Medical management of metabolic and cardiovascular complications after liver transplantation
2020-06-08ChiaraBecchettiMelisaDirchwolfVanessaBanzJeanFranoisDufour
Chiara Becchetti, Melisa Dirchwolf, Vanessa Banz, Jean-François Dufour
Abstract Liver transplantation represents the only curative option for patients with endstage liver disease, fulminant hepatitis and advanced hepatocellular carcinoma.Even though major advances in transplantation in the last decades have achieved excellent survival rates in the early post-transplantation period, long-term survival is hampered by the lack of improvement in survival in the late post transplantation period (over 5 years after transplantation). The main etiologies for late mortality are malignancies and cardiovascular complications. The latter are increasingly prevalent in liver transplant recipients due to the development or worsening of metabolic syndrome and all its components (arterial hypertension, dyslipidemia, obesity, renal injury, etc.). These comorbidities result from a combination of pre-liver transplant features, immunosuppressive agent side-effects, changes in metabolism and hemodynamics after liver transplantation and the adoption of a sedentary lifestyle. In this review we describe the most prevalent metabolic and cardiovascular complications present after liver transplantation, as well as proposing management strategies.
Key words: Solid organ transplantation; Hypertension; New-onset diabetes after transplantation; Obesity; Orthotopic liver transplantation; Post-transplantation metabolic syndrome
INTRODUCTION
Liver transplantation represents the only curative treatment option for end-stage liver disease, chosen cases of acute liver failure and selected patients with hepatocellular carcinoma, providing patients with a complete recovery of their liver function with excellent survival and quality of life[1,2]. Advances in surgical techniques and postoperative medical management have resulted in very good early post-transplant survival rates in the last decades; however, late mortality has remained unchanged[3].In Europe current reported survival rates are 83%, 71%, 61% and 51% at 1, 5, 10 and 15 years, respectively, with rates increasing up to 86% at 1-year and 74% at 5-year if the period from 2010 to 2014 is considered[4]. Similarly, data from the United States indicates 85%, 68% and 50% 1-year, 5-year and 10-year survival rates after liver transplantation, respectively, with significant differences according to the etiology of the underlying liver disease[5]. These excellent survival rates in the early posttransplantation period underline the importance of understanding the causes and risk factors for late post-transplant mortality, in order to improve overall survival.
Late mortality is traditionally defined as death occurring 5 years or more after liver transplantation[6]. Late mortality is predominantly not related to the liver graft (63%),with high rates of cardiovascular causes and malignancies[7]. Although these findings are in keeping with the main causes of mortality of the general population, patients who underwent liver transplantation show higher risk for developing metabolic,cardiovascular and neoplastic complications[8]. This is partially explained by the need for chronic immunosuppressive drugs, the majority of which are associated with the worsening or development of new-onset hypertension, dyslipidemia and diabetes[9,10].However, the massive adoption of the Western-world lifestyle and diet have dramatically affected metabolic changes, predisposing and increasing the development of cardiovascular diseases[11]. Therefore, the unmet goal in the management of the post-liver transplantation follow-up is the prevention of these long-term complications. In this review, we aim to review the prevalence of these lateonset complications, their impact on post-transplant morbidity and mortality, and the optimal management currently available.
METABOLIC SYNDROME
Metabolic syndrome is defined as a cluster of interrelated risk factors of metabolic origin, involving insulin resistance and inflammation, which directly promote the development of atherosclerotic cardiovascular disease and type 2 diabetes mellitus[12].There are different definitions, but most of them consider hypertension, obesity,dyslipidemia, and diabetes mellitus as the main components of metabolic syndrome.Its initial defining criteria, known as the World Health Organization criteria, have not been consistently used because of the need to measure serum insulin and urinary microalbumin to allow for the diagnosis, two expensive analyses[13]. Later on, the Third Report of the National Cholesterol Education Program and the Adult Treatment Panel III[14], proposed a more practical classification (initially described in 2001 and successively revised in 2006[12]), that was widely accepted by the scientific community.According to the National Cholesterol Education Program and the Adult Treatment Panel III modified classification, metabolic syndrome is diagnosed when at least ≥ 3 of the following criteria are met: (1) Impaired glucose tolerance: Fasting plasma glucose≥ 100 mg/dL (5.6 mmol/L); (2) Abdominal obesity: Waist circumference > 102 cm (40 in) in men, > 88 cm (35 in) in women; (3) Hypertriglyceridemia: ≥ 150 mg/dL (1.7 mmol/L) or drug treatment for high triglycerides; (4) Low levels of high-density lipoproteins (HDL): < 40 mg/dL (1 mmol/L) in men, < 50 mg/dL (1.3 mmol/L) in women or drug treatment for low HDL; and (5) High blood pressure: ≥ 130/85 mmHg or drug treatment for hypertension.
Although originally these considerations on metabolic syndrome were described for the general population, they are currently also adopted in transplanted patients.Another attempt to classify this syndrome was made in 2005 by the International Diabetes Federation criteria, establishing specific national cut-offs, in order to make the classification uniform all over the world[15].
The prevalence of metabolic syndrome is higher in liver transplant recipients when compared to the general population. Retrospective studies assessing the presence of metabolic syndrome post liver transplantation detected this problem in 43%-58% of recipients[16], compared to 30% of non-transplanted patients, with slight variations according to different geographical areas[17]. A recent meta-analysis evaluated eight original publications on metabolic syndrome after liver transplantation, underlining some modifiable and non-modifiable risk factors[16]. Male gender, and components present prior to transplantation such as high BMI[18], type 2 diabetes mellitus[19]and hypertension were all related to the development ofde novometabolic syndrome. In particular, patients suffering from diabetes mellitus before transplantation had a sixfold higher risk for developingde novometabolic syndrome[19]. When considering the etiology of the underlying liver disease resulting in the indication for liver transplantation, patients affected by hepatitis C, cryptogenic cirrhosis [group that possibly could include patients with misdiagnosed non-alcoholic steatohepatitis(NASH)] and alcohol related cirrhosis were at higher risk of developing metabolic syndrome after liver transplantation[16,19].
Although the data are not completely conclusive on the effect of immunosuppressive therapy on metabolic syndrome, the metabolic effects of these drugs are well established. Prolonged exposure to these drugs may increase the risk of metabolic complications and/or affect the reversibility of comorbidities present before transplantation. Corticosteroids, usually used in the early post-transplant phase, can act directly on pancreas beta cells increasing insulin resistance, while calcineurin inhibitors can affect the development both of diabetes mellitus (particularly for tacrolimus) and of hypertension (mainly true for cyclosporine). Dyslipidemia is often related to the use of mammalian target of rapamycin (mTOR) inhibitors, whereas the use of anti-metabolites such as mycophenolate have fewer detrimental effects on metabolic syndrome related comorbidities[20]. Considering that all these metabolic side effects are related to immunosuppression, it is reasonable to think that these agents may be the cause of metabolic syndrome. Nevertheless, there is no robust data to support this relationship[21]. Minimizing the effective dose of immunosuppression and supporting a healthy lifestyle are all measures recommended in order to prevent and reduce the development of metabolic syndrome and its related comorbidities.
In the general population, metabolic syndrome is recognized as an independent risk factor for cardiovascular morbidity and mortality. Regardless of the single components of metabolic syndrome, which represent themselves cardiovascular risk factors, metabolic syndrome is a cluster of metabolic dysfunctions that play a multiplicative impact on cardiovascular prognosis[22]. In keeping with these findings,metabolic syndrome has been extensively studied in the setting of liver transplantation. In the aforementioned meta-analysis by Liet al[16], liver transplant recipients patients with metabolic syndrome exhibited a higher rate of cardiovascular events, but not poorer survival rates. Patients who are at high risk of developing metabolic syndrome after liver transplantation should undergo regular surveillance in order to achieve an earlier diagnosis and treatment. An early diagnosis of metabolic syndrome will limit possible comorbidities, thereby reducing the risk of cardiovascular events. Additionally, patients who develop metabolic syndrome after liver transplantation are at a higher risk of developing graft steatosis, leading to an increase in the recurrence or in the development ofde novonon-alcoholic fatty liver disease (NAFLD). NAFLDde novorates range from 20% to 40%[23], but they can increase to 78% when we consider patients transplanted for NASH[24]. This wide variability depends on the methodology used for liver steatosis diagnosis[25].Nevertheless, in the majority of cases, the recurrence of NAFLD and NASH are harmless, without an evolution towards cirrhosis[26]. Notably, patients with recurrent NAFLD/NASH are more prone to develop cardiovascular comorbidities, type 2 diabetes mellitus and suffer from increased infection-related morbidity and mortality[27]. Interestingly, recipient genetic predisposition might play a role in the recurrence of NAFLD and NASH. The presence of the rs738409-G allele of the patatinlike phospholipase in liver transplant recipients represents an independent risk factor for post-procedure development of obesity and steatosis[28].
DIABETES MELLITUS TYPE II
New-onset diabetes mellitus type II after-liver transplantation is increasingly recognized as a complication of solid organ transplantation. It is defined by a hemoglobin A1c (HbA1c) level ≥ 6.5% in the transplanted populations[29]. Data on the prevalence of type 2 diabetes in patients after liver transplantation are still controversial. This is due to the heterogeneity of the criteria used for the diagnosis of diabetes mellitus and to the variability in the follow-up time points in the different studies. Nevertheless, the prevalence of type 2 diabetes mellitus ranges from 31% to 38% in post-liver transplantation patients, while the incidence of new onset type 2 diabetes ranges from 13% to 28% in the first three years following transplantation[29,30].Diabetes mellitus has been demonstrated to have significant consequences in both the early and late post-liver transplantation periods. When present, it was associated with a higher 10-year mortality, compared to non-diabetic liver transplant patients[31].
Patients with diabetes mellitus are more prone to experience complications with an increased risk of cardiovascular events, nephropathy, infections and death[32]. In addition, they experience a higher number of acute rejection episodes compared with non-diabetic patients, with higher rates of graft lost[33]. There are several wellestablished risk factors associated with the development of diabetes after liver transplantation. Male gender[34], ethnicity, family history[35], hepatitis C[36],citomegalovirus infections[10], and immunosuppressive drugs significantly contribute to the development of new-onset diabetes mellitus or worsening of pre-existing diabetes.
Among the available immunosuppressive drugs, corticosteroids are undisputedly known to increase the risk of new-onset diabetes in a length and dose-dependent manner[37]. This diabetogenic effect represents one of the most worrisome side-effects of glucocorticoids, justifying a strategy of rapid steroid withdrawal. Calcineurininhibitors also have a known diabetogenic effect, by directly damaging pancreatic islets cells. Although tacrolimus and cyclosporine share this mechanism of damage,the risk of developing or worsening of diabetes is significantly higher with tacrolimus than with cyclosporine (16.6%vs9.8%, respectively), valid findings for all solid organ recipients[38]. There is convincing evidence from the non-liver transplant population that target glycemic levels significantly reduces morbidity and mortality in patients with type 2 diabetes mellitus[39]. Although this approach has not been specifically proven in the liver transplant population, and little information exists on the use of anti-diabetic drugs in this subset of patients, it is reasonable to assume that euglycemic status is a goal to achieve in post-liver transplantation management.Expert consensus and guideline recommendations suggest screening transplanted patients with basal glycaemia at weekly intervals during the first month following transplantation and subsequently at 3, 6, and 12 mo, with additional annual screening of diabetic complications[35,40]. The oral glucose test remains the best available test to definitely assess new-onset diabetes mellitus[41]. It should be noted that diagnosis of new-onset diabetes is not feasible in the first two months after liver transplantation[41],since in the immediate post-transplant period, insulin requirement is usually increased, being the safest and most effective therapy to treat hyperglycemia.However, once patients have returned to a regular eating pattern and stable immunosuppression, hyperglycemia may either disappear or, in the case of new onset diabetes mellitus, persist. In concordance, use of HbA1c test is recommended 3 mo post-liver transplantation due to possible peri-transplantation transfusions that render the test invalid[40]. The goal for transplanted patients with established type 2 diabetes mellitus should be an HbA1c level of less than 6.5%-7%[35]. An HbA1c level < 6.5% is recommended for patients with a shorter disease duration, younger age and fewer comorbidities. In older patients with multiple comorbidities and a high risk of hypoglycemia, an HbA1c of < 8.0% is considered a safer goal[42]. At present, there is insufficient data to recommend a specific algorithm of anti-diabetic agents in posttransplant diabetes mellitus, as studies addressing this specific population are lacking.However, if current guidelines for the treatment of type 2 diabetes in the general population are extrapolated to liver transplant patients, the choice of the antihyperglycemic agent should be tailored to patients' preference and clinical characteristics[43]. Lifestyle changes represent the first line treatment for glycemic control, starting with a balanced diet low in calories and simple carbohydrates accompanied by moderate exercise, although this is often difficult in this patient population with general frailty persisting many years post-liver transplantation.When these measures are not sufficiently effective, pharmacological therapy with hypoglycemic agents and/or insulin needs to be considered. As the majority of oral diabetic medications are metabolized in the liver, they should be used with caution in patients in whom graft function is reduced[44]. Rosiglitazone, pioglitazone and sulfonylureas have been studied in the post-transplant population showing a possible minimization in insulin requirement[45,46]. Pioglitazone might also be considered in patients at risk of developingde novoor recurrent NAFLD after liver transplantation[47]. Metformin has not been extensively studied in the post-liver transplant setting despite its common use as the first-line therapy choice in type 2 diabetes. A single retrospective analysis of 24 renal transplant recipients treated with metformin reported a high rate of drug discontinuation due to gastrointestinal complaints or an increase in serum creatinine. However, no serious adverse events or severe alteration in immunosuppression drug levels were recorded[48]. Interestingly,in vitroanalysis revealed that metformin optimally reverts diabetogenic genes that are dysregulated in the context of immunosuppression, which is something to take into account when evaluating the choice of therapy[49]. More recently, glucagon-like peptide-1 receptor agonist (GLP-1 RAs,i.e., liraglutide) and inhibitors of dipeptidyl peptidase 4 (DPP-4I or gliptins) were introduced as part of the current antidiabetic therapy. According to recent guidelines, GLP-1 RAs are recommended in the presence of established atherosclerotic cardiovascular disease and might be considered for their additive weight-loss properties. In this scenario, DPP-4I may also be useful because they do not affect body weight[50]. Sitagliptin or vildagliptin use after liver transplantation are not thought to have any significant effect on calcineurin inhibitor or mTOR inhibitor availability. A possible exception includes use of sitagliptin and cyclosporine as well as tacrolimus and vildagliptin, drug combinations that warrants further investigation[51,52]. Finally, there is next to no experience with sodium-glucose cotransporter type 2 (SGLT-2) inhibitors (i.e., canagliflozin, dapagliflozin and empagliflozin) in the setting of liver transplantation. All these drugs work by increasing urinary glucose excretion and are considered highly safe. Nevertheless, we have to consider that SGLT-2 inhibitors are associated with an increased risk of genital and urinary (the latter only for high doses of dapagliflozin) tract infections[53],leading to some controversy in a possible use in liver transplant patients. Moreover,drug elimination mainly occurs through hepatic and biliary excretion, making difficult the use of this medication when liver enzymes alterations are present[50]. The use of SGLT-2 inhibitors may have a positive effect in the setting of heart failure or renal impairment, with a specific dose adjustment needed according to renal function[50]. However, the only direct assessment of the potential interaction with immunosuppressive drugs to date was described in a study including healthy volunteers. Co-administration of cyclosporine resulted in a 23% increase in the mean canagliflozin area under the operating curve (AUC)[54]. The same mechanisms may result in an increased exposure to calcineurin inhibitors and mTOR inhibitors,although further studies are warranted to clarify this possible interaction. In addition,as impaired insulin secretion is a major determinant for liver transplantation, when hepatogenous diabetes[55,56]is suspected, drugs capable to improve β-cell function such as incretins or SGLT-2 inhibitors might be considered.
If therapeutic goals are not met with lifestyle changes and oral anti-diabetic medication, or if the patient becomes metabolically decompensated (symptomatic hyperglycemia with ketosis), insulin must be administered[57]. Ideally, glucagon-like peptide-1 receptor agonists should be used, in combination with basal insulin, in order to reduce the insulin requirement.
In summary, in addition to pharmacological treatment of diabetes mellitus, the adjustment of immunosuppressive regimens can aid in reducing the risk of post-liver transplantation diabetes and improve glycemic control. The possible strategy to adopt consists in minimizing the use of corticosteroids or adopting cyclosporine rather than the more diabetogenic tacrolimus, as well as titrating tacrolimus by adding other immunosuppressive agents (i.e., mycophenolate mofetil or mTOR inhibitors). These possible combinations may help improve glycemic control[57]. Careful attention also needs to be taken into account with regard to other cofactors, such as the occurrence of graft rejection, the concomitant presence of renal failure,etc. As mentioned, all immunosuppressive regimen adjustments should be combined with lifestyle modifications, and a carefully selected antidiabetic therapy (Figure 1).
OBESITY

Figure 1 Proposal of a treatment algorithm for diabetes mellitus type ll in liver transplant recipients. GLP-1 RA: Glucagon-like peptide-1 receptor agonist;SGLT2 inhibitors: Sodium-glucose cotransporter type 2; DPP-4l: Inhibitors of dipeptidyl peptidase 4; NASH: Non-alcoholic steatohepatitis; NAFLD: Non-alcoholic fatty liver disease.
Obesity is defined by the World Health Organization as a body mass index (BMI) > 30 kg/m2and morbid obesity as a BMI of > 35 kg/m2[58]. In the past decade, obesity as a whole has progressively become a worldwide epidemic and a relevant comorbidity in the pre-liver transplant setting, with an overt adverse impact on the post-transplant outcome. Although dry weight is not always measurable in patients with decompensated cirrhosis, it is estimated that 15% to 30% of pre-transplant patients meet the criteria for obesity[59]. Following liver transplantation, weight gain tends to increase progressively over time. At one-year post-surgery, 33.7% of patients meet criteria for obesity, and by 5 years, 40.3% of patients are obese[60]. It is frequent that patients with a history of obesity prior to liver transplantation maintain this tendency after the surgical intervention. But additionally, one-third of patients with normal weight prior to transplantation become obese following the procedure[59]. Weight gain in the early post-transplantation period is related to several factors, such as an increased appetite as a result of the resolution of cirrhosis and thus, absence of a catabolic state, and the orexigenic effect of steroids. Risk factors for post-liver transplantation obesity include age greater than 50 years, obesity or type 2 diabetes prior to transplant and NASH as indication to liver transplantation[61]. Patients should be advised to achieve a healthy body weight prior to liver transplantation, as obesity is associated with numerous negative postoperative outcomes such as development of fatty deposits in the graft, development of diabetes, higher cardiovascular and oncogenic risk. Furthermore, patients should be made aware of the tendency to gain weight after transplantation and the problems associated herewith in order to adopt early preventive measures. Modulating immune suppression, such as adopting a regimen with a rapid withdrawal of steroids, is one of the possible strategies in patients at risk. However, it should be noted that steroids are needed not only in the early post-liver transplantation period, but also in the long-term follow-up as treatment of severe cellular rejection, where its use outweighs its associated risks.While corticosteroids are a well-known cause of weight increase, the effect of the exposure to the other available immunosuppressant drugs is not completely defined.Compared with tacrolimus, cyclosporine is associated with more weight gain in the first year following transplantation, whereas this difference is mitigated 2 years postliver transplantation[60]. Recently, in a randomized trial by Charltonet al[62], the authors found that an early introduction of everolimus with reduced-exposure to tacrolimus at 1 month post liver transplantation reduced weight gain assessed at 1 and 2 years post-liver transplantation. When this reduced-exposure to tacrolimus arm was compared with the absent-exposure to tacrolimus arm, the weight gain was even lower, suggesting a beneficial effect of isolated everolimus therapy. In addition to selecting the best immunosuppression therapy, the fundamental approach to treat and prevent weight gain are lifestyle modifications. Supervised physical activity is considered safe and effective in stable liver transplant recipients[63]. It is proven that increasing aerobic capacity and muscle strength has a favorable impact on glucose homeostasis[64]. There are studies that describe a modified behavior in food intake before and after liver transplantation, with a positive energy balance in the first year after the surgery[65]. Therefore, ongoing physical exercise and the adoption of a healthy low-calorie diet are essential for the management of obesity in the posttransplant setting. Similar to the goals in the pre-transplant setting, the objectives of treating obesity after liver transplantation are to prevent obesity-related comorbidities and mortality, as well as to reduce the incidence ofde novoNAFLD. When diet and exercise fail to achieve the proposed goal, pharmacologic therapies and/or bariatric surgery should be considered. Orlistat was tested in the post-liver transplant setting and was considered well-tolerated, safe, with no need for a close supervision of immunosuppressant drug levels, and dietary adherence. However, there was no significant evidence regarding its efficacy[66]. Liraglutide was recently approved for the treatment of obesity in non-diabetic patients[67], but to date there is no experience available in liver transplant recipients. Bariatric surgery is considered feasible, when indicated, although some issues remain. Potential problems include the presence of extensive adhesions, rendering surgery technically difficult, as well as the increased risk of wound complications in the setting of steroids or mTOR inhibitors[68].Whenever possible, steroids should be tapered and stopped and mTOR inhibitors switched to other immunosuppressive agents to reduce the risks of wound healing problems. In the published literature, only case series are available describing the implementation of this therapy in liver transplant recipients (Table 1). Despite weight loss being observed in all reported series (range 21%-75%), high complication rates(30-40% of complications > grade III of the classification of Clavien-Dindo)[69]were documented for all types of procedures, particularly for sleeve gastrectomy[70].Regarding mortality, there were no reports for sleeve gastrectomy, whereas gastric by-pass showed a mortality rate of 20%[71]. Regarding the pharmacokinetic of immunosuppressant drugs, studies have shown that the kinetics of tacrolimus and mycophenolate mofetil was not impacted by the performance of a sleeve gastrectomy[72]. On the other hand, patients with a gastric by-pass had significantly modified immunosuppressive drugs serum levels[73]. With currently limited data available on the effect of both bariatric surgery and pharmacological treatment on major outcomes such as survival in the post-liver transplant setting, diet and exercise are still considered the cornerstone treatment option for tackling and preventing weight gain.
DYSLIPIDEMIA
High blood lipid levels are unusual in the pre-liver transplant population, due to the impaired hepatic synthetic function in end-stage liver disease. On the other hand,dyslipidemia is a very common finding in the post-liver transplant setting. The definition of hyperlipidemia varies widely among different studies in the post-liver transplant era and only a few consider the standard NCEP-ATP III criteria. In view of this lack of standardization, dyslipidemia is reported as present in 45% to 71% of liver transplant recipients[74]. In most cases, hypertriglyceridemia occurs in the first six months after transplantation, maintaining its prevalence throughout the first year,while it decreases in subsequent years. On the other hand, hypercholesterolemia and low levels of high-density lipoprotein concentration appear later, with an increasing prevalence that affects about 30% of patients at the end of the first post-transplant year[74].
Dyslipidemia has multiple causes after liver transplantation that have been previously discussed in this review: Frequent body weight increase, poor glycemic control, genetic predisposition, donor related factors, early post-liver transplantation renal dysfunction[75]and the effect of immunosuppressant medication[76]. With regard to the latter, long-term corticosteroid use can contribute to hyperlipidemia[77].Cyclosporine is more frequently associated with hyperlipidemia (14%vs5%) and hypertriglyceridemia (49%vs17%) when compared to tacrolimus, with a dosedependent relationship[78]. The possible explanation for this cyclosporine effect is related to the inhibition of bile salt synthesis. In the case of tacrolimus, since this drug is known to cause hyperinsulinemia, this effect theoretically may lead to the development of hypertriglyceridemia. mTOR inhibitors are also known to increase

Table 1 Series reporting bariatric surgery after liver transplantation
the risk of hyperlipidemia (especially hypertriglyceridemia), through changes in insulin signaling pathways resulting in an excess of triglycerides production and secretion[79]. The combination therapy of mTOR inhibitors and tacrolimus results in lower rates of dyslipidemia[80], something also observed when switching from cyclosporine to tacrolimus[81]. Post-transplant dyslipidemia is generally resistant to dietary interventions, but it responds to traditional lipid-lowering agents. The most recent guidelines of the European Society of Cardiology[82]recommended the use of low-density lipoprotein concentrations (LDL-C) as the primary target for treatment of dyslipidemia, while for patients with elevated triglycerides, HDL-C is recommended as a secondary goal. In primary and secondary prevention for patients catalogued as having very-high risk for cardiovascular events, an LDL-C reduction of ≥ 50% from baseline and an LDL-C goal of < 1.4 mmol/L (< 55 mg/dL) are recommended,whereas in patients at high risk an LDL-C goal of < 1.8 mmol/L (< 70 mg/dL) is sufficient. This last version of the European Society of Cardiology guidelines dedicated a specific session on the management of dyslipidemia in solid organ recipients, although the recommendations are mostly based on studies on kidney recipients. They conclude that the management of dyslipidemia in transplant recipients should be comparable to that recommended for high or very-high risk patients, with an additional caution for possible drug-drug interactions (Figure 2).Statins are unanimously considered as a first line therapy for dyslipidemia in liver transplant patients, preferably pravastatin and fluvastatin because of the lack of interaction with cytochrome P450 and calcineurin inhibitors metabolization[21].Generally, cyclosporine increases the blood levels of all statins, even more so than tacrolimus. Nevertheless, statins, with particular reference to pravastatin, have been established to be safe, efficacious and well tolerated in solid organ transplant recipients[83]. The concomitant use of other drugs metabolized by the cytochrome CYP3A4 should be carefully used in patients receiving both calcineurin inhibitors and statins[82], because a perturbation in the cytochrome P450 metabolic pathway can increase immunosuppressive drugs toxicity[84]. Ezetimibe may be considered in recipients who do not tolerate statins, although the experience is scant[85]. Concomitant use of calcineurin inhibitors may result in increased statin levels in the blood. Isolated hypertriglyceridemia can also be present post- liver transplantation and it generally responds well to fish oil. Omega 3 has less drug-drug interactions with immunosuppressive therapy. In addition, omega 3 oil has other pleiotropic effects, such as anti-inflammatory and anti-proliferative properties, which can improve hepatic steatosis[86]. With regard to other lipid-lowering drugs, such as fibric acid derivatives,they are usually well tolerated, although there is scarce data available on their use in liver transplant patients. Importantly, the combination of fibrates with statin therapy increases the risk of myopathies and is thus not recommended. Patients on both these medications should be counseled regarding myalgia as a potential early symptom of rhabdomyolysis[87].
ARTERIAL HYPERTENSION
Arterial hypertension, which is defined as a systolic blood pressure greater than 140 mmHg and/or a diastolic blood pressure greater than 90 mmHg[88], occurs in 30%-50%of patients after liver transplantation, increasing up to 70% when evaluating patients in the long term[89,90]. Features such as high cardiac output, low systemic vascular resistance and low mean arterial pressure characterize end-stage liver disease. After patients are transplanted, this hemodynamic situation changes, leading to an increase in systemic blood pressure. Nevertheless, the etiology of post-liver transplantation hypertension is multifactorial and includes not only this change in hemodynamics,but also the use of immunosuppressive medications. These drugs are a well-known risk factor for hypertension, in particular calcineurin inhibitors. Although there are numerous pathogenetic mechanisms related to the development of hypertension in such patients, vasoconstriction seems to be the main causal factor. Vasoconstriction is caused by the excessive secretion of endothelin-1 and thromboxane and decreased production of prostacyclin, leading to an increase in sympathetic nervous system activity. In addition to these mechanisms, cyclosporine and tacrolimus act on sodium retention, resulting in an increase in effective-volume[90]. Nevertheless, cyclosporine seems to have a more deleterious effect compared to tacrolimus, showing a higher prevalence rate of arterial hypertension (73%vs63%, respectively)[91]. Glucocorticosteroids are also a known cofactor for the development of arterial hypertension. They increase blood pressure through the renin-angiotensinaldosterone system, causing a reduction in prostacyclin and nitric oxide production,and an increase in the quantity of angiotensin II receptors[92]. However, considering the usually short time of exposure to steroids in these patients, calcineurin inhibitors are the main agent responsible for the long-term development of arterial hypertension. The main concern about arterial hypertension is related to the direct damage on organs and its established association to increased risk for cardiovascular events[93]. Elevated blood pressure may lead to endothelial damage, atherosclerosis,kidney damage and left ventricle remodeling. Hypertensive control is essential to the improvement of long-term survival of both the graft and the recipient, related to the non-negligible risk of developing major cardiovascular events. The withdrawal of steroid therapy, the down-titration of calcineurin inhibitors (when adding mycophenolate mofetil or mTOR inhibitors) are possible strategies to reduce the increase in blood pressure values. Lifestyle modifications (i.e., low-sodium diet,cessation of smoking, avoidance of alcohol, and weight loss) should always be clearly explained to the patient. Nevertheless, when these measures are unsuccessful,medical therapy is mandatory. A blood pressure goal lower than 130/80 mmHg should be targeted to minimize cardiovascular risk[94]. Dihydropyridine calcium channel blockers are the preferred first-line agents in patients who do not exhibit proteinuria, in order to directly counteract the vasoconstriction associated with calcineurin inhibitors[95]. If proteinuria is present, liver transplant recipients benefit from angiotensin-converting enzyme (ACE) inhibitors or angiotensin II receptor blockers as a first line choice[95]. If a single-agent therapy is ineffective, a combination therapy should be evaluated, taking into account that the addition of beta-blockers is particularly indicated when a cardiac complication is well established[96]. Furthermore,angiotensin-converting enzyme inhibitors and angiotensin-2 blockers may magnify the collateral effects of calcineurin inhibitors such as hyperkalemia and metabolic acidosis, so it is advisable to use them during the long-term follow-up after liver transplantation, when the activation of the renin-angiotensin system becomes more evident. Diuretic therapy is typically avoided, due to the fact that volume contraction in the face of renal vasoconstriction may lead to further impairment in renal function[97].
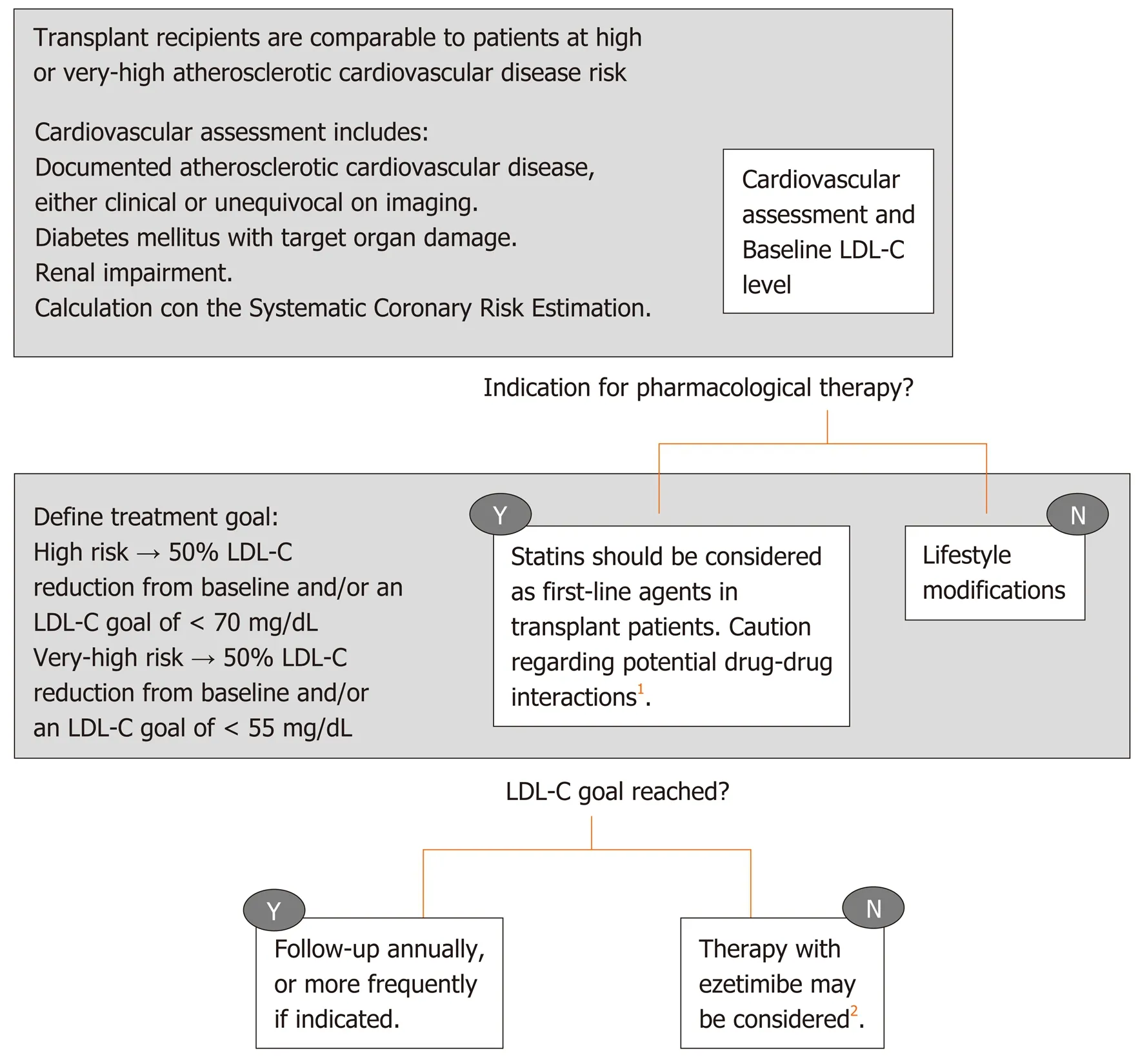
Figure 2 Proposal of a treatment algorithm for low-density lipoprotein cholesterol lowering strategy in liver transplant recipients.1Class of recommendation: IIa; level of evidence: B, according to 2019 ESC/EAS Guidelines for the management of dyslipidaemias[118]. 2Class of recommendation: IIb; level of evidence: C, according to 2019 ESC/EAS Guidelines for the management of dyslipidaemias[118]. LDL-C: Low-density lipoprotein cholesterol.
It is important to keep in mind that drug-drug interactions are frequent in this subgroup of patients. Certain antihypertensive medications, namely beta-blockers,can significantly impact levels of immunosuppressive medication, thus they should be monitored during the introduction of any new drug. Independently from the chosen approach for blood pressure control, the end goal is to find a balance between antihypertensive therapy and immunosuppressive therapy modulation.
RENAL IMPAIRMENT
One of the most frequent medium- and long-term medical complications after liver transplantation is the development of nephrotoxicity, which is estimated to be 8%,13.9% and 18.1% at 12, 36 and 60 mo post-transplant respectively[98]. Major causes of renal injury include the diagnosis of renal failure and/or hepatorenal syndrome prior to liver transplantation, critical intraoperative variables such as the need for vasopressors[99], donor-related variables such as donation after circulatory death, cold ischemia time, and graft steatosis[100,101]. All of these features are well established predictors of renal insufficiency after liver transplantation, particularly in the early post-surgical phase. However, in the majority of the cases, renal impairment is strongly associated with the direct side effects of immunosuppressive drugs in a dose dependent manner, such as calcineurin inhibitors. Nevertheless, it can also occur with combination regimens that aim to achieve low serum levels of tacrolimus. These findings have suggested the existence of different types of kidney damage based on different, partially reversible, mechanisms. The first type of damage is early and reversible, characterized by vasoconstriction of the kidney afferent arteriole, with a consensual reduction in glomerular filtration rate. A second and often irreversible damage is characterized by hyaline degeneration of renal arterioles, leading to glomerulosclerosis[102]. In this setting, the withdrawal of cyclosporine or tacrolimus is not effective for the recovery of kidney damage. Thus, early detection of renal impairment after liver transplantation is essential in order to implement different strategies to reduce calcineurin inhibitors levels. The introduction of immunosuppressive combination therapies such as adding mTOR inhibitors to low doses of calcineurin inhibitors represents a possibility to minimize the exposure to nephrotoxic agents, sparing kidney function, without an increase in graft rejection rates[103].Recently, new findings regarding the relationship between cardiovascular events after liver transplantation and renal impairment have been documented, underlying that even mild renal disease at the time of liver transplantation is a risk factor for posttransplant all-cause and cardiovascular mortality[104]. In a retrospective study on 202 transplant candidates pre-transplant renal impairment was found to be an independent predictor of post-transplant cardiac events (HR = 2.19, 95%CI: 1.25-3.85)and reduced cardiac event-free survival (HR = 2.27, 95%CI: 1.31-3.94)[105]. In addition,the velocity of the decline of glomerular filtrate rate after liver transplantation strongly correlated with the risk of adverse cardiovascular outcomes, highlighting the need to preserve early renal function in order to reduce these complications[104].
CARDIOVASCULAR DISEASES
Cardiovascular diseases affect long-term prognosis after solid organ transplantation.Nevertheless, this risk is substantially different for liver transplant recipients compared to other solid organ recipients. This is partially related to hemodynamic and metabolic changes associated with chronic liver disease[106]. The marked peripheral vasodilatation present in patients with decompensated end-stage cirrhosis makes difficult the detection of a latent myocardial dysfunction with cardiac abnormalities, such as an attenuation in the systolic and diastolic contractile responses leading to the so-called cirrhotic cardiomyopathy. These changes, combined with reduced serum cholesterol, can mask pre-liver transplant cardiovascular risk factors,increasing the challenge to identify those patients at highest risk for cardiovascular diseases[97]. The relevance is notable when analyzing mortality after liver transplantation: It is estimated that 12%-16% of deaths one year after liver transplantation in the USA is due to cardiovascular disease[7]. In Europe, the median estimated 10-year risk of fatal cardiovascular disease is 1% (range: 0%-9%) and 10% of the affected patients have a high risk for these events[107]. A detailed cardiovascular assessment during pre-liver transplant evaluation is thus mandatory to not only assess the perioperative risk but also to allow for an early intervention, if needed, to ensure a good long-term outcome. Despite no guidelines being available in the preliver transplant assessment for cardiovascular disease, every transplant center adopts different routines for cardiovascular assessment, in order to stratify the population risk.
Standard evaluation before liver transplantation normally includes a full history and clinical examination, peripheral artery oxygen saturation, 12 lead electrocardiogram and a complete transthoracic ultrasound with assessment of left ventricular, right ventricular and valvular function (with an estimation of systolic pulmonary artery pressure). Further investigations, such as stress echocardiography,cardiac computerized tomographic scan, cardiac magnetic resonance or angiography are solicited based on medical history, cardiology indication and findings from the initial screening tests[108]. It should be noted that second line tests such as dobutamine stress echocardiography have shown a poor predictive value for coronary artery disease screening (sensitivity: 28%), although with high specificity (specificity: 82%),compared with the gold standard coronary angiography[109]. When using a protocol angiography in the pre-transplant cardiac evaluation, 36% of patients showed coronary artery disease in a recently published study, with NASH and hepatitis C being independent risk factors[110]. However, another study showed that the incidence of major cardiovascular events and overall survival after liver transplantation are similar between patients with and without coronary evaluation[111]. In another study where a control group without cardiovascular risk factors was matched with a group with coronary artery disease showed that the severity or extent of coronary artery disease does not affect post liver transplantation survival, if appropriately revascularized. However, early postoperative cardiac events could be associated with lower survival rate, irrespectively of underlying coronary artery disease[112]. Hence, it is unclear how many pre-liver transplant asymptomatic cardiovascular abnormalities could influence long-term outcome after transplantation. On the other hand, it seems that cardiac complications are significantly more frequent in patients with a pre-liver transplant known heart disease compared with those without pre-existing cardiovascular disease[113]. Since liver transplantation is a significantly stressful procedure from a cardiovascular standpoint, cardiovascular mortality is of the utmost importance, particularly when cirrhotic cardiomyopathy is unknown or underestimated[114]. Following liver transplantation, peripheral vascular resistance and blood pressure rapidly increase; these changes may cause an overt cardiac failure leading to pulmonary edema in predisposed patients. Other possible cardiovascular complications include the development of post-operative atrial fibrillation, defined as a new-onset atrial fibrillation during liver transplantation surgery or within 30 d after this procedure in a patient without previous episodes. This phenomenon can drive to hemodynamic and thromboembolic events, significantly affecting the prognosis of the patients in the early post-liver transplantation[115]. Although the impact of these early events on the long-term cardiovascular prognosis has not been explored in detail, a recent retrospective study in over 1000 liver transplant patients found that the development of postoperative atrial fibrillation is an independent risk factor for postliver transplant mortality (OR = 2.0; 95%CI: 1.3-3.0;P< 0.01)[116]. Furthermore, as might be expected, NASH as an indication for liver transplantation had a significantly higher risk of a cardiovascular event 1 and 3 years after liver transplant. Even with a relatively low prevalence, major cardiac events are significantly associated with a lower 5-year survival rate, thus stressing the importance of identifying and stratifying high-risk patients prior to liver transplantation and offering targeted postoperative interventions. A study of Patelet al[117]has recently shown that despite that the presence and severity of pre-transplantation coronary artery disease may not affect post transplantation survival, the use of statins in the post-transplantation period might confer a survival benefit (HR = 0.25; 95%CI: 0.12-0.49;P< 0.001). This is independent of the use of aspirin, which did not show an effect on mortality.Nonetheless, the study highlighted that statin therapy is still very much underused,with only 46% of patients with proven coronary artery disease benefitting from this therapy. The medication was well tolerated (only 12% of recipients needed to stop the therapy due to side effects)[117], suggesting a promising role of statins in improving the outcomes after liver transplantation.
CONCLUSION
The proper identification of liver transplant recipients at risk of metabolic and cardiovascular morbidity and mortality after liver transplantation is still far from being satisfactory. Literature devoted to this topic is scarce and often of low quality,making it difficult to provide recommendations or to develop appropriate guidelines.Moreover, the efficacy and safety of the current treatment strategies for these metabolic complications needs to be validated in this specific population, as well as finding adequate surrogates which can be considered suitable targets to impact on the prognosis of liver transplant recipients.
However, as survival rate after liver transplantation increases, it seems clear that the management of metabolic complications and cardiovascular disease requires heightened attention. These comorbidities have a major impact on the morbidity,mortality and quality of life of liver transplant recipients in the late postoperative period. Early identification and proper management of these metabolic alterations,initially acting on lifestyle modifications, immunosuppression titration, and tailored medical therapy remain crucial to improve the outcome of liver transplant patients.
杂志排行

World Journal of Gastroenterology的其它文章
- New role for ceramide in hypoxia and insulin resistance
- Role of gut microbiota on intestinal barrier function in acute pancreatitis
- Prognostic significance of hepatic encephalopathy in patients with cirrhosis treated with current standards of care
- Optimal proximal resection margin distance for gastrectomy in advanced gastric cancer
- Computed tomography vs liver stiffness measurement and magnetic resonance imaging in evaluating esophageal varices in cirrhotic patients: A systematic review and meta-analysis
- Annexin A2 promotion of hepatocellular carcinoma tumorigenesis via the immune microenvironment