Therapeutic observation of manipulation plus exercise therapy in treating upper crossed syndrome postures of primary school students
2020-06-22JiangFang姜芳LuoRong罗容TangJing唐静YeYong叶勇ZhaoYanling赵艳玲
Jiang Fang (姜芳),LuoRong (罗容),Tang Jing (唐静), Ye Yong (叶勇),Zhao Yan-ling (赵艳玲)
1Hunan University of Chinese Medicine,Changsha 410208,China
2The First Affiliated Hospital of Hunan University of ChineseMedicine,Changsha 410007,China
Abstract
Keywords:Tuina; Massage; Exercise Therapy; Upper Crossed Syndrome; PosturalAssessment; Biomechanics;Students
Upper crossed syndrome (UCS) is a postural disorder featuredby forwardheadpostureandabnormal configuration of shoulder girdle, caused by loss of the biomechanicalbalanceinthehead,neckand shoulders[1]. Due to incorrect postures throughout study andlifeandthepopularity of electronic products,the incidence of UCS has beenincreasing inprimary schoolstudents.Thesurvey conductedby Beijing National Physique Monitoring Center showed that over 85% of the adolescentshad abnormalpostures, and forwardneck,roundedshouldersandhunchback accounted for 46.1%[2]. Children are the future of our country.Their physicalquality directly affects their future development and the overall image of the nation.Thestudy performedby SunBH,et al[3]has demonstratedthatyoung peoplehavehighphysical plasticity, so that their physiological curvature hopefully can be corrected and restored. This study result was of guidingsignificanceto changetheUCS postures in primary schoolstudents.Currently,exercise,physical and Chinese tuina therapies are the main methods used inthetreatment of UCS[4].Weusedsinew-bone balancing manipulation combined with exercise therapy to treat UCS in primary school students, and observed the changes in the sagittal static posture assessment totalscore,forwardheadangle(FHA)andforward shoulder angle (FSA) in order to evaluate the postures.The report is given as follows.
1 Clinical Materials
1.1 Diagnostic criteria
The diagnostic criteria were made by referring the relevant literatures[5]: pain in the neck and shoulders,scapular winging,forwardhead;slouchedback (roundedshoulders),chest tightness,occasional headache; viewed from the side, the earlobe is in front of the acromion.
1.2 Inclusion criteria
Conformedto the abovediagnostic criteria;aged 6-13years old;skeletaldiseases (suchascongenital scoliosis, deformity, bone tuberculosis and bone tumors)excluded by imaging tests; willing to participate in the trialandthe guardiansignedtheinformedconsent form.
1.3 Exclusion criteria
Was receiving other treatments; coupled with other diseases that made it improper to take this treatment protocol; cervical spondylosis; had a history of cervical or shoulder surgery.
1.4 Statistical analysis
TheSPSS version25.0 softwarewas usedfor statisticalanalysis.Measurement datainnormal distributionandhomogeneity of variancewere expressed as mean ± standard deviation (±s), and were analyzedusing pairedt-test inintra-group comparisonsandgroupt-test inbetween-group comparison.Enumerationdatawereexaminedby Chi-squaretest.Rankeddatawereprocessedusing rank-sum test.P<0.05 indicated statistical significance.
1.5 General data
This trial was conducted between September 2018 and July 2019 in the First Affiliated Hospital of Hunan University of Chinese Medicine.
A total of 60 primary school students diagnosed with UCS were recruited from the posture training class of the Acupuncture-moxibustion and Tuina Rehabilitation Department of TheFirst AffiliatedHospital of Hunan University of Chinese Medicine. They were divided into an exercise group and a combination group using the random number table method, with 30 cases in each group.Therewereno dropouts throughoutthe intervention. There wereno significant differences in the general data such as gender and age between the two groups (bothP>0.05), indicating the comparability (Table 1).

Table 1.Comparisonof the general data
2 Treatment Methods
2.1 Combination group
2.1.1 Sinew-bone balancing manipulation
Sinew-adjusting manipulation:AppliedAnrou- pressing andkneadingandTanbo-plucking manipulations to the tense muscles including the major and minor pectoralis muscles, upper trapezius muscle,levator scapula,sternocleidomastoidandrhomboid,especially wherestiff andpainfulnodules were felt (Figure 1).
Cervicalspinebalancing manipulation:First step,fixedthespots.Taking C2spinousprocesstilting towards the right side as an example, the patient took a supine position and the practitioner stood by the right side of the patient’s head, forming 45° with the patient.The patient lifted his chin by 30° and turned his head left by 45° (Figure 2). Second step, fixed the positions.The practitioner held the patient by the chin naturally with his left hand, using the palm to fix the chin and the left forearm to support the left occipitotemporal region of the patient. The physician then cupped his right hand,with the radial side of the index finger supporting the posterior nodeof the right transverse processand spinousprocess of C2, the thumbbelly pressing the mastoidprocess,andtherestfingerscovering the occipitalbone(Figure 3).Directionof force:the physician moved his right elbow towards left with the shoulder and extensors of the upper arm, passing the force through the fixed wrist, metacarpophalangeal and interphalangeal joints to the radial side of the index finger belly to push C2to shift laterally by 2-3 mm at a high speed. The feeling of joint shifting or a ‘click’ sound from the joint shifting indicated the completion of the manipulation.Other vertebraeof thecervicalspine were treated following the same procedure but with the index finger belly attaching to the affected side of the vertebral body and different force direction.

Figure 2. Fixing spots in cervical spine balancing manipulation
Thoracic spine balancing manipulation:First step,fixed the spots. Taking adjusting T6as an example. The patient took a supine position with a thin pillow under the head, crossing the arms to hold the shoulders. The physicianstoodby theright sideandpressedthe patient’s folding elbows downwards. Second step, fixed the positions. With the left hand holding the patient’s shoulder,thepractitioner turnedthepatient’sbody towards right. At the same time, the physician put his right fist at the two sides of the spinous process of T6and asked the patient to lie down (Figure 4). Then the doctor held the neck of the patient from behind with hisleft hand and slightly lifted thepatient’sneck to extendthethoracic vertebrae forward.Directionof force: when feeling the tension produced by thoracic extension pass to the spinous process of T6, the doctor gently bent forward to press down the patient’s upper body. The force transmitted from the patient’s elbows to T6. The feeling of joint shifting or a ‘click’ sound from thejoint shifting indicatedthecompletionof the manipulation (Figure 5). Other segments of the thoracic spine were treated following the same procedure.
The above treatments were conducted once every other day for a total of 1monthby physicians from Tuina Department.

Figure 4.Fixing spots in thoracic spine balancing manipulation
2.1.2Exercisetherapy
The exercise therapy was performed following the manipulation therapy.
Stretching training:Whenflexing the elbows,the patient stretched the chest muscles with the assistance of a wall (or door frame), (Figure 6). The patient was also guided to do cervical spine exercises to stretch the levator scapula (Figure 7) and upper trapezius muscle(Figure8).Crossing thearms behindthehead,the patientlaterally forwardbent androtated theupper body tostretch thelatissimus dorsi(Figure9).Each movement should last for 30 s, 10 times as 1 set, and the patients were required to do 5 sets successively.
Intensivetraining:Anelasticstrapwasusedto strengthen the muscle force. When holding the strap withbothhandsandstretching it tillthemaximum range, keeping the upper arms close to the body and abdomen flat, the arms staying in a neutral position, the patient rotated the shoulders externally to intensify the external rotators of the shoulder (Figure 10). Held the elastic strap tightly to perform the movement of rowing a boat to train the middle and lower trapezius muscles and rhomboid (Figure 11). Wore the strap around the back,holding it tightly, to train the serratus anterior muscles with the shoulder girdle (Figure 12). With the elastic strap fixing thehead, thehead exerted force backward to fight against the strap to intensify the deep neck flexors (Figure 13). Each movement should last for 30 s, 5 times as 1 set, and the patients were required to perform 5-10 sets according to their endurance.

Figure 6.Stretching chest muscles

Figure 7.Stretching the levator scapula

Figure 8.Stretching the upper trapezius muscle

Figure 9. Stretching the latissimus dorsi

Figure 10. Strengthening the external rotator of the shoulder

Figure 11.Strengthening the middle and lower trapezius musclesand rhomboid

Figure 12.Training the serratus anterior muscles
Stretching cervicalspine: Thepatient took asupine position.Withayogaballunder the thoracic spine, the patientopenedthearms fromsides whilekeeping the head,shoulders andribs relaxed(Figure14),holding for 100 s,andthentook a 30 srest.Repeatedit for 5times successively.
Theaboveexerciseswerepracticedonceevery other day,for atotalof 1monthunder theguidance of the physician fromRehabilitationDepartment.

Figure 14. Stretching the thoracic spine
2.2 Exercise group
Patients in the exercise group only performed the same exercises as in the combination group.
3 Observation of Outcomes
3.1 Observation items
3.1.1Sagittal static postureassessment totalscore[6-7]The participant exposed the neck and shoulder skin.With the feet close to each other and heels in a line, the participant stood naturally with hands dropping down naturally. The evaluator stood right by the patient’s side and assessed the patient’s sagittal static posture. The assessment involved 6 sections: head posture, shoulder posture,scapular posture,slouchedback,abdomen posture and lumbar lordosis. Each section was scored accordingly: 0 point, normal postures; 1 point, slightly altered postures; 2 points, moderately altered postures;3 points, severely altered postures.
3.1.2 Static neck-shoulder posture assessment[8]
TheFHA andFSA wereassessed.Measurement methods: whilerelaxing the whole body, thepatient stood sideward in front of the posture assessment wall chart, looking straight forward, exposing the neck and shoulder skin, to take a photo[9]. Drew a vertical line through C7, and linked C7respectively with the center of the tragus and thepeak of the acromion. The angle betweentheverticallineand the linebetween the tragus and C7was defined as FHA; the angle between the vertical line and the line between the acromion and C7was defined as FSA. See Figure 15 for illustration.
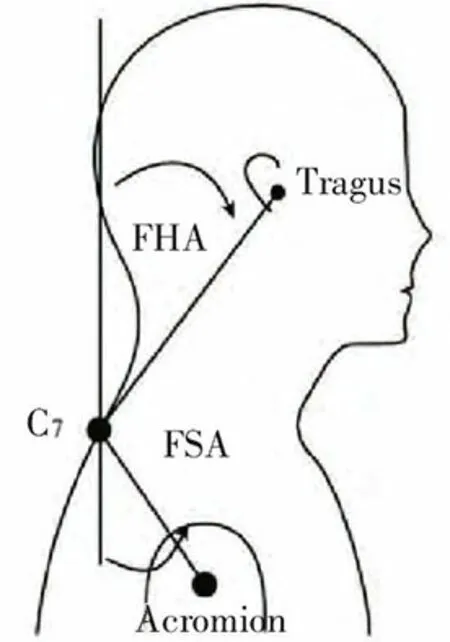
Figure 15. Illustration of the measurement of FSA and FHA
3.2 Treatment results
Beforetreatment,therewerenosignificant differencesinthesagittalstatic postureassessment totalscore,FSA andFHA betweenthetwogroups (allP>0.05).After treatment,the sagittalstatic posture assessmenttotalscore,FSA andFHA alldeclined significantly inthe twogroups (allP<0.01),andwere significantly lower inthecombinationgroupthaninthe exercisegroup(allP<0.01).Thedetails areshownin Table2-Table 4.
Table 2.Comparisonof the sagittal staticposture assessment total score( ±s, point)

Table 2.Comparisonof the sagittal staticposture assessment total score( ±s, point)
GroupnPre-treatment Post-treatment t-value P-value Combination 3010.43±1.17 4.80±1.0825.960 0.002 Exercise 3010.23±1.20 5.60±1.1123.1110.004 t-value -0.6412.781 P-value0.5240.007
Table 3.Comparisonof theFHA ( ±s,°)

Table 3.Comparisonof theFHA ( ±s,°)
GroupnPre-treatment Post-treatment t-valueP-value Combination 3041.57±4.10 32.23±2.7016.9220.001 Exercise 3041.70±3.7835.40±3.1519.1360.004 t-value 0.1294.110 P-value0.8980.004
Table 4.Comparisonof the FSA ( ±s, °)

Table 4.Comparisonof the FSA ( ±s, °)
GroupnPre-treatment Post-treatment t-valueP-value Combination 3049.53±4.26 38.77±3.4928.3630.001 Exercise 3049.33±3.57 42.73±3.4813.9340.003 t-value -0.1944.333 P-value0.8470.005
4 Discussion
UCS refers to a group of signs including head forward,roundedshoulders,hunchback,liftedshoulders,scapular forward extension, lifted scapula, and scapular winging caused by loss of biomechanical balance in the head, neck and shoulders[10]. UCS has not been adopted asanindependentclinicaldiagnosis inChinayet[11].Instead, it is often diagnosed as cervical spondylosis,cervical myofascitis, cervical muscle strain, etc. UCS gets its name from the ‘X’ shape formed by the imbalanced muscle groups in the neck, chest and back (tight major andminor pectoralismuscles,levator scapula,upper trapeziusmuscle,sternocleidomastoid,scalene and latissimus dorsi; weak deep neck muscles, middle and lower trapezius muscles,rhomboid,androtator cuff muscles). Spinal stability depends on both internal and external stabilities under normal physiological condition.The internal stability refers to the static balance, mainly realizedby the vertebralbodies,intervertebraldiscs,zygapophysialjointandLuschkajoint;theexternal stability refers tothedynamic balance,mainly maintainedby paravertebralmuscles[12-15].When the spinalexternalstability isdestroyedanddynamic balanceislost,theinternalstability structurewill change accordingly, which belongs to the scopes of ‘Jin ChuCao’and‘GuCuo Feng’intraditionalChinese medicine (TCM). ‘Jin Chu Cao’ means abnormal changes of sinews in the structure, location or function; ‘Gu Cuo Feng’refers to subluxationsof bonesand joints,resulting in limited range of motion of joints[16]. TCM holds that the movement of bones dependson the contraction and extension of sinews, while the sinews need the support of the bones to assist the body to move, and they work together to maintain a dynamic balance of the body[17-18].
Our researchgroupput forwardtheconcepts‘relaxation,correctionandstrengthening’toprevent and treat spine-relateddiseases. Theprevention and treatment of spine-related diseases should emphasize early intervention in both prevention and treatment. In thisstudy,thecombinationgroupfirst usedtuina manipulations to relax the overactive major and minor pectoralis muscles and levator scapula and the involved fascia,representing theconcept ‘relaxation’.At the sametime,basedonthetraditionaltuinaand chiropractic manipulations,precisebone-setting skills were usedtocorrect thedisplacedjoints,which indicated the concept ‘correction’. The sinew-regulating manipulations canmodulate the externalmechanical balance by promoting blood flow, dissolving stagnation,unblocking meridians and activating collaterals in the tense muscles; bone-setting manipulations can restore thestatic balance inside the cervical spine. The two treatments work together to finally let the bones stay in the right place and tendons pliable[19]. Exercise therapy can help strengthen the weakened muscles in UCS, such asrhomboid,middleandlower trapezius muscles,serratus anterior muscle, rotator cuff muscles and deep neck flexors, standing for the concept ‘strengthening’. It is anintegration of the therapist-guided training and self-rehabilitationtraining[20].Meanwhile,stretching trainings were added to stretch and correct the tense musclesto helprestorethebalancebetweenthe agonists and antagonists. The current study combined tuina,chiropractic andrehabilitationas awhole,in combination with the concepts of ‘relaxation, correction and strengthening’, to fully display the advantages of the Acupuncture-moxibustion and Tuina Rehabilitation Department.
By observing the sagittal static posture assessment total score, FHA and FSA before and after treatment,this study evaluated the effect of sinew-bone balancing manipulation plus exercise therapy on UCS postures. Of the outcomemeasures,althoughthesagittalstatic posture assessment total score is somewhat subjective,it can provide a comparatively overall evaluation of the abnormal postures in UCS patients and is a reflection of the concept of holism and ‘posture chains’[6]. FHA and FSA have beenwidely usedinclinic,withcertain reliability[21]. The results showed that the sagittal static assessment score,FSA andFHA declined significantly after treatment in both groups (allP<0.01) and were significantly lower in the combination group than in the exercise group (allP<0.01), suggesting that sinew-bone balancing manipulation combined with exercise therapy can produce more notable efficacy. This method is also well accepted by the primary school kids, so that it is worth promoting. Besides, we would like to remind the parents to pay attention to the postures of kids in daily life to prevent the creation and development of UCS.

Conflict of Interest The authorsdeclarethat there isnoconflict of interest.Acknowledgments Thiswork wassupported by Traditional Chinese MedicineScience Research Planning Key Project of Hunan Province(湖南省中医药科研计划项目重点课题,No.201907).Statement of Informed Consent Informed consent wasobtained from theguardiansof the kids.
Received:19September 2019/Accepted:24October 2019
猜你喜欢
杂志排行
Journal of Acupuncture and Tuina Science的其它文章
- Analysis of clinical application patterns in acupuncture-moxibustion treatment of Alzheimer disease
- Therapeutic observation on lung-clearing and spleen-strengthening tuina in children with exogenous cough
- Clinical observation on heat-sensitive moxibustion plus lactulose for postoperative constipation of mixed hemorrhoid due to spleen deficiency
- Therapeutic effect of heat-sensitive moxibustion plus medications for senile osteoporosis and its effect on serum BMP-2 and OPG levels
- Effects of electroacupuncture plus drug anesthesia on pain and stress response in patients after radical surgery for stomach cancer
- Therapeutic efficacy observation on auricular point sticking therapy for cardiac syndrome X in women