Establishment and management of neurosurgery emergency observation ward during the COVID‑19 epidemic period
2020-06-22HuiTingNIEZongYingZOUHuiZHANG
Hui‑Ting NIE, Zong‑Ying ZOU, Hui ZHANG
Department of Neurosurgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology,Wuhan, China
ABSTRACT
During the COVID‑19 epidemic period, the front‑line antiepidemic departments have attracted much attention.However, to meet people’s daily needs for the diagnosis and treatment, emergency department and intensive care unit are also the focus of work to control the source of infection, cut off the transmission route, and reduce the risk of novel coronavirus transmission while treating patients.In order to further strengthen the management, our department of neurosurgery took active measures in the emergency treatment for patients and summarized the coping strategies and relevant experience from the aspects of establishment of emergency observation wards, medical staff management,patients and family management, daily environment and object surface disinfection management, material management, and nursing quality management, hoping to provide reference for the nursing management of emergency wards after the outbreak of public health emergencies.
Keywords: COVID-19, neurosurgery emergency observation wards, nursing management, public health emergencies
COVID‑19 is strongly infectious, with the wide range of transmission.Patients with COVID‑19 are the main infectious source, whereas asymptomatic carries may be infectious source.[1]According to the Law of the People’s Republic of China on Prevention and Treatment of Infectious Diseases, the National Health Committee of the People’s Republic of China classified COVID‑19 as Class B infectious disease on January 20, 2020, and took the control measures of Class A infectious disease to manage the disease.[2]Under the deployment of the National Health Committee,our department of neurosurgery, as national key clinical specialty, successfully transformed general wards with 43 beds into an emergency observation isolation ward with 15 beds within 24 h to accommodate the patients who need hospitalization after being checked during the COVID‑19 epidemic period.In this article, we mainly summarized the establishment and management of neurosurgery emergency observation wards, and thought that effectively doing prevention work well not only protected doctors and nurses from infection but also promoted the recovery of patients.
ESTABLISHMENT OF OBSERVATION WARD
The layout and transformation of observation ward
Based on the mandatory requirements of the superior administrative departments, we implemented flexible work on the layout and transformation of observation ward during the COVID‑19 epidemic period by analyzing the practical situations of inpatient ward of our department.According to the standards for the establishment of infectious inpatient wards and strict requirements of division of infectious areas,the original inpatient wards were transformed into three areas and two routes [Figure 1].The three areas refer to clean, potential contaminated, and contaminated areas while two routes refer to passage for medical staff and passage for patients.Between clean area and potential contaminated area and between potential contaminated area and contaminated area are buffer zones which help avoid cross contact of doctor–patient and in‑out process of articles.Observation ward needed to strictly follow hospital infection protective requirements as follows: A patient in the stable condition should be arranged in a single ward; medical staffs should take secondary protective measures; drugs and all worker staff should have clean passage while patients and specimens have their channel; a totally closed administration should be implemented in the observation ward, with the front door normally closed and specially‑assigned person watch over,and access control system should be set up to only allow working staff with authority to enter the observation ward.
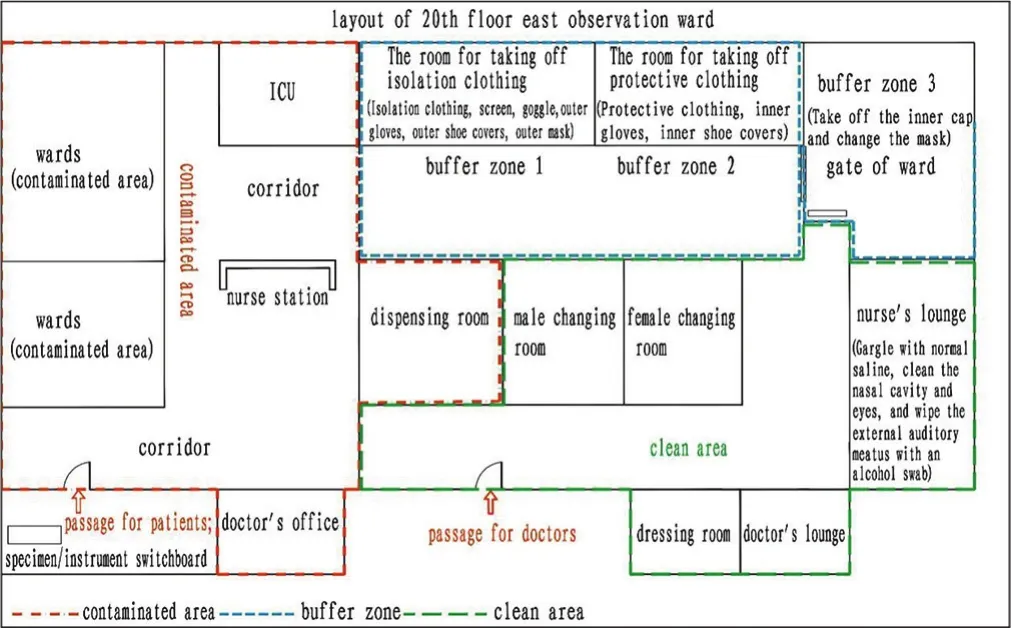
Figure 1: The diagram of observation ward after transformation.Notes:Dressing room is a place where medical staff wear protective equipment,such as protective clothing, isolation clothing and other protective articles after changing their working clothes in the changing room
Intensive care unit
The six‑persons ward was transformed into 4‑persons intensive care unit (ICU) with the distance between beds≥2 m, which was set up in the corridor in the inpatient ward where the working staff come in and out centrally to help nurses to observe the patients’ condition.The curtain was used between the beds.In addition, ICU is equipped with first‑aid equipment and routine nursing equipment,such as separate rescue carriage, defibrillator, invasive ventilator, high‑flow humidifying oxygen therapy instrument,electrocardiograph, infusion pump, enteral feeding pump,and blood‑gas analyzer.
Personnel allocation
Doctors are routinely assigned to first‑line, second‑line, and third‑line shifts, and second‑line doctors are responsible for 24‑h consultation of emergency patients.The 26 nurses in inpatient ward were divided into eight groups,three nurses (including a group leader) in each group, and working around the clock in four shifts (morning shift,evening shift, former night shift, and later night shift).Moreover, the other two auxiliary nurses were responsible for the treatment work of the main shift.As for personnel arrangement of each group, a comprehensive consideration should be given to the individual’s professional title and professional ability to make a rational personnel allocation in each group.Each group leader needed to be responsible for critically ill patients be in charge of working arrangement and cooperation for each shift, as well as concern dynamic physical and mental health of group members.In addition,because of high air tightness of multi‑layer protection during the second‑level protection, chest tightness and fatigue are easy to occur, so the nurses who entered the contaminated area had to adopt a pattern of “one helping another” to avoid such situation.Moreover, according to the number of patients in hospital, a standby shift was set up everyday in case of emergency.Last but not least, the psychological intervention group composed of medical personnel who have obtained the qualification of psychological counselor was established to timely participate in psychological counseling tasks to solve the psychological problems of inpatients and their families.
WARD MANAGEMENT
Management of patients
According toRegulationsonResponsestoPublicHealth Emergencies[3]andDiagnosisandTreatmentProtocolfor COVID-19(TrialVersion6),[1]our department formulated workflow system related with neurosurgery medical characteristics, includingEmergencyCasesConsultationSystem DuringtheEpidemicOutbreakandPreventionandControl ManagementofIn-hospitalPatientsinNeurosurgeryEpidemic ObservationWard.As per workflow system, all newly admitted patients should be screened for novel coronavirus.First,the initial screening should be completed in the outpatient department.If the patient is critically ill and in need of emergency treatment, screening can be conducted in the observation area with strict protective measures.Second,patients should have their body temperature examined at least twice a day, and those with suspected signs should undergo computed tomography (CT) and nucleic acid tests in time.Third, only after consultation by the core group through testing and screening to explicitly exclude virus infection can the patients in the observation ward be transferred to the general ward.Fourth, if a patient in the observation ward is found to be suspected or diagnosed after screening, he/she shall be reported to the medical service office in a timely manner and initiate the mechanism of expert consultation and referral [Figure 2].
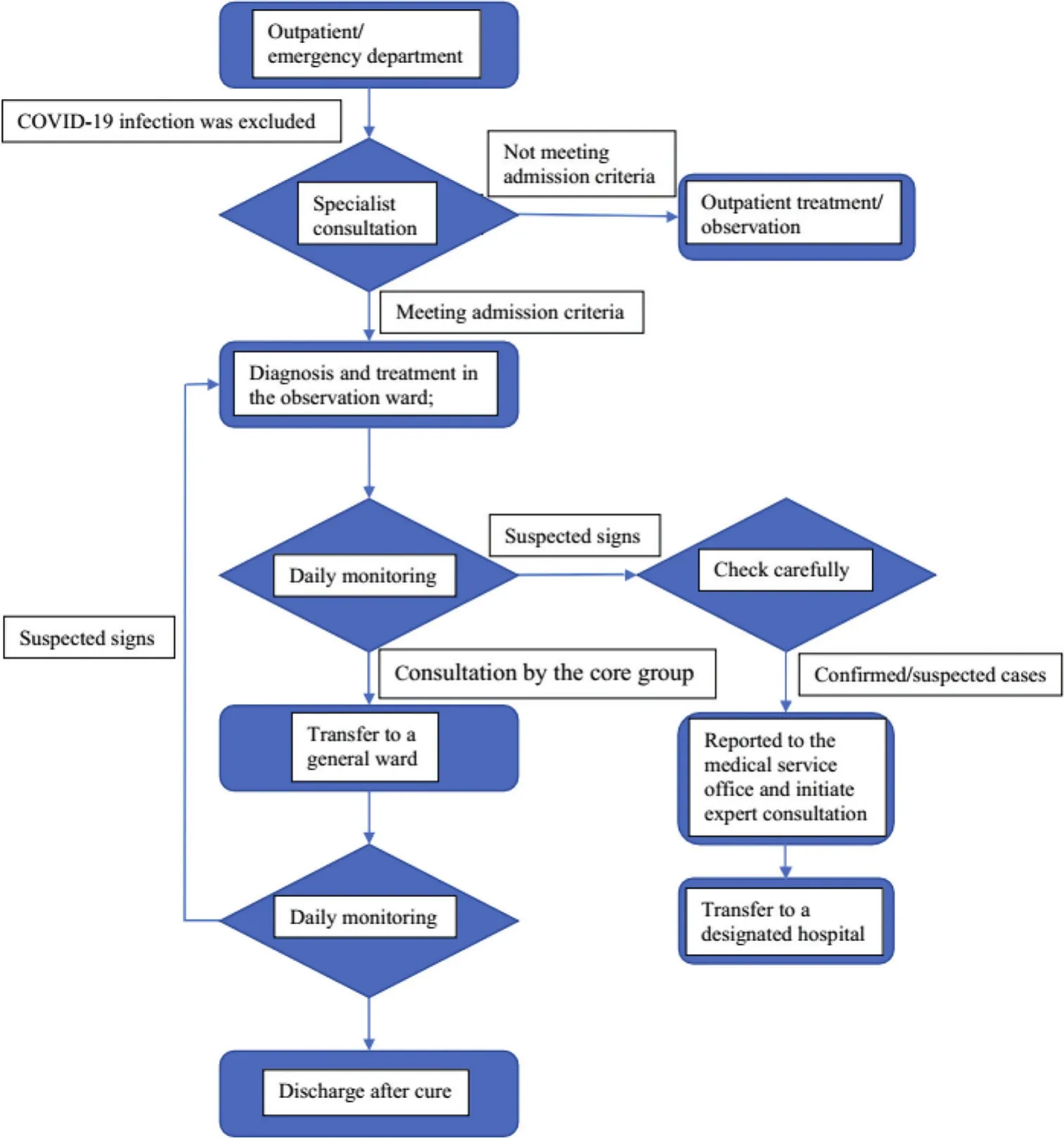
Figure 2: Management flow chart of patients in the neurosurgery observation ward
Management of caregivers
During the epidemic period, each patient should stay with a fixed caregiver (generally family member).Only after being excluded from novel coronavirus infection by outpatient CT and nucleic acid testing can the caregiver enter the ward.Without inspection and permission to go out, patients and their caregivers in the ward are not allowed to leave, go in and out the ward at will, or visit other ward.Daily meals for them were brought by the caterer to the reception desk in the lobby of the ward and then brought to the ward by the assistant nurses.Provide protective equipment for patients and their caregivers, such as masks and hand sanitizers, as appropriate.The body temperature of their caregivers should be taken twice a day and registered.If the caregivers are found to be suspected or diagnosed after screening, the medical personnel should immediately ask them to go to the designated hospital and report to the medical affairs office in time [Figure 3].Attentions were paid to humanistic care and education:Strengthen the communication with patients and their families to timely understand their needs and provide help for them; publicize COVID‑19 prevention and control and management knowledge through various forms every day,such as radio, TV, and video; nurses regularly ask patients and their families about their needs for living supplies, and a specially‑assigned staff will go to the supermarket on the first floor to help them purchase.If hospitalization renewal payment, it is recommended to use Alipay or WeChat to renew the payment; if discharge, the nurse or nurse assistant accompanies the patients and their families to the checkout center for discharge.
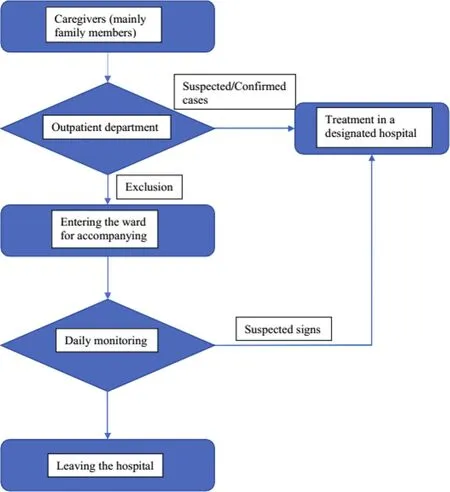
Figure 3: Management flow chart of caregivers in the neurosurgery observation ward
Ward disinfection and isolation management
Current studies have shown that the virus is sensitive to ultraviolet rays and heat (56 0C for 30 min), and 75% ethanol and chlorine‑containing disinfectant can effectively inactivate the virus as well.[1]Therefore, the department should do a good job of the disinfection for the ward.(1) Air disinfection:The window should be opened to ventilate the room at least 2 times a day, 30 min each time, or a ultraviolet air sterilizer with recirculating air is used for disinfection 4 times a day,2 h and each time.(2) Disinfection of object surface and the ground: Beds, bedside table, bedside chair, nurse station,the doctor’s office, lounge, and so on need to be wiped with 1000 mg/L effective chlorine‑containing disinfectant,or with a disposable paper towel to disinfect 2 times a day.All the toilets in the ward should be soaked with 5000 mg/L chlorine‑containing disinfectant for 30 min, then washed clean.Cleaning tools, including duster and mop, should be only used in a special room and special area.After use, they should be sealed in a double‑layer yellow garbage bag for centralized treatment.(3) Disinfection of medical instruments:Stethoscope, infusion pump, blood pressure monitor, and other commonly used items should be thoroughly wiped with 1000 mg/L effective chlorine‑containing disinfectant after each use.The thermometer should be soaked with 1000 mg/L effective chlorine‑containing disinfectant for 30 min after each use, then cleaned and dried for standby application.(4) The reusable medical instruments (such as goggles) should be soaked in 1000 mg/L chlorine‑containing disinfectant for 30 min immediately after use, then packed in double‑layer plastic bags, and sent to the disinfection supply center for the treatment.The handover records should be made.(5) Disinfection of fabrics: The patient’s bed sheet,quilt cover, and other fabrics after use are put into an orange special bag and sealed, and then sent to the washing center for cleaning and disinfection.(6) Medical waste disposal:Patients’ household garbage and medical garbage must be sealed in double‑layer yellow garbage bags and disposed of as infected garbage.(7) Disposal of the patient’s corpse: The dead patient’s body should be immediately sprayed with 3000 mg/L effective chlorine‑containing disinfectant.Moreover,such the patient’s orifices as mouth, nose, ears, and anus should be filled with 3000 mg/L effective chlorine‑containing disinfectant or 0.5% peroxyacetic acid cotton ball or gauze.After that, the body are wrapped in a double‑layer cloth sheet,put in a double‑layer body bag, and sent in a special vehicle to the designated place for cremation.Each disinfection was recorded.
NURSING MANAGEMENT
Strict protection training and management
By shooting video of “how to do a protection job well in the management of critically ill patients admitted in general wards during the COVID‑19 outbreak”, the head nurse and teaching supervisor demonstrated to the working staff the whole processes of how to wear protective equipment properly according to the instructions from worker elevator to the clean area to the contaminated area and how to go through the buffer areas after work and take off protective equipment as per the instructions back to the clean area to do personal hygiene well.The working staff had to punch in to learn the video content and had examinations.The group leader was trained on a point‑by‑point basis.After being checked, they would guide and check the team members.It is important to set up a training wall in the clean area and post relevant information on COVID‑19 prevention and control for everyone to read and learn independently.The senior teachers with front‑line experience in fighting the epidemic served as a safety supervision class to supervise whether the protective equipment are properly put on and taken off,and particularly provide one‑to‑one guidance for cleaning logistics personnel.Every staff should go through strict clothing inspection to make sure there is no problem in wearing the equipment before entering the contaminated area.The staffs on duty on the day were organized to learn about the division of the ward environment, the use of protective equipment and articles, the requirements of disinfection and isolation specifications, the emergency plan for occupational exposure, and the procedures for handling the bodies of the dead patients.The teachers in safety supervision class also supervise the disinfection situations of the ground, object surface and air in the ward,and the standard disposal of medical waste at each shift of cleaning staff and medical staff, find their weakness, and help them correct their mistakes in time, thus to ensure the safety of all the staffs and patients in the ward.
Strict implementation of standard protection
The standard prevention and protection was strictly implemented: (1) The medical staff of our department must wear working clothes, disposable working caps, disposable gloves, medical disposable protective clothing (in accordance with national or European standards), medical protective masks, goggles/protective face shield, and shoe covers in strict accordance with the second‑level protection requirements to avoid cross‑infection.(2) According to the requirements ofGuidelinesontheuseofcommonmedicalprotectiveequipment inthepreventionandcontrolofCOVID-19(Trial),[4]the daily temperature register for staff on duty was established,temperature taking twice a day; those with clinical symptoms or suspected cases should be conducted with etiological detection immediately; the head nurse inquired every day to learn about the exposure of medical personnel, handled and reported occupational exposure according to the requirements of the hospital.(3) The staff and the patients’family members have meals distributed by the nutrition center of the hospital.They are separated from each other at meals and wear masks after eating.The staff must wash their hair with hot water and wash their hands with running water after work.[5]It is necessary to surpervise the cleaning staff and catering staff to standardize the treatment of medical waste and blood and body fluid specimens.
Management of protective supplies
it is required to strictly implement the provisions on the management of medical consumables, strengthen the storehouse management, scientifically and rationally allocate protective equipment, and verify the quantity of existing protective equipment (e.g., medical protective masks,surgical masks/caps, goggles, protective face shields, gloves,protective clothing, isolation clothing) in the department.It is better to check the items every day, and ask the materials department to get them in advance if the protective materials are insufficient.
Nursing quality management
During the epidemic period, nursing staff should pay more attention to epidemic prevention.The head nurse could not relax the quality and safety management of daily nursing work in the ward.It is necessary to arrange the shift dynamically and flexibly according to the workload of the ward and to strengthen the implementation of the nursing core system and self‑check of quality.The bedside rounds of patients were carried out every day, and the “ten knowns” and “key points of nursing” of critically ill patients were transferred from one shift to another.The daily dynamic feedback in the ward was given to everyone in the WeChat group to ensure the safe development of nursing work and timely feedback of key problems to the head nurse and nursing department.
PSYCHOLOGICAL SUPPORT TO MEDICAL STAFF
Some medical staff have never directly faced the occurrence of a public health emergency, so the outbreak of this epidemic caused intense psychological stress to them.Since they need to receive various emergency treatment training, physical fatigue is also an important factor leading to psychological stress of nurses in the ward.[6]Therefore, while paying attention to the psychological changes of neurosurgical emergency patients, we should also pay attention to the physical and mental health of clinical medical staff.Nurses with poor psychological status should be given appropriate rest and adjustment.Meanwhile, psychological counseling should be carried out in the ward.Nurses who have difficulties in family life should be given help through the labor union.
CONCLUSION
During the epidemic period of COVID‑19, our department has taken a series of active emergency measures, including replanning the layout of the ward, sorting out the management system and work process in line with the epidemic period,strictly implementing disinfection and protection measures,and paying attention to the psychological intervention of medical staff, so no medical staff or patients in the ward has been infected in hospital.In the future work, nursing team also need to set up a perfect nursing emergency rescue system to ensure the quality of nursing management from the aspects of the materials, technology, workforce and infection control, guarantee timely response to emergency care and complete the nursing work with high quality and high efficiency.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
杂志排行

Journal of Integrative Nursing的其它文章
- The relationship between diabetes‑related distress and self‑management in empty‑nest elderly patients with type 2 diabetes mellitus: The mediating effect of self‑efficacy
- Impact of the emigration of nurses on health care delivery system in selected hospitals, Benin‑City, Edo State, Nigeria
- A bibliometric analysis of nursing research in COVID‑19 in China
- Effect of flapping‑meridians combined with thunder‑fire moxibustion on upper limb dysfunction after stroke
- Clinical effect of scraping therapy in the treatment of knee osteoarthritis
- Competence investigation on insulation testing on electrosurgical instruments and needs analysis of training for Central Sterile Supply Department staff