Analysis of clinical application patterns in acupuncture-moxibustion treatment of Alzheimer disease
2020-06-22DongXiaoqing董小庆LiXiying李茜莹KongXiehe孔谐和WuLijie吴丽洁HuangQinfeng黄琴峰YangYanting杨延婷YangLing杨玲YangGuang杨光MaXiaopeng马晓芃ShiJianrong施建蓉
Dong Xiao-qing (董小庆),Li Xi-ying (李茜莹),Kong Xie-he (孔谐和),Wu Li-jie (吴丽洁),Huang Qin-feng (黄琴峰),Yang Yan-ting (杨延婷), Yang Ling (杨玲), Yang Guang (杨光),Ma Xiao-peng (马晓芃),,ShiJian-rong (施建蓉)
1ShanghaiUniversity of Traditional Chinese Medicine,Shanghai201203,China
2ShanghaiResearch Institute of Acupunctureand Meridian,Shanghai 200030,China
3ShanghaiJiaoTong University School of Medicine,Shanghai 200025,China
Abstract
Keywords:AcupunctureTherapy;MoxibustionTherapy;Acupuncture-moxibustionTherapy;Alzheimer Disease;Dementia; Bibliometrics; Databases (TraditionalChinese Medicine)
Alzheimer disease (AD)is achronic degenerative neurological disease, featured by progressive memory loss and cognitive impairment[1]. It affects the medial temporal lobe and cortical structures[2], and manifests as memory impairment, aphasia, agnosia, visuospatial impairment,executive dysfunctionandchangesin behaviors and personality[3]. An epidemiological study founditsincidence doubledevery 5yearsamongst people aged over 65 and above 35% of people aged over 80 were affected by this disease[4]. By 2025, the number of people affected by AD is predicted to exceed 0.115billion[5].Thecauseof ADisunclear yet,but multiple factors such as genetic factor, environmental factor, neurotransmitters, and immunological factor are possibly involved[6].Itspathogenesis israther complicated,involving extracellular β-amyloidprotein(Aβ) deposition, abnormal intracellular accumulation of tauprotein,cholinergicsystemdisorder,synaptic damage,interneuronabnormality andbrainnetwork abnormality[7]. During the recent 10 years, acupuncture- moxibustion therapy has achieved significant efficacy in treatmentof AD[8].Itsmulti-target multi-channel comprehensive regulation effect has unique advantage compared with the symptomatic treatment of Western medicine[9]. Based on the previous research, this article summarizedtheclinicalapplicationrules of acupuncture-moxibustion treatment of AD by analyzing the eligible clinical studies published during the past 10 years, to provide references for clinical practice.
1 Materials and Methods
1.1 Retrieval strategy
Thefollowing databasesweresearched:China NationalKnowledge Infrastructure(CNKI),Wanfang Academic JournalFull-textDatabase(Wanfang),ChongqingVIP Database(CQVIP),ChineseMedicine Acupuncture-moxibustionInformationDatabase,PubMedMedicalDataRetrievalServiceSystem,Springer Database and Ovid Technologies (OVID). Same search terms were used in both Chinese and English,including ‘senile dementia’, ‘Alzheimer disease’, ‘elderly dementia’,‘acupuncture-moxibustion’,‘acupuncture’,‘acupunctureandmedication’,‘electroacupuncture’,‘moxibustion’, ‘point’, ‘acupoint’ ‘application’, ‘compress’,‘ear’,‘thread-embedding’,‘cupping’,‘bloodpricking’,‘hydro-acupuncture’ and ‘point injection’, and the target study type was clinical trial only. The Boolean retrieval strategies wereestablishedusing subjects, titlesand keywords, with AND, OR and NOT as the conjunctions.
1.2 Inclusion criteria
Clinical studies of acupuncture-moxibustion treating AD;Chineseor Englisharticlespublishedin journals betweenJanuary 2009andDecember 2019;acupuncture-moxibustionwastakenas themajor treatment whileother Westernor Chinesemedicine treatmentscouldbe involvedonly asthe adjuvant;samplesize ≥5casesandtherapeutic efficacy was confirmed, with detailed point selection, treatment and observationmethods;if therewas another acupuncture-moxibustion method or a different group of pointselectedin thecontrol, thestudy couldbe separated into two or more studies accordingly.
1.3 Exclusion criteria
Repetitivepublications(theinitialpublicationwas kept); same content but published both in Chinese and English languages (the Chinese version was kept); had errors in data.
1.4 Data processing
Quantitative analysis was conducted for major points andtreatmentmethodswithhighfrequencies.The SPSS version24.0 softwarewas usedfor clustering analysis;Clementine12.0was adoptedtoperform associationanalysisusing Apriorialgorithm.Measurementdatainnormaldistributionwere expressedasmean±standarddeviation(±s)and examinedusingt-test inintra-groupcomparisons.Thosenot innormaldistributionwere expressedas median (inter quartile range) [M (IQR)] and examined by non-parametric test. The inter-group comparisons of rate were analyzed using Chi-square test. The statistical standard was set atα=0.05 andP<0.05 was considered statistically significant.
2 Results
2.1 Generalresult indataretrievalof acupuncture- moxibustion treatment of AD
A total of 166 clinical studies were retrieved, of which,145were eligibleaccording totheinclusionand exclusion criteria, including 130 in Chinese language and 15inEnglish, involving 159 acupuncture-moxibustion prescriptions, 110 points, 10 treatment methods and 8 outcome measures.
2.2 Analysisof pointselectioninclinicalstudies of acupuncture-moxibustion treatment of AD
2.2.1 Point frequency analysis
Of the 110 points from the 145 clinical studies, 96 were from the fourteen meridians, 5 were extra points and 9 were auricular points.Baihui (GV 20)had the highest frequency andhadbeenused for 88 times,accounting for 55.3% (Frequency rate = Frequency ÷ Totalnumber of prescription×100%);followedby Zusanli(ST 36),Sishencong (EX-HN1),Taixi(KI3),Sanyinjiao (SP6)andNeiguan(PC 6),allwitha frequency above 40. The details are shown in Table 1.

Table 1.Major pointsinacupuncture-moxibustion treatment of AD
2.2.2 Analysis of meridian and region distributions
Thefrequency rate andpercentagewereusedto interpret the results. Frequency rate = Total frequency of the involvedpointsfromthis meridian÷ Total frequency of theinvolvedpointsfromthefourteen meridians × 100%. Percentage = Total number of the involved points from this meridian ÷ Total number of the involved points from the fourteen meridians × 100%.Thefourteenmeridians wereallinvolvedinclinical studiesof acupuncture-moxibustion treatment of AD and their points had a total frequency of 926, while the total frequency of extra points was 91. In respect to the meridian distribution, points from yang meridians had higher frequencies, accounting for 61.9% of the total frequency of the fourteenmeridianpoints.Of the points from yang meridians, those from the Governor Vesselhadthe highestfrequency,whichwas226,followed by those from the Stomach Meridian and the Gallbladder Meridian, whose frequency was 117 and 98,respectively. The total frequency rate of the points from theabovethreemeridians was47.6%.Among the Bladder Meridianpoints,Back-Shupoints hadthe highest frequency;themost commonly used Pericardium Meridian point was Neiguan (PC 6) and it was Taichong (LR 3) for the Liver Meridian (Table 2).
Table3shows that thepoints selectedin acupuncture-moxibustion treatment of AD were mainly distributedin the head-faceandlower-limbregions,followedby upper-limb,back andchest-abdomen regions.Table2andTable3unveilthatthepoints located in the head-face region were mainly from the Governor Vessel and Gallbladder Meridian, those in the lower-limbregionweremainly fromtheSpleen,Stomach and Kidney Meridians, those in the upper-limb region were mainly from the Pericardium Meridian and the Heart Meridian, and those in the chest-abdomen region were mainly from the Conception Vessel and the Bladder Meridian.
2.2.3 Point association analysis
Clementine12.0was usedtoperformassociation analysis for the 10 majorly used points and 10 terms with a confidence >85.0% were listed in order from high to low confidence. Support shows the support for the former item in the rule, and here it specifically referred to the rate of the number of studies involving the points in the former item to the total number of the included studies in acupuncture-moxibustion treatment of AD.Baihui (GV 20)-Sishencong (EX-HN 1)-Zusanli (ST 36) and Baihui (GV 20)-Neiguan (PC 6)-Sanyinjiao (SP 6) had a comparatively high support. Confidence stands for the ratio of support to support intherule,here representing therateof thenumber of studies concurrently involving both the former and latter items to the number of studies involving the former item. For example,thepossibility of concurrent presenceof Baihui(GV 20)andSishencong (EX-HN1)-Neiguan(PC 6)-Sanyinjiao (SP 6) was 100%, and the support of this prescription was12.057%. The point association analysisshowedthatof the prescriptions in acupuncture-moxibustiontreatmentof AD,Baihui(GV 20)andSishencong (EX-HN1)-Neiguan(PC 6)-Sanyinjiao (SP 6) had the most significant association,followed by Baihui (GV 20) and Sishencong (EX-HN 1)- Neiguan (PC 6)-Zusanli (ST 36), and Zusanli (ST 36) and Sanyinjiao(SP6)-Sishencong (EX-HN1)-Taixi(KI3)- Baihui (GV 20), (Table 4).
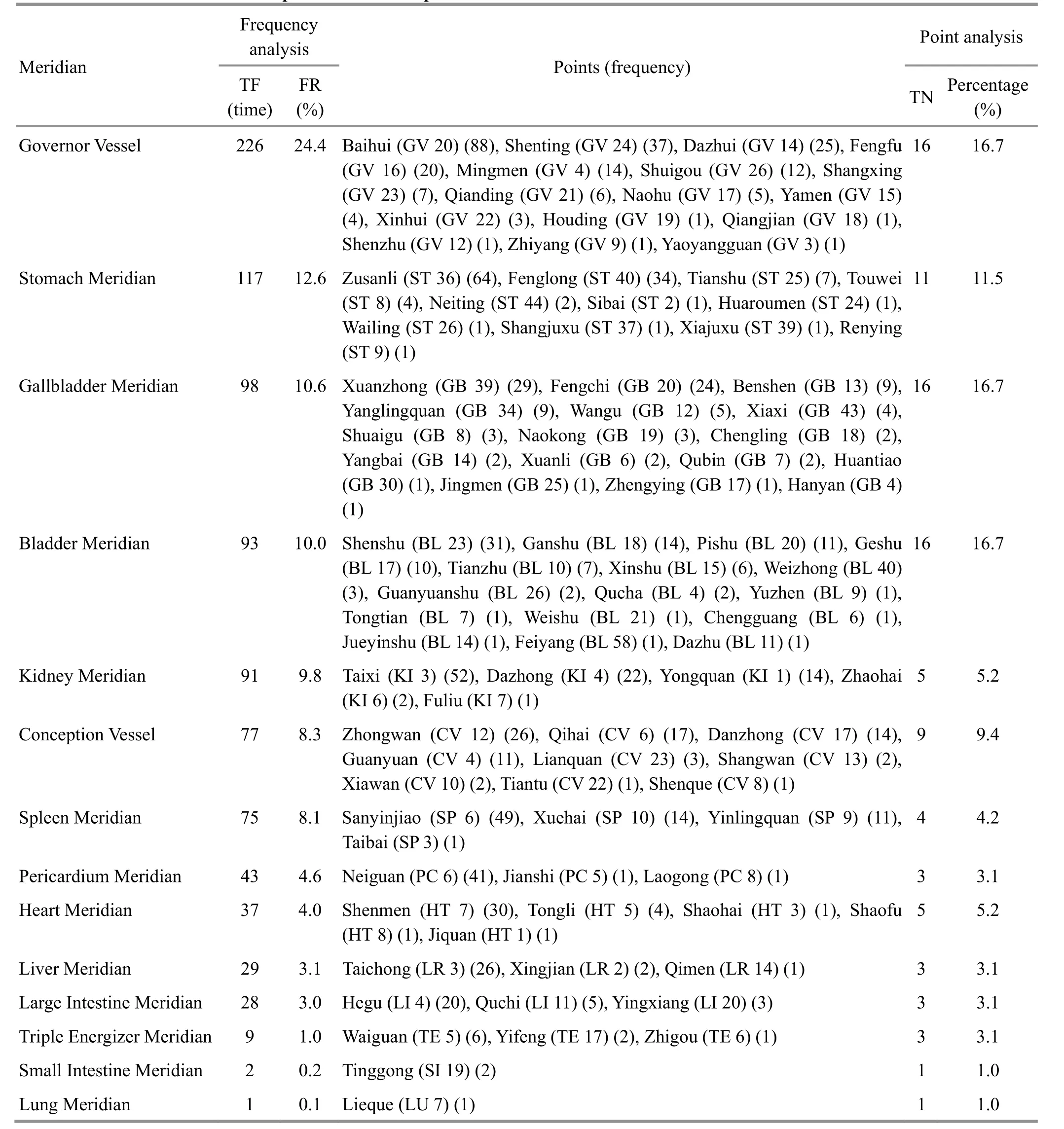
Table 2.Meridian distributionof pointsused inacupuncture-moxibustion treatment of AD
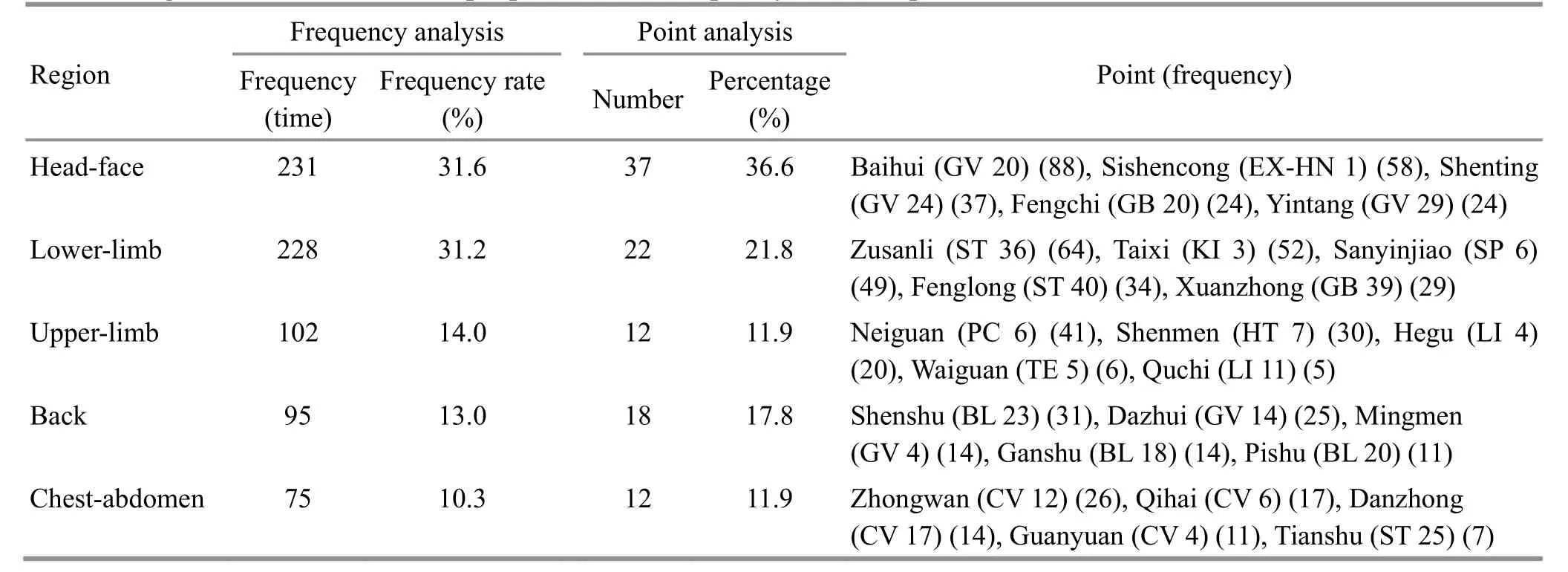
Table 3.Region distribution of thetop5points onthe frequency list inacupuncture-moxibustiontreatment of AD
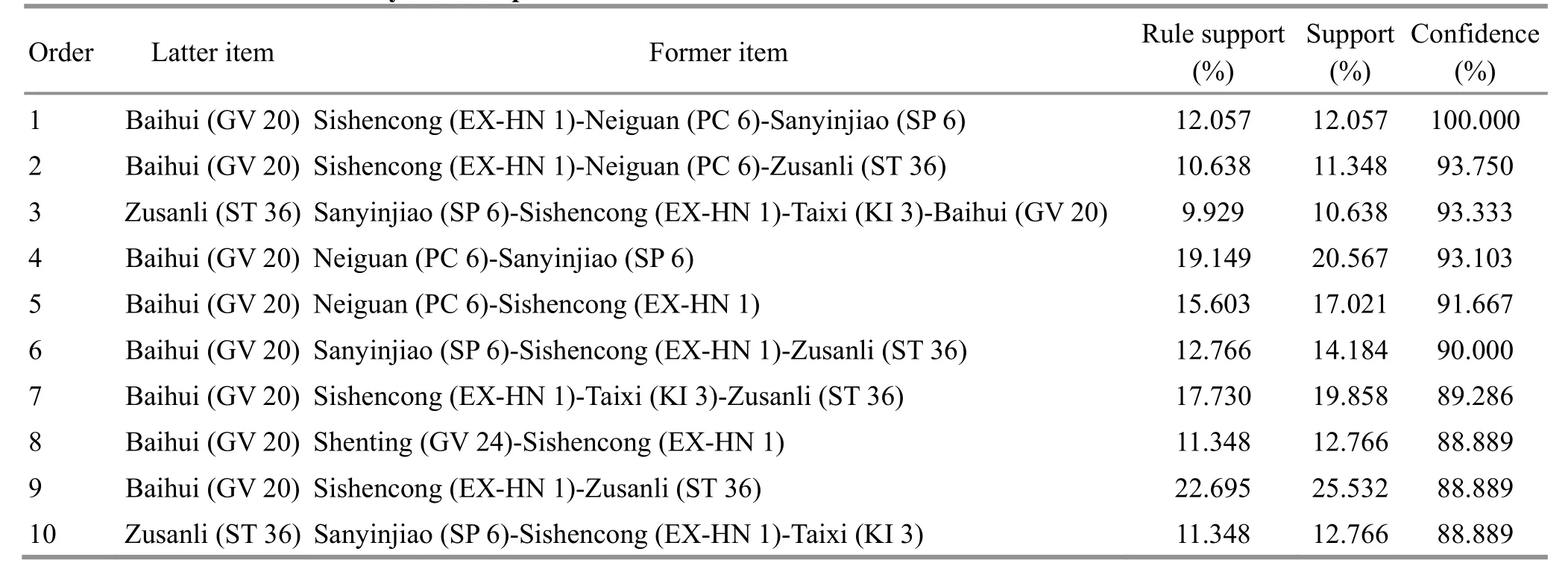
Table 4.Point associationanalysis in acupuncture-moxibustion treatment of AD
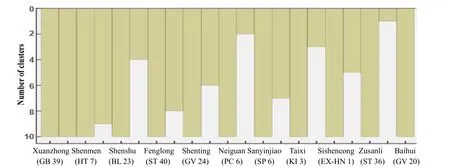
2.2.4 Clustering analysis of the major points
SPSS 24.0 was used to perform clustering analysis for the major points in acupuncture-moxibustion treatment of AD.
Figure 1 is an icicle plot revealing the point clustering results. When divided into four clusters, four effective clusters wereobtained:Baihui(GV 20),Zusanli (ST 36)-Sishencong (EX-HN1),Taixi(KI3)-Sanyinjiao(SP 6) and Neiguan (PC 6)-Shenting (GV 24)-Fenglong(ST 40)-Shenshu(BL 23)-Shenmen(HT 7)-Xuanzhong (GB 39).
Figure 2 is a dendrogram presenting point clustering results.Inline withtheicicleplot,Figure2 demonstrates that Baihui (GV 20) alone was classified into one cluster, while the rest points all belonged to another cluster,suggesting thegreat significance of Baihui(GV 20)intreating AD.According tothe clustering analysis, the commonly usedpoint groups included: Sishencong (EX-HN 1)-Zusanli (ST 36) and Taixi(KI3)-Sanyinjiao (SP6),whichdisplayedanobvious coordination relationship between each other; another group was Neiguan (PC 6)-Shenting (GV 24)-Fenglong (ST 40)-Shenshu(BL 23)-Shenmen(HT 7)-Xuanzhong (GB 39). The above groups were all closely associated with Baihui (GV 20).
2.3 Efficacy comparison amongst the commonly used acupuncture-moxibustion treatment methods for AD
Of theincludedstudies,62studiedacupuncture alone,55focusedonacupuncturecombinedwith medication,12observedmonotherapy of electroacupuncture,and9studiedelectroacupuncture combinedwithmedication.Studies thatadopted efficacy index [calculatedbasedonthescoreof mini-mental state examination (MMSE) as the outcome measurewereselected[10],basedonwhich,three treatment methods at the top of the frequency list were compared in term of efficacy. The results showed that acupuncture plus medication achieved the highest total effective rate and electroacupuncture won the second place,bothbetter thanacupuncturealone,with significant differences(bothP<0.05).Although acupuncture plus medication had a higher effective rate compared with electroacupuncture, the difference was statistically insignificant (P>0.05), (Table 5).

2.4 Analysis of thescale scores inacupuncturemoxibustion treatment of AD
Thereweremainly 8kinds of scales usedinclinical studiesof acupuncture-moxibustion treatment of AD,predominatedby theMMSE,activity of daily living scale(ADL)andAlzheimer disease assessment scale-cognitive section(ADAS-cog).Other scales,suchasMontreal cognitiveassessment (MoCA),digit symbolsubtest (DS),rapidvocabulary response(RVR),functionalactivities questionnaire(FAQ),andrevisedHasegawadementia scale(HDS-R),wereused3timesonaverage.We comparedthemeans(or medians)of thescoresof MMSE,ADL andADAS-cogbefore andafter acupuncture-moxibustiontreatment,demonstrating that thepost-treatmentdifferences inthe scoresof MMSE,ADL andADAS-cog wereallstatistically significant (allP<0.01),(Table 6).
Of theincludedclinicalstudies,33studies that observedmonotherapy of acupuncture,37on acupunctureplusmedicationand9onmonotherapy of electroacupunctureadoptedMMSEas theoutcome measureandoffereddetailedscores.Inthese studies,the MMSEscoreshowedsignificant differences after treatment despitethemethod(allP<0.01).The between-groupcomparisonsalsoshowedstatistical significance(allP<0.05),indicating thatacupuncture plus medicationhadthe most significant efficacy and electroacupuncturewas superior to acupuncture(Table7).

Table 5.Comparisonamongst the commonly used acupuncture-moxibustiontreatment methods for AD

Table 6.Outcome measure analysisin thestudies of acupuncture-moxibustion treatment of AD(point)
Table 7.Comparison among the three treatment methodsbased ontheMMSEscore ( ±s, point)

Table 7.Comparison among the three treatment methodsbased ontheMMSEscore ( ±s, point)
Note:Compared with thesamegroup beforetreatment,1) P<0.05;compared with acupuncture,2) P<0.05
Treatment method nPre-treatment Post-treatment Post-treatment difference Acupuncture3317.94±0.5621.66±0.571)3.72±0.34 Acupuncture plusmedication 3717.17±0.3722.67±0.511)5.50±0.422)Electroacupuncture916.69±0.8020.80±0.831)4.11±0.742)
3 Discussion
During the recent years,therehave occurredmore andmore reportsonacupuncture-moxibustiontreating AD.A systematic review focusing onitseffectiveness andsafety[11]showedthatacupuncture-moxibustion may bemoreeffective than medicationandcanhelp medicationinimproving thecognitivefunctionin additiontoits highsafety assessment. Therefore,it is of great significance to summarizetherulesof using acupuncture-moxibustionintreatment of AD,to provide referencesfor clinicalpractice andpromoteits application.
Thepoint selectioninacupuncture-moxibustion treatment of AD showed,Baihui(GV 20)wonthetop withitsfrequency of 88andits frequency ratewas 55.3%,followedby Zusanli(ST 36),Sishencong (EX-HN1),Taixi(KI3),Sanyinjiao(SP6)andNeiguan(PC 6),whichallhadafrequency over 40.The associationandclustering analyses demonstrated:Baihui(GV 20)andSishencong (EX-HN1)-Neiguan(SP6)-Sanyinjiao(SP6)hadthemostsignificant association;the commonly usedpointpairswere Zusanli(ST 36)-Sishencong (EX-HN1),andTaixi (KI3)-Sanyinjiao(SP6);thecommonly usedpoint groupswereNeiguan (PC 6)-Shenting (GV 24)-Fenglong (ST 40)-Shenshu(BL 23)-Shenmen(HT 7)-Xuanzhong (GB 39). These commonly usedpoint groups were all closely associatedwithBaihui(GV 20).Of the involved points,Baihui(GV 20),Sishencong (EX-HN1)and Neiguan(PC 6)cancalmthemindandbenefit the intelligence,sothatthey areusedto treatmental disorders.Baihui(GV 20)is the crossingpoint of the FootTaiyangMeridian,HandandFoot Shaoyang Meridians,Foot JueyinMeridianandGovernor Vessel andit connectsthe brain. It is saidthat thefourteen meridians allgo passing the vertex and joinat Baihui(GV 20)[12].Hence,puncturing Baihui(GV 20)can nourishtheseaof marrow,awakenthebrainandopen orifices.Taixi(KI3)andSanyinjiao (SP6)functionto tonify thespleenandkidney.TraditionalChinese medicine(TCM)holds that ADmainly affects thebrain andkidney deficiency istheroot.Brainisgeneratedby theprenatalkidney essence whileitsnormalfunctionis based onthe nourishment of thepostnatalessence.Whenspleen-stomachqiat themiddleenergizer failsto ascendanddescendnormally,qiand bloodwon’t be ableto reachtheheartandhead,sothat turbid phlegm andstasis willblock the orificesandcognitive dysfunctionssuch asforgetfulnessanddementiaare likely tohappen[13].Essenceand bloodsharethesame origin.If kidney essence is insufficient,qiandbloodwill be inshortage.Insufficient kidney essenceandalack of postnatalqiandbloodmay causeshortnessof nourishment providedtothe seaof marrow,leading to bloodstasisblocking collaterals andthedevelopment of AD[14].Therefore,Taixi (KI 3),Sanyinjiao (SP 6),Zusanli(ST 36)andShenshu(BL 23)areselectedtosupplement the essence andblood,dispelstasisandunblock collaterals.Sincebrainisconsideredtheseaof marrow andXuanzhong (GB 39)isdefinedasthejointof marrow, it is of great significancetoselect these points to treat AD. A modern study told that acupuncture at Baihui (GV 20) and Sishencong (EX-HN 1) can notably improve the learning and memory abilities and enhance the activation of superoxide dismutase (SOD) based on an AD rat model[15]. According to the point selection analysis, the involved points which are located in the head-face region are mainly from the Governor Vessel andGallbladder Meridian,andthoselocatedinthe lower-limb region are mainly from the Spleen, Stomach and Kidney Meridians, which are in accordance with the frequency list.Theinvolvedpointslocatedinthe upper-limbregionarepredominately fromthe Pericardium and Heart Meridians and those located in the chest-back region are mostly from the Conception Vessel and Bladder Meridian. TCM theory says that the heart isinchargeof mind andspirit andisclosely related to mental activities[16].Chapter Xie Ke ofLing Shu(the 71st Chapter of Spiritual Pivot) states, ‘heart,the monarch of the five Zang and six Fu organs, is where the spirit resides’. Modern research has also proved the regulatory effects of heart-secretedcardionatrinand brainnatriuretic peptide(BNP)onthebrain function[17-18], which hasprovided strong evidence to testify the closerelationshipbetween thebrainand heart.
Analysis of the major outcome measures used in the includedstudies discoveredthat concurrent useof MMSE and ADL is the most common way in evaluating thecognitivefunction,thoughsomestudiesmade some mistakes in application. The MMSE scale assesses the cognitive function via 30 questions, mainly involving theabilities of attention,orientation,memory,registration,recall, calculation,language anddrawing complex polygons[19]. But, this assessment result is likely tobe affectedby theeducationlevelof patients,demonstrated by false negative in the high education group and false positive in thelow education group.Therefore, the consistency of patients’ education level is anecessary condition to ensure the accuracy of this scale. However, most clinical studies did not make clear requirements for the MMSE baseline values. AD has a progressiveclinicalprocess.Its severity andstage shouldbeassessedusing well-recognizedscalesto reducebias.Another study showedthat theMMSE scalelacksaccuracy indifferentiating mild cognitive impairment (MCI) and AD-induced dementia[20]. MoCA is more suitable than MMSE to diagnose MCI in patients agedover 60[21].It is likely to causecertainbiasin sampleselectionwhenMMSEisadoptedasthe diagnosis or inclusionandexclusioncriteriainAD studies, which may misguide clinical practice due to the falsestudy results[22].But unfortunately,thereis no other option yet.
Regarding thefrequency of treatment method,although the frequency of acupuncture alone won the first place,acupunctureplusmedicationwas the optimal one in terms of total effectiverate and the improvementof theMMSEscore,followedby electroacupuncture.Thelatter twomethodswere superior to acupuncturealoneconsideringthe therapeutic efficacy. However, possible errors may exist due to the small sample of the included studies. Studies have proved that moxibustion can reduce the edema of nerve cells to promote the repair[23]; the combination of moxibustionandelectroacupuncturecandown- regulate the expressions of Aβ1-42 and LC3-I, thereby improving thecognitivefunctionand protecting the centralnervous system of ADmice[24-25];moxibustion plus electroacupuncturewasequivalent todonepezil hydrochloride comparing the protective and treatment effects onAD[26].Meanwhile,it’salso reportedthat moxibustion at Shenque (CV 8) and Zusanli (ST 36) can enhance the expressions of adiponectin receptor gene and protein and exert protective effect on the brain of AD rats[27]. However, most studies in this field are based on animals and there lacks sufficient clinical reports on moxibustion treatment of AD. More clinical studies are expected to verify the findings.
This articleanalyzedthepoints andtreatment methods in acupuncture-moxibustion treatment of AD basedonliteratureanalysis anddatamining.The recommendedpointsincludeBaihui(GV 20),Sishencong (EX-HN 1), Neiguan (PC 6), Zusanli (ST 36),Sanyinjiao (SP 6) and Taixi (KI 3), with Shenting (GV 24),Fenglong (ST 40), Shenshu (BL 23), Shenmen (HT 7) and Xuanzhong (GB39)addedaccordingly.Treatment methodsincluding acupuncture-moxibustionplus medication and electroacupuncture are recommended.In clinical practice, the points can be adjusted based on patterndifferentiationof TCMtoachieveabetter treatment result.
Conflict of Interest The authorsdeclarethat thereisnoconflict of interest.Acknowledgments Thiswork wassupported by National Natural Science Foundation of China (国家自然科学基金项目,No.81674073);Training Project for Talent Leader of Shanghai Municipal Health Commission (上海市卫生计生系统优秀学科带头人培养计划项目, No.2017BR047.
Received:19 November 2019/Accepted:9January 2020
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Therapeutic observation of manipulation plus exercise therapy in treating upper crossed syndrome postures of primary school students
- Therapeutic observation on lung-clearing and spleen-strengthening tuina in children with exogenous cough
- Clinical observation on heat-sensitive moxibustion plus lactulose for postoperative constipation of mixed hemorrhoid due to spleen deficiency
- Therapeutic effect of heat-sensitive moxibustion plus medications for senile osteoporosis and its effect on serum BMP-2 and OPG levels
- Effects of electroacupuncture plus drug anesthesia on pain and stress response in patients after radical surgery for stomach cancer
- Therapeutic efficacy observation on auricular point sticking therapy for cardiac syndrome X in women