Endoscopic reduction of colocolonic intussusception due to metastatic malignant melanoma:A case report
2020-04-08
Kengo Kasuga,Taku Sakamoto,Hiroyuki Takamaru,Masau Sekiguchi,Masayoshi Yamada,Yutaka Saito,Endoscopy Division,National Cancer Center Hospital,Tokyo 104-0045,Japan
Masau Sekiguchi,Cancer Screening Center,National Cancer Center Hospital,Tokyo 104-0045,Japan
Naoya Yamazaki, Department of Dermatologic Oncology,National Cancer Center Hospital,Tokyo 104-0045,Japan
Taiki Hashimoto,Division of Diagnostic Pathology,National Cancer Center Hospital,Tokyo 104-0045,Japan
Toshio Uraoka,Department of Gastroenterology and Hepatology,Gunma University Graduate School of Medicine,Maebashi 371-8511,Gunma,Japan
Abstract BACKGROUND Intussusception rarely causes intestinal obstruction in adults. Metastatic malignant melanoma is the main cause of intussusception of the small intestine among adults. However,malignant melanoma rarely causes intussusception of the colorectum. Moreover,emergent surgery is usually performed for such cases.Here,we report a case of a patient with colocolonic intussusception caused by a malignant melanoma,for which endoscopic reduction and elective surgery were performed.CASE SUMMARY The patient was a 64-year-old woman who underwent multiple surgeries and received chemotherapy and immunotherapy for a malignant melanoma. During immunotherapy,she had abdominal pain,diarrhea,and bloody stool. Physical examination and laboratory studies did not reveal any findings that warranted emergent surgery. Computed tomography revealed intussusception in the descending colon without intestinal necrosis and perforation. Intussusception was reduced endoscopically,and elective surgery was performed.CONCLUSION This report suggests that endoscopic reduction and elective surgery constitute a treatment option for colocolonic intussusception of metastatic malignant melanomas.
Key Words: Metastatic malignant melanoma; Intussusception; Colon; Nonsurgical management; Endoscopic reduction; Case report
INTRODUCTION
Intussusception rarely causes intestinal obstruction among adults. Metastatic malignant melanoma is the main cause of intussusception in the small intestine of adults[1-3]. Symptomatic metastatic melanoma of the colon is very rare,and there are only a few reports on intussusception due to metastatic malignant melanoma of the colorectum[4-6]. In intussusception of the colon due to metastatic melanoma,emergent surgery is commonly performed. Here,we report a case of a patient with colocolonic intussusception caused by a malignant melanoma,for which endoscopic reduction and elective surgery were performed.
CASE PRESENTATION
Chief complaints
A 60-year-old woman had abdominal pain,diarrhea,and bloody stool in July 2019.
History of present illness
The patient had abdominal pain intermittently 11 d before admission. She also had diarrhea and bloody stool,due to which she sought hospital admission.
History of past illness
In 2004,a melanoma in the patient’s left fifth toe was resected,and inguinal lymph node dissection was performed. The patient underwent five courses of adjuvant chemotherapy with dacarbazine,nimustine,vincristine,and interferon-β.
In June 2015,she developed intussusception and was diagnosed with melanoma metastasis following laparoscopic partial resection of the small intestine. In September 2016,she underwent partial resection of the small intestine and mesenteric lymph node removal for mesenteric lymph node metastasis. In September 2016,she was referred to our hospital after undergoing partial resection of the small intestine and mesenteric lymph node removal for mesenteric lymph node metastasis. Left supraclavicular lymph node enlargement was noted in a follow-up evaluation; thus,in July 2017,treatment with talimogene laherparepvec was initiated,but the lymph node enlargement persisted. In January 2018,pembrolizumab therapy was started. The patient’s lymph nodes gradually reduced in size.
Personal and family history
The patient had a free previous medical history.
Physical examination
Her vital signs were normal. Physical examination revealed diffuse abdominal tenderness without rebound tenderness.
Laboratory examinations
The results of the laboratory tests showed normal values,which were as follows:Hemoglobin,12.4 g/dL; white blood cell count,5.4 × 103/mm3; and C-reactive protein,0.12 mg/dL.
Imaging examinations
Computed tomography,which was performed on the day of admission,revealed antegrade intussusception in the descending colon without intestinal necrosis and perforation (Figure 1). Therefore,colonoscopy was performed for diagnostic purposes.The patient was examined using carbon dioxide and water insufflations. Colonoscopy showed a greyish-white protruded lesion in the descending colon (Figure 2A); the mucosa surrounding the tumor was reddish and edematous,and the tumor in the descending colon fell to the anal side,causing intussusception. Intussusception was reduced naturally during the examination (Figure 2B). After the examination,the abdominal symptoms subsided. Biopsy of the protruded lesions revealed that the tumor was a metastatic melanoma.
TREATMENT
The intussusception did not recur after eating,and elective laparoscopic surgery was performed 14 d after the reduction. Surgical findings showed a tumor with a diameter of approximately 30 mm located in the splenic flexure of the descending colon; thus,left hemicolectomy was performed.
FINAL DIAGNOSIS
Histopathological examination revealed that the tumor cells had infiltrated into the colonic muscularis propria. The patient was diagnosed with metastatic melanoma with no metastatic tumor in 7 lymph nodes (Figure 3).
OUTCOME AND FOLLOW-UP
The patient’s postoperative course was good,and she was discharged on postoperative day 7. The patient is scheduled to continue to undergo immunotherapy.
DISCUSSION
To the best of our knowledge,this is the first report of endoscopic reduction and elective surgery for colocolonic intussusception caused by a malignant melanoma.Endoscopic reduction relieved the bowel obstruction associated with the disease. To treat intussusception in children,it is common to perform air or saline enema under ultrasound or fluoroscopic guidance[7]; however,if reduction cannot be achieved,surgery is generally performed. In adults,surgery is the standard treatment. In small bowel intussusception,preoperative reduction is often performed. However,colocolonic or ileocolic intussusception is often caused by a primary colorectal cancer;thus,preoperative and intraoperative reduction is not recommended because of the risk of hematogenous metastasis associated with the reduction procedure[8]. The previously recommended treatment for intussusception among adults was surgery,and preoperative reduction with barium or air is not recommended[8,9].

Figure 1 Computed tomography scan showing suspicious presence of a target or doughnut sign in the descending colon.
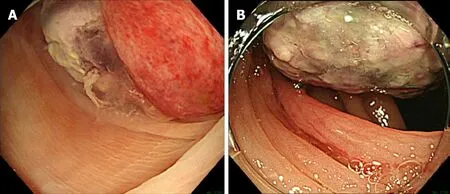
Figure 2 Colonoscopy examinations. A:Intussusception caused by a protruded lesion in the descending colon; B:Intussusception reduced naturally during colonoscopy.
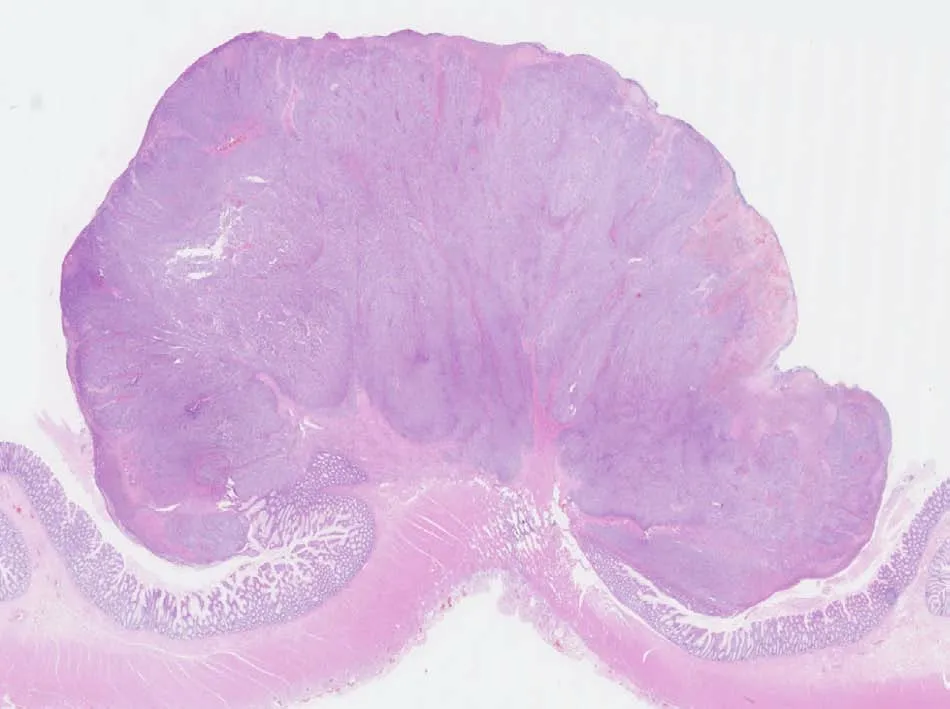
Figure 3 Histopathologically,hematoxylin and eosin staining shows a tumor invading the muscularis propria (magnification,× 4).
Recently,asymptomatic intussusception could be easily diagnosed owing to the advancement in computed tomography; sometimes,for these cases,conservative treatment is performed without surgery[10,11]. Thus,emergent surgery is not necessary for all cases of colocolonic intussusception. Furthermore,reduction procedures have been performed in some adult cases of colocolonic or ileocolic intussusception[3,12]. In addition,preoperative colonoscopy is performed to confirm the presence of colorectal tumors and make pathological diagnoses. In this case,the patient had no clinical findings that required emergent surgery such as necrosis or perforation. Thus,we carefully performed colonoscopy using carbon dioxide and water insufflations. We could establish the pathological diagnosis safely without any adverse events.Furthermore,endoscopic reduction was performed coincidentally on the patient,thereby preventing the occurrence of tumor seeding due to perforations. In addition,we were able to evaluate the patient’s general condition preoperatively. Thus,the patient underwent surgery more safely,allowing for a limited resection.
In this case,we performed endoscopic reduction of intussusception of the colon due to a metastatic malignant melanoma. Thus,in some cases,the reduction of intussusception due to other metastatic tumors may be possible.Emergent surgery is indicated in patients with intestinal necrosis or perforation or if a primary colorectal cancer is suspected. However,endoscopic reduction may be an option if the patient’s medical history suggests metastasis of another organ cancer and the patient has no intestinal necrosis or perforation.
CONCLUSION
Endoscopic reduction and elective surgery constitute a treatment option for colocolonic intussusception of metastatic malignant melanomas. If colocolonic intussusception is confirmed,based on the clinical and imaging findings,without any intestinal necrosis and perforation and there is a medical history of a malignant melanoma,preoperative endoscopy for diagnosis and reduction should be considered.
杂志排行
World Journal of Clinical Cases的其它文章
- Is Dynesys dynamic stabilization system superior to posterior lumbar fusion in the treatment of lumbar degenerative diseases?
- Is positivity for hepatitis C virus antibody predictive of lower risk of death in COVID-19 patients with cirrhosis?
- Usefulness of ultrasonography to assess the response to steroidal therapy for the rare case of type 2b immunoglobulin G4-related sclerosing cholangitis without pancreatitis:A case report
- Large leiomyoma of lower esophagus diagnosed by endoscopic ultrasonography-fine needle aspiration:A case report
- Robot-assisted laparoscopic pyeloureterostomy for ureteropelvic junction rupture sustained in a traffic accident:A case report
- Hemorrhagic fever with renal syndrome complicated with aortic dissection:A case report