to the inclusion and exclusion criteria, randomized controlled trials on the treatment of infectious bone defects using Masquelet technology and Llizarov technology were collected, and the retrieved literature was independently screened, evaluated, and data extracted by two researchers, and then RevMan5.3 software was used so for meta-analysis. Results: A total of 10 RCT documents were included, with a total of 496 patients, including 242 in the Masquelet group and 254 in the Llizarov group. The results of the meta-analysis showed that: in terms of bone defect healing time, total weight bearing time, treatment cost, and complication rate, the Masquelet group was significantly different from the Llizarov group, and the Masquelet group was better than the Llizarov group (P <0.05); In terms of knee joint Lowa score and SF-36 score, Masquelet group has significant differences compared with Llizarov group, Llizarov group is better than Masquelet group (P <0.05); in excellent rate, number of operations, ankle Lowa score, infection control rate In terms of excellent rate of affected limb function, there was no significant difference between Masquelet group and Llizarov group (P> 0.05). Conclusion: Compared with Llizarov technology, Masquelet technology has obvious advantages in the treatment of infectious bone defects in terms of bone defect healing time, total weightbearing time, treatment cost, and complication rate. In terms of scoring, it has advantages over Masquelet technology, but in terms of excellent treatment rate, number of operations, and ankle lowa score. In terms of infection control rate and excellent function of affected limbs, there was no significant difference between Masquelet technology and Llizarov technology,However, due to the low quality of the included studies and the small sample size, the exact efficacy still needs to be confirmed by higher quality RCT studies.
1. Introduction
Infectious bone defects have always been one of the difficult problems that bother orthopedists in clinical practice, which are specifically manifested in the control of infection and the reconstruction of bone defects and the repair of soft tissues. Infectious bone defects are usually caused by bone infections caused by accidents [1], trauma causes fractures, local blood flow is slow after fractures, and bacteria tend to stay at the stump [2]. Due to the presence of bacterial biofilms, antibiotics are used throughout the body. It is not obvious that bone infections are usually difficult to control [3]. Although thorough debridement is recognized as the most effective method for treating bone infections, repeated debridement will exacerbate local bone defects, making treatment more difficult, and improper treatment will make Patients are at risk for amputation [4]. Masquelet technology and Llizarov bone transfer technology are the two most commonly used methods for the treatment of infectious bone defects [5]. Masquelet technology is to fill the defect with antibiotic bone cement after thorough debridement, and use external or internal fixation to stabilize the fracture. Then, the iliac bone graft was performed after 6 ~ 8 weeks, and finally the soft tissue covered the wound surface [6]; Llizarov's bone transfer technology uses the principle of tensile stress to promote severance of blood supply and osteogenesis. The surrounding skin, muscles, blood vessels, Nerves are extended accordingly to restore bone defects [7]. Both techniques are effective for infectious bone defects, but the clinical results are different. At present, there is no meta-analysis on Masquelet technology and Llizarov technology for the treatment of infectious bone defects. Therefore, this article collected the published literature on the use of Masquelet technology and Llizarov bone removal technology to treat infectious bone defects for meta-analysis. The clinical efficacy and safety of the two methods were compared to provide clinical references.
2. Materials and methods
2.1 Inclusion and exclusion criteria
2.1.1 Research Type
Randomized controlled trials of Masquelet technology and Llizarov technology for the treatment of infectious bone defects published at home and abroad, the language is limited to Chinese and English.
2.1.2 Research objects
It meets the diagnostic criteria for infectious bone defects, and there are no special restrictions on age, gender, and so on. Randomized controlled trials comparing Masquelet technology with Llizarov technology in the treatment of infectious bone defects.
2.1.3 Interventions
One group was treated with Masquelet technology, the other was treated with Llizarov technology, and no other treatment was used in both groups.
2.1.4 Outcome indicators
Excellent rate, number of operations, treatment costs, healing time, complete weight bearing time, complication rate, infection control rate, excellent rate of affected limb function, SF-36 score, knee lowa score, ankle lowa score.
2.1.5 Exclusion criteria
①Non-randomized controlled trials; ②Reviews, case reports, experience introductions, and animal research literature; ③Interventions do not meet the inclusion criteria.
2.2 Retrieval strategy
Databases retrieved by the computer include China Knowledge Network (CNKI), VIP, Wanfang, China Biomedical Literature Database (CBM), PubMed, Medline, Cochrane Library and other databases. The search time is from the establishment of the database to January 2020. The search is performed in the form of subject words plus free words. Bone defect, etc., and then manually retrieve the references of the included literature to improve the recall rate of the literature.
2.3 Screening and extraction of included data
Use NoteExpress document management software on the computer to check the retrieved documents, and then the two researchers independently screened and retrieved the checked documents, browsed the titles and abstracts, and excluded the documents that did not meet the inclusion criteria. Then read the full text of the rest of the literature, and then screen again according to the inclusion and exclusion criteria to determine the final literature included. If the opinions of the two researchers are not consistent, internal discussions or a third party in the team should be read to discuss the decision. Perform quality evaluation and data extraction on the included literature.
2.4 Data extraction and quality evaluation
The quality of the included studies was evaluated using the Jadad score method[8]. The evaluation contents include: ①the generation of random sequences; ②the randomization and hiding;③whether the blind method is used; ④withdrawal or loss of follow-up.
2.5 Statistical methods
Meta analysis was performed using RevMan5.3 statistical software provided by Cochrane. Continuous variables were expressed as mean difference (MD); binary data were expressed as relative risk (RR) with 95% confidence interval. Calculate the I2 value to judge the heterogeneity between different studies. When I2 is greater than 50%, it indicates that the heterogeneity between studies is low. A fixed effect model should be used. When I2 is greater than 50%, it indicates the heterogeneity between studies. Higher, a random effect model should be used, P <0.05 indicates that the difference is statistically significant.
3. Results
3.1 Inclusion of basic information in the literature
According to the above search strategy and inclusion exclusion criteria, a total of 522 related documents were retrieved. The literature management software checked the remaining 339 articles. After reading the title and abstract of the article, 149 articles were initially obtained. After reading the full text of the remaining articles according to the inclusion and exclusion criteria, Finally, 10 articles were selected [9-18]. The process of document selection is shown in Figure 1. The basic information of the included documents is shown in Table 1.
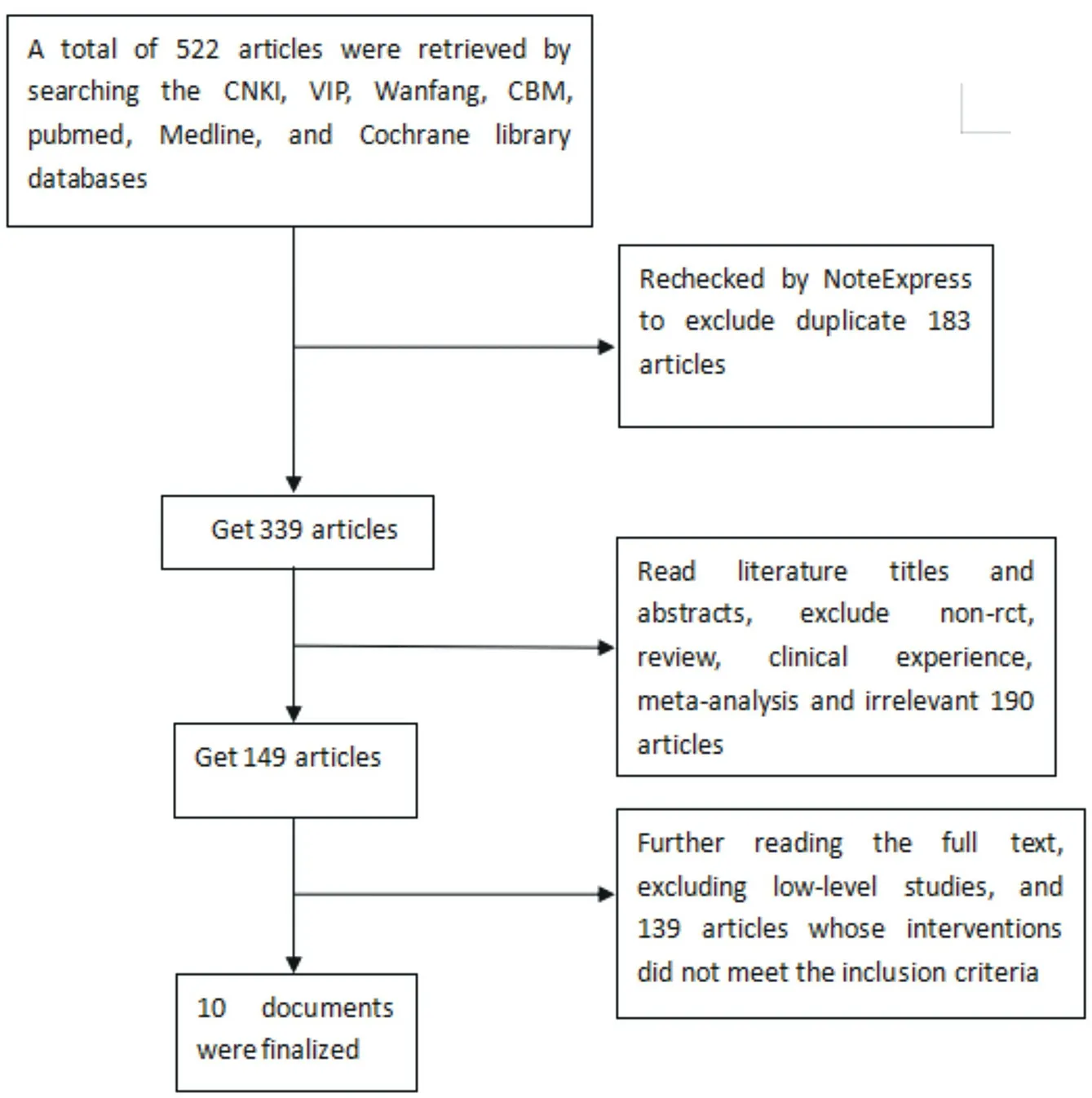
Figure 1 Document screening process
3.2 Literature quality evaluation results
A total of 10 articles were included in the study. The results of scoring the articles according to the Jadad score table are shown in Table 1. The scores of the included articles were 2 points, and the overall quality was not high. The application of the allocation concealment and blindness methods has comparable baselines between groups, as shown in Figure 2.
3.3 Meta Analysis Results
3.3.1 Cost of treatment
There are 3 literatures related to the cost of treatment [9, 10, 16]. Heterogeneity test found no heterogeneity (P = 0.92, I2= 0), using fixed effect model analysis, Meta The analysis showed that the treatment cost of the Masquelet group was lower than that of the Llizarov group, and the difference was statistically significant (MD = -1.33, 95% CI: -2.00 ~ -0.66, P <0.05), as shown in Figure 3.

Figure 3 Meta analysis of treatment costs in the two groups
3.3.2 Healing time
There are 9 articles related to healing time [9, 10, 12-18]. Heterogeneity was found after heterogeneity test (P <0.01, I2=97%). Random effect model analysis was used. Meta analysis results showed that the healing time of Masquelet group was better than that of Llizarov group, the difference was statistically significant (MD = -5.15, 95% CI: -7.53 ~ -2.78, P <0.05), as shown in Figure 4.

Table 1 Basic characteristics of the included literature
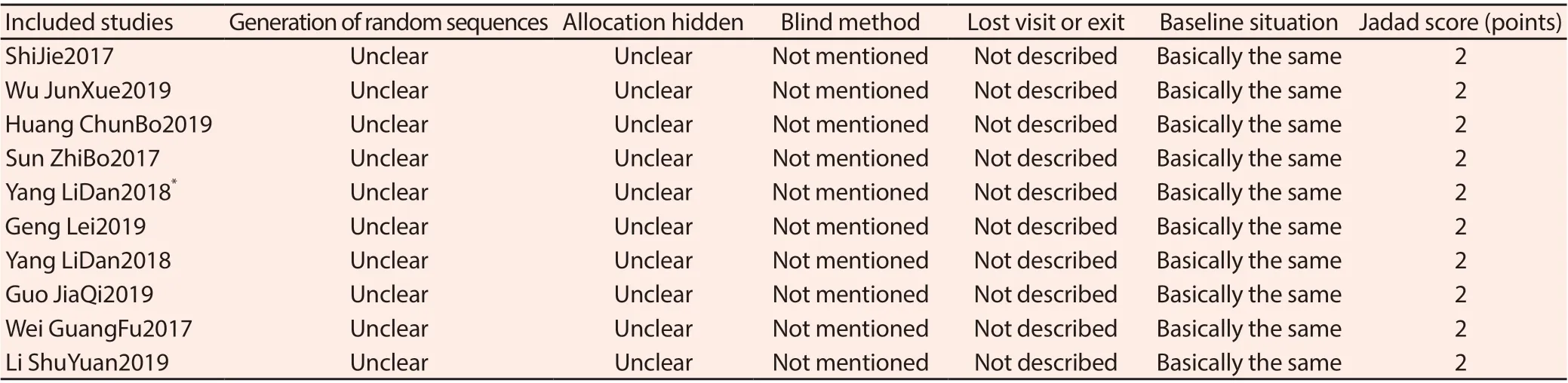
Figure 2 Included literature quality evaluation form
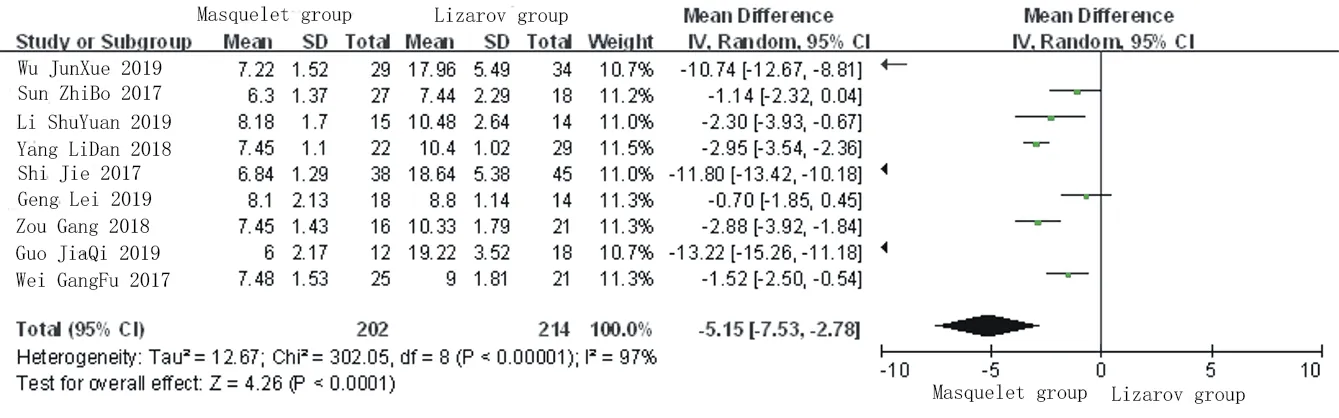
Figure 4 Meta analysis of healing time between the two groups
3.3.3 Time to complete weight bearing
There are 4 literatures concerning time to complete weight bearing [12, 13, 15, 18]. Heterogeneity test found heterogeneity (P = 0.02, I2= 68%). Random effects were used. Model analysis and Meta analysis results showed that the complete weight-bearing time of the Masquelet group was better than that of the Llizarov group, and the difference was statistically significant (MD = -10.50, 95% CI: -13.60 ~ -7.40, P <0.05), as shown in Figure 5.
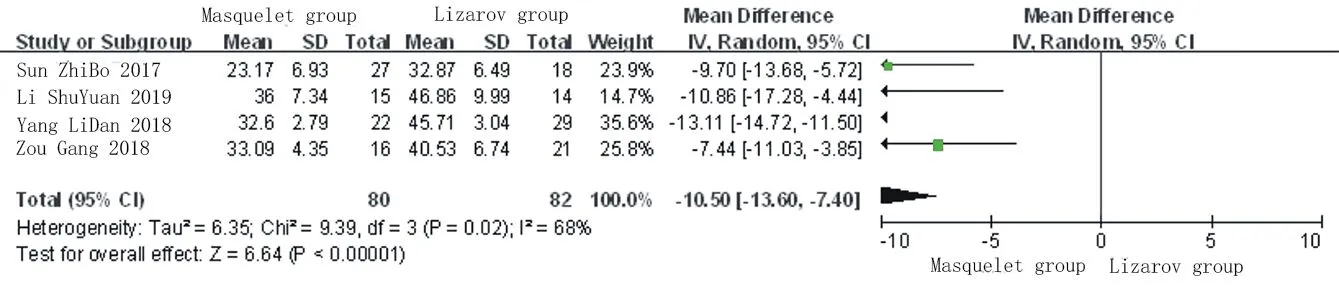
Figure 5 Meta analysis of complete weight-bearing time in two groups
3.3.4 Knee Lowa Score
There are 4 literatures related to Knee Lowa Score[12,13,15,18],Het erogeneity found after heterogeneity test (P = 0.05,I2=63%),Using random effects model analysis, the results of Meta analysis showed that the Lowa score of the knee joint in the Llizarov group was better than that in the Masquelet group, and the difference was statistically significant (MD = 3.30, 95% CI: 1.33 ~ 5.27,P<0.05),As shown in Figure 6.
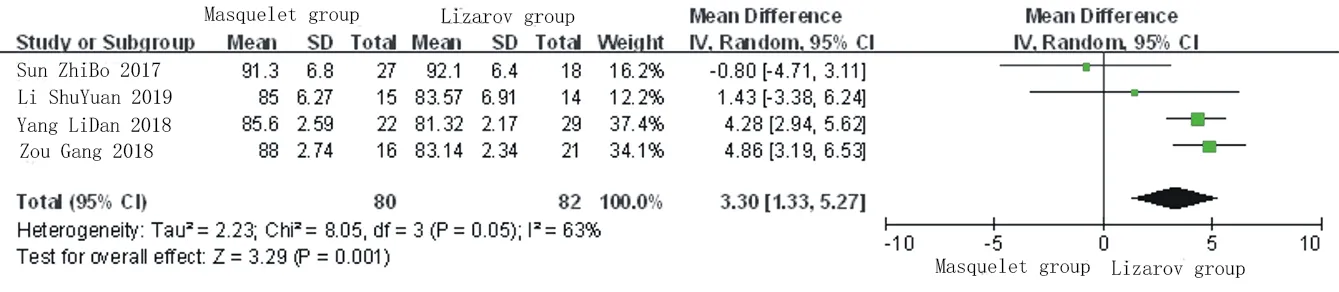
Figure 6 Meta analysis of Lowa score of two knee joints
3.3.5 Complication rate
There are 10 articles related to the complication rate [9-18]. Heterogeneity test found no heterogeneity (P = 0.09, I2= 42%). A fixed effect model was used. Analysis and meta-analysis showed that the complication rate in Masquelet group was better than that in Llizarov group, and the difference was statistically significant (RR = 0.58, 95% CI: 0.47 ~ 0.72, P <0.05), as shown in Figure 7.

Figure 7 Meta analysis of the complication rate between the two groups
3.3.6 SF-36 scoring
There are 4 literatures related to SF-36 scoring [10, 12, 13, 15]. Heterogeneity test found heterogeneity (P = 0.02, I2= 71%). Random effect model analysis and Meta analysis results showed that the SF-36 score in the Llizarov group was better than the Masquelet group, and the difference was statistically significant (MD = 8.84, 95% CI: 6.50-11.19, P <0.05), as shown in Figure 8.
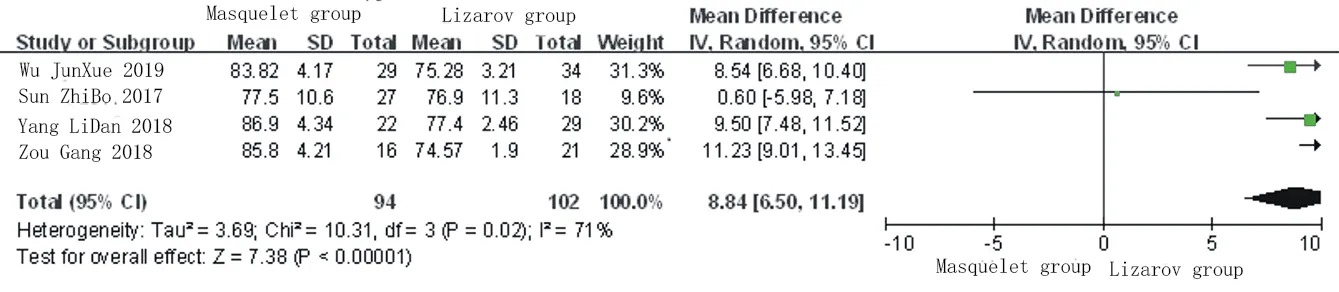
Figure 8 Meta analysis of SF-36 scores in two groups
3.3.7 Excellent rate
There are 4 articles related to excellent rate [9-11, 16]. After heterogeneity test, it is found that there is no heterogeneity (P = 0.5, I2= 0). Using fixed effect model analysis, Meta The analysis results showed that there was no significant difference in the excellent and good rate between the two treatment methods (RR = 0.99, 95% CI: 0.88 ~ 1.13, P> 0.05), indicating that the excellent rate of Masquelet technology and Llizarov technology in the treatment of infectious bone defects There is no obvious difference, as shown in Figure 9.
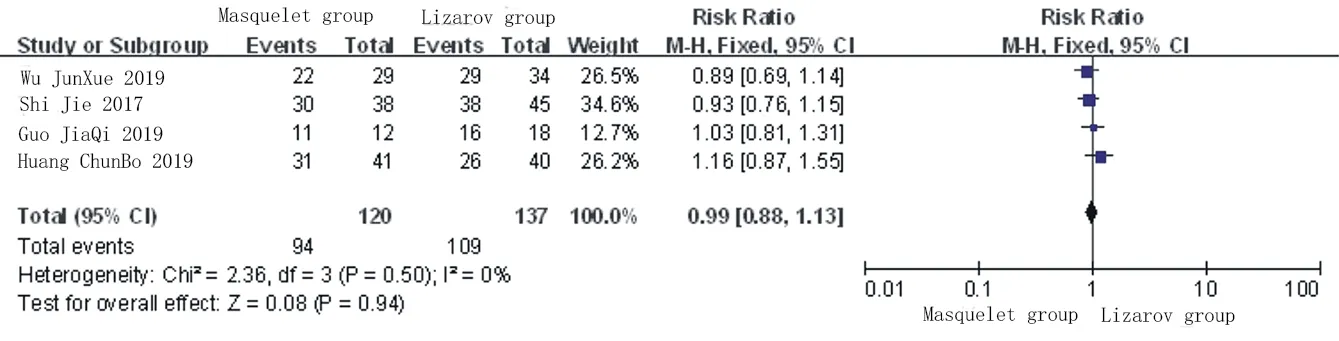
Figure 9 Meta analysis of excellent and good rate of two groups
3.3.8 Number of operations
There are 4 articles related to the number of operations[9-11,16].Heterogeneity test found heterogeneity (P = 0.10, I2= 52%). Random effect model analysis was used. Meta The analysis results show that there is no significant difference in the number of operations between the two treatment methods (MD = -0.25, 95% CI: -0.65 ~ 0.15, P> 0.05), indicating that the number of operations for Masquelet technology and Llizarov technology in the treatment of infectious bone defects There is no obvious difference in this aspect, as shown in Figure 10.
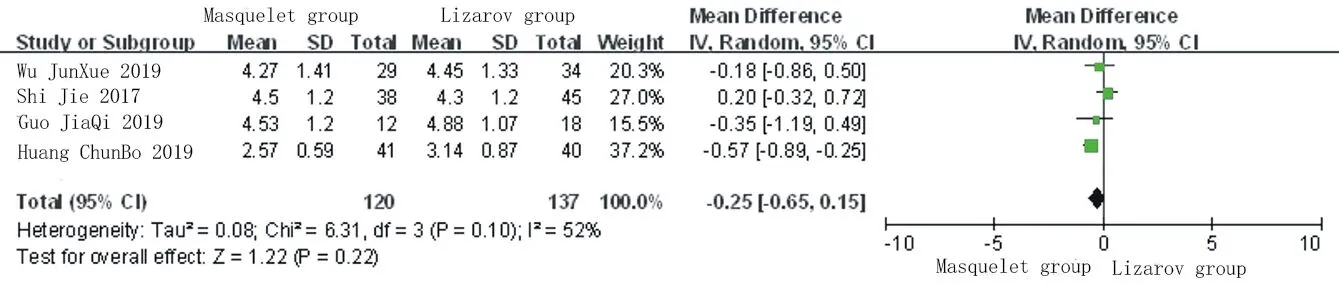
Figure 10 Meta analysis of the number of operations in the two groups
3.3.9 Ankle Lowa Score
There are 3 literatures related to the Ankle Lowa Score [12, 13, 18]. Heterogeneity test found no heterogeneity (P = 0.55, I2= 0), using fixed effects Model analysis and Meta analysis results show that there is no significant difference in the Lowa score of the ankle joint between the two treatments (MD = 0.27, 95% CI: -1.57 to 2.11, P> 0.05), indicating that Masquelet technology and Llizarov technology are in the treatment of infection There is no significant difference in the Lowa score of ankle joints for bone defects, as shown in Figure 11.
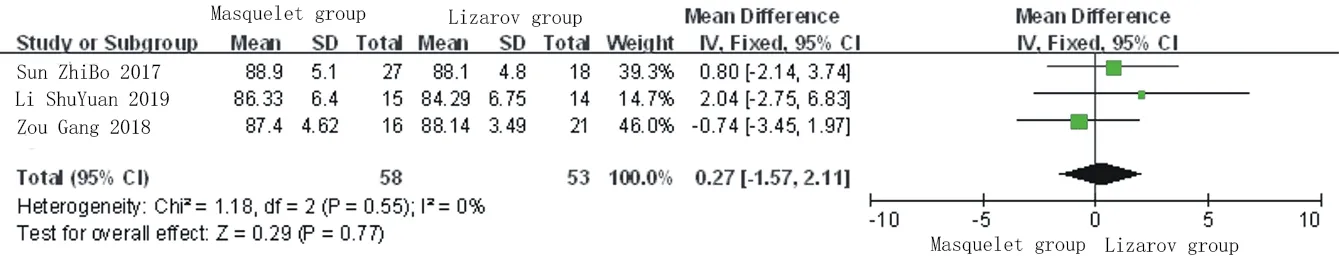
Figure 11 Meta analysis of Lowa scores of ankle joints in two groups
3.3.10 Infection control rate
There are 2 literatures on infection control rate [11, 18]. Heterogeneity test found heterogeneity (P = 0.03, I2= 78%). Random effect model analysis was used. The analysis results showed that there was no significant difference in the infection control rate between the two treatments (RR = 0.69, 95% CI: 0.15 ~ 3.10, P> 0.05), indicating that the infection control rate of Masquelet technology and Llizarov technology in treating infectious bone defects There is no obvious difference in this aspect, as shown in Figure 12.
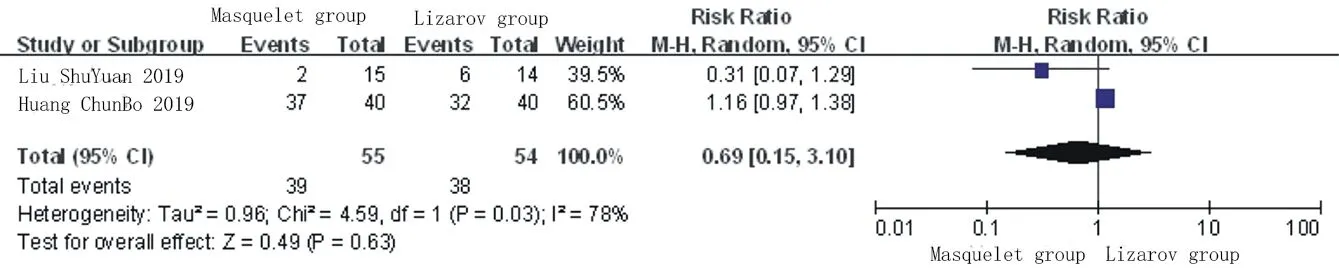
Figure 12 Meta analysis of infection control rates in two groups
3.3.11 Excellent rate of affected limb function
There are 3 literatures concerning the excellent rate of affected limb function [9, 11, 16]. Heterogeneity test found no heterogeneity (P = 0.21, I2= 35%) Using fixed-effects model analysis, the meta-analysis results showed that there was no significant difference between the two treatments in improving the excellent rate of function of the affected limb (RR = 0.99, 95% CI: 0.84 ~ 1.17, P> 0.05), indicating that Masquelet technology and Llizarov technology There is no significant difference in improving the function rate of affected limbs with infectious bone defects, as shown in Figure 13.
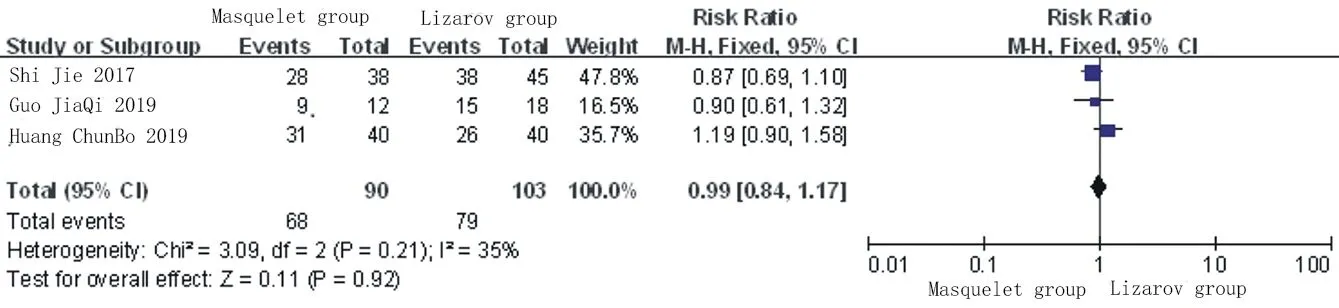
Figure 13 Meta-analysis of excellent function rate of affected limbs in two groups
3.3.12 Analysis of sensitivity and publication bias
A funnel chart was used to analyze the publication bias based on the complication rate of the included studies. It can be seen that most studies are concentrated on the top of the graph, indicating the lack of small sample studies, and the graph is approximately symmetrical, indicating that the risk of reporting bias is relatively small, as shown in Figure 14.
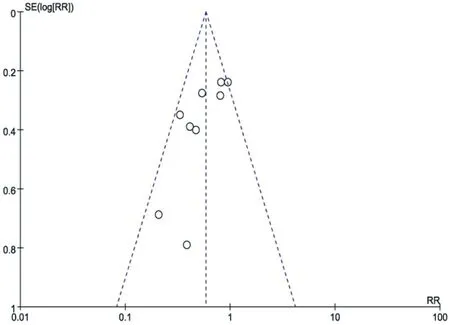
Figure 14 Funnel diagram
4. Discussion
Severe open fractures after trauma are the main causes of bone infections. The local normal blood flow is damaged and uncontrollable infections make it difficult to heal the fractures [19], which can cause infectious bone defects. In severe cases, they even face Risk of amputation. The key to the treatment of infectious bone defects is to control the infection and repair the bone defects at the same time. Masquelet technology and Llizarov bone removal technology are both commonly used in clinical treatment of infectious bone defects. In the clinic, the surgical method should be reasonably selected according to the patient's condition [20]. Llizarov bone transfer technology was first proposed in the 1950s for the treatment of bone defects, which greatly improved the treatment of bone infections. There are studies using Llizarov technology to treat infectious bone defects of the lower limbs, with a healing rate of 95% and an amputation rate. Only 2.6% [21]; Sahu used Llizarov technology to treat 60 cases of infectious osteomyelitis, and all patients achieved bone healing after surgery, with an excellent rate of 92%[22]. However, Llizarov technology also has some disadvantages: ①If the defect is large, the risk of re-fracture is high [23]; ②Moving 1mm every day, the healing time is longer; ③The external fixator brings great inconvenience to the patient's life and complications There are also more[24, 25]. The advantage of Masquelet technology is the use of antibiotic bone cement to fill femoral defects, which can continuously release antibiotics, better control infection, and provide a good environment for the defect site, induce abundant blood flow around the membrane, and have a good blood source for bone reconstruction[26]. At present, there are not many comparative studies on the clinical efficacy of Masquelet technology and Llizarov technology in the treatment of infectious bone defects, and there are some differences. There is no meta-analysis of Masquelet technology and Llizarov technology in the treatment of infectious bone defects. So this article conducted a meta-analysis.
A total of 10 literatures were included in this meta-analysis, and the methodological quality score was relatively low. The included literatures were all retrospective studies. The generation of random sequences, allocation hiding, and blind methods were not clear. Because the purpose of this study is to compare the difference between the two surgical methods, Masuquelet and Llizarov, in the treatment of infectious bone defects, the patient must be informed before treatment, which will result in low quality literature. Some of the studies have a small sample It also leads to publication bias, which affects the reliability of analysis conclusions.
This study evaluated the clinical efficacy and safety of Masquelet technology and Llizarov technology in the treatment of infectious bone defects by meta-analysis. The results show that Masquelet technology is superior to Llizarov technology in terms of treatment cost, healing time, total weight-bearing time, and incidence of complications; Llizarov technology is superior to Masquelet technology in terms of knee Lowa score and SF-36 score; in the excellent rate, the number of operations In terms of ankle joint Lowa score, infection control rate, and excellent function of affected limb, there was no significant difference between Masquelet technique and Llizarov technique. However, the quality of the literature included in this study is low and the number of cases is not large. Therefore, large-scale, high-quality RCT studies need to be further clinically conducted to further verify the results.
杂志排行

Journal of Hainan Medical College的其它文章
- Experience of Professor Shao Mingxi in treating knee osteoarthritis based on "Bin Si Xue" acupuncture
- Establishment and evaluation of Type 2 Diabetes Mellitus andits complications induced by low dose of multiple streptozotocin
- Effect of TGIF1 expression on epithelial cadherin and Twist1 protein expression in breast cancer cells
- Acupuncture for post-stroke dysphagia: An overview of systematic reviews
- Study on novel coronavirus pneumonia (COVID-19) mechanism by Huashi Baidu Formula based on network pharmacology
- A case of recurrent PMT caused by poor atrial pacing