Chest, pericardium, abdomen, and thigh penetrating injury by a steel rebar: A case report
2020-04-08XianWeiYangWenTaoWang
Xian-Wei Yang, Wen-Tao Wang
Xian-Wei Yang, Wen-Tao Wang, Department of Liver Surgery & Liver Transplantation Center,West China Hospital, Sichuan University, Chengdu 610000, Sichuan Province, China
Abstract BACKGROUND Combined penetrating trauma involving the chest, pericardium, abdomen, and thigh is rare and lethal. It is difficult to quickly rescue patients with penetrating injuries from long steel bars.CASE SUMMARY A previously healthy 56-year-old male worker presented with a length of rebar that penetrated the chest-abdomen-pelvic cavity and was palpable on the anterior side of the neck and thigh. On radiological imaging, the left chest wall-left chest cavity-mediastinum-abdominal cavity-right groin area-right thigh demonstrated a strip-like density shadow, about 1.5 cm thick, with the heart, stomach wall, and part of the intestine involved. There was a left-sided pleural effusion, left lung compression of about 50%-60%, and a small amount of left pleural effusion/blood accumulation; possible perforation of hollow organs; and double multiple ribs fractures on the side. An emergency green channel was opened to provide a rescue process for smooth and timely diagnostic and treatment to save the patient's life. The patient was followed at 4 mo after discharge and showed good recovery.CONCLUSION For pre-hospital emergency treatment in locations that are not fully prepared for surgery, we do not recommend cutting the steel bars outside the body. We advocate pulling out foreign bodies intact to reduce secondary injuries.
Key Words: Penetrating trauma; Rebar; Diaphragm injury; Thoracoabdominal; Pre-hospital emergency; Case report
INTRODUCTION
Rebar penetration injury is extremely rare but it is life-threatening for construction workers, especially chest, abdomen, pelvic cavity, and limb injuries. The length,diameter, and path into the human body are the main factors that affect pre-hospital emergency and surgical methods. Very few studies[1-4]reported the penetration damage of steel bars, which lack systematic guidance. Therefore, we describe in detail a case of penetrating injury with regard to pre-hospital emergency, imaging, surgery,and follow-up.
CASE PRESENTATION
Chief complaints
A 56-year-old male worker went to the hospital and suffered a penetrating injury to his chest and abdomen for 1 h due to a fall from about 3 m. In the emergency department, he presented with nervousness, fear, mild chest pain and abdominal pain.
History of present illness
This patient sustained penetrating trauma of the left chest, abdomen, and right thigh with a piece of rebar that was 2 m in length and 15 mm in diameter during an accidental fall that had occurred 1 h earlier. His workmates immediately called ambulance and he was transported to our center. We opened a priority channel for him to surgery preparation.
History of past illness
This patient was usually healthy, had regular physical examinations, and had no family history.
Physical examination
The patient was conscious and his answers were smooth and accurate. His vital signs were as follows: Body temperature, 37.3°C; pulse, 108/min; respiration rate, 26/min;blood pressure, 119/72 mmHg; and oxygen saturation, 97%. He had no angina,shortness of breath, bloating, muscle tension, or rebound pain. The patient had no other evidence of trauma.
Laboratory examinations
Main laboratory results were: Hemoglobin 133 g/L, white blood cell count 10.3 × 109/L, neutrophil percentage (NEUT%) 87.0%, alanine aminotransferase (ALT) 16 IU/L,sodium (NA) 139.9 mmol/L, potassium (K) 4.08 mmol/L, total bilirubin (TBIL) 10.4µmol/L, myoglobin (Myo) 150.50 ng/mL, and prothrombin time (PT) 10.7 s.
Imaging examinations
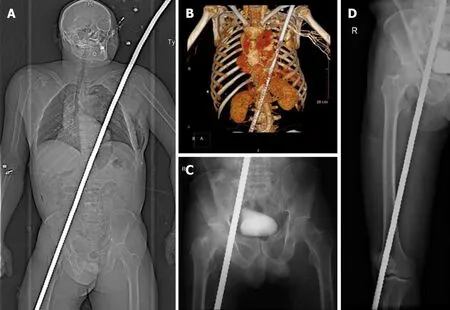
Figure 1 X-ray images. A: X-ray image revealing a high-density shadow; B-D: Images revealing that the rebar passed through the pericardium, reaching the pelvis and extending to the thigh.
Computed tomography and X-rays of the body revealed a rebar extending through the left chest next to the heart and abdominal cavity. A significant portion of the rebar protruded into the abdomen (Figure 1A). There was evidence of rib fractures,pneumothorax, pericardium and diaphragm rupture, and stomach and intestinal wall injuries, not excluding left liver lobe rupture and gastrointestinal perforation. The great vessels of the chest were spared, and the left lung and pericardium were lacerated and contused (Figure 1B-D).
MULTIDISCIPLINARY EXPERT CONSULTATION
After multidisciplinary discussions including thoracic surgery, cardiac surgery, liver surgery, gastrointestinal surgery, urology, vascular surgery, plastic surgery,orthopedics, psychotherapy, and anesthesiology, it was firmly agreed that the patient was in critical condition and should undergo surgery as soon as possible. Firefighters waited outside the operating room door with professional equipment prepared to cut the rebar during the operation. However, because the nature and severity of the impaling injury were not yet known, the decision was made to take directly the patient to the operating room.
FINAL DIAGNOSIS
This patient was finally diagnosed with penetrating injuries involving multiple organs,mainly including the chest, pericardium, stomach, intestine, and thighs. After preoperative evaluation, thoracotomy and exploratory laparotomy were planned and performed on April 25, 2020.
TREATMENT
More than ten surgeons from different departments performed over 3 h of surgery to remove the rebar from the body and successfully repaired the injuries. The patient received tetanus prophylaxis and intravenous cefoxitin and was then transported to the operating room, carefully placed in the supine position without moving the rebar.A left thoracoabdominal incision was made, joining the entry and exit wounds(Figure 2A). The surrounding organ tissue was incised or moved around the edge of the rebar. The rebar (wrapped with gauze) was slowly lifted from the thigh to the left chest under vision directly from the surgical incision and was removed completely.Repair of pulmonary parenchymal damage, diaphragm, stomach wall, mesentery, and subcutaneous holes in the thighs was then performed (Figure 2B and C). Total blood loss was approximately 200 mL.
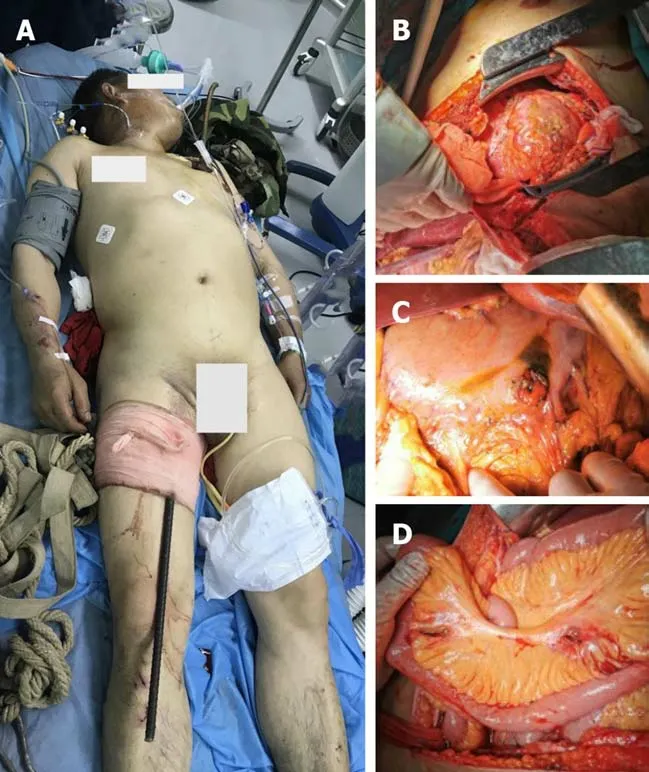
Figure 2 Treatment process. A: The length of the rebar in the patient’s body; B-D: After removing the rebar from the body, it was found that rupture of the pericardium, perforation of the stomach wall, and penetrating trauma of the mesentery were the main manifestations.
OUTCOME AND FOLLOW-UP
The patient received psychological care and did not suffer postoperative complications. He recovered uneventfully and was discharged 13 d later on oral antibiotics. During the follow-up period of nearly 4 mo, the patient showed no fever or infection, and returned to normal work and family life.
DISCUSSION
Combined thoracic and abdominal injuries result in sequential damage, including lung lobes, heart, pericardium, diaphragm, and abdominal organs. Despite the low incidence, the mortality rate is high[5,6]. This case highlights the importance of a multidisciplinary team approach and maintenance of foreign body integrity for the survival of severe rebar injury patients. We do not recommend cutting steel bars before surgery to avoid secondary damage. Thoracic and abdominal penetrating injuries should be treated simultaneously to ensure that the rebar has a wide range of movement in the chest cavity, pericardium, mesentery, and stomach wall. Similar to the case reported by Zhanget al[4], emergency treatment measures for penetrating injuries are particularly important. Although these two lucky patients eventually survived, our experiences in managing steel injuries are worth recommending and emulating. This case focused on the indications of surgery and the description of the intraoperative situation. The successful rescue of this patient depended on the quick judgment of the way that the rebar was taken out. This was also the benefit of simultaneous thoracotomy and laparotomy. This study did not focus on the details of nursing, trauma assessment, emergency triage process, and role tasks, which should be the basic principle of emergency. Last but most important, patients should be followed to avoid losing monitoring of diaphragmatic hernias[7,8], infections, intestinal obstruction, psychological injury, and posttraumatic stress disorder.
CONCLUSION
Emergency doctors should establish a holistic concept in dealing with penetrating injuries. Pulling out rebar under direct surgery can reduce secondary injuries. To help workers recover smoothly, antibiotics and psychotherapy are also particularly important.
ACKNOWLEDGEMENTS
We are grateful to the departments of emergency medicine, cardiothoracic surgery,urology surgery, gastrointestinal surgery, vascular surgery, orthopedics, and anesthesiology of our hospital, for their substantial help.
杂志排行

World Journal of Clinical Cases的其它文章
- Effective administration of cranial drilling therapy in the treatment of fourth degree temporal, facial and upper limb burns at high altitude:A case report
- Rare imaging findings of hypersensitivity pneumonitis: A case report
- Successful management of a tooth with endodontic-periodontal lesion: A case report
- Primary chondrosarcoma of the liver: A case report
- Choriocarcinoma with lumbar muscle metastases: A case report
- Monocular posterior scleritis presenting as acute conjunctivitis: A case report