Catastrophic vertebral artery and subclavian artery pseudoaneurysms caused by a fishbone: A case report
2020-04-08WeiHuangGuangQiangZhangJianJunWuBinLiShuGaoHanMingChaoKaiJin
Wei Huang, Guang-Qiang Zhang, Jian-Jun Wu, Bin Li, Shu-Gao Han, Ming Chao, Kai Jin
Wei Huang, Guang-Qiang Zhang, Jian-Jun Wu, Bin Li, Shu-Gao Han, Ming Chao, Kai Jin,Department of Radiology, The Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou 310009, Zhejiang Province, China
Abstract BACKGROUND Fishbone is the most common esophageal foreign body and tends to migrate after piercing the esophagus to nearby structures. Vascular injury around the esophagus is a serious complication and has a high mortality rate, especially in the case of multiple vascular injuries.CASE SUMMARY We report an extremely rare case of successive vertebral artery and subclavian artery pseudoaneurysms caused by swallowing a fishbone in a previously healthy 29-year-old female. She was transferred to the emergency department of our hospital because of hemorrhagic shock due to a vertebral artery pseudoaneurysm.We successfully managed the vertebral artery pseudoaneurysm with endovascular stent implantation and the patient’s vital signs as well as hemodynamics once became stable. However, the patient died of the second subclavian artery pseudoaneurysm occurring within a short time, which was thought be related to the obvious displacement of the fishbone in the mediastinum.CONCLUSION Surgery and endovascular stent implantation may be the best choice for treating such complications. Early removal of the fishbone is of great significance in improving the survival of such patients.
Key Words: Esophageal fishbone; Vertebral artery; Subclavian artery; Pseudoaneurysm;Endovascular stent implantation; Case report
INTRODUCTION
Fishbones are the most common esophageal foreign bodies. Most swallowed fishbones can be naturally excreted through the digestive tract or removed endoscopically without further treatment[1]. In rare cases, swallowed fishbones can penetrate the wall of the esophagus and cause catastrophic damage to the blood vessels around the esophagus. This serious complication is associated with a very high mortality rate. We here report an extremely rare case of successive vertebral and subclavian arterypseudoaneurysms caused by a fishbone within a short time. We also review the relevant literature to improve the understanding of such serious complications of vascular injuries around esophagus caused by fishbones.
CASE PRESENTATION
Chief complaints
A previously healthy 29-year-old female was transferred to the emergency department of the Second Affiliated Hospital of Zhejiang University School of Medicine because of left hemothorax with hemodynamic instability.
History of present illness
She had suffered from increased neck pain with shortness of breath and severe vomiting without hematemesis after eating fish two days before. The examination in a local hospital indicated a massive left pleural effusion on chest radiograph; however,no fishbone was found under laryngoscopy. Due to her rapidly decreasing blood pressure even after massive liquid infusion, the patient was quickly transferred to our hospital for further treatment.
History of past illness
The patient had a free previous medical history.
Physical examination
At the time of admission, the patient was in a light coma. Vital signs showed a heart rate of 129 beats/min and blood pressure of 69/35 mmHg.
Laboratory examinations
Blood tests revealed that her hemoglobin was 46 g/L.
Imaging examinations
The enhanced chest computed tomography (CT) showed a pseudoaneurysm in the initial segment of the left vertebral artery and massive effusion in the mediastinum and the left thoracic cavity (Figure 1A).

Figure 1 Coronal reconstruction of the contrast-enhanced chest CT (A) and digital subtraction angiography of the vertebral artery and endovascular stent implantation (B and C). A: Pseudoaneurysm formation in the initial segment of the left vertebral artery (arrow) and a large amount of effusion in the left thoracic cavity; B: Contrast medium overflow at the start of the left vertebral artery (arrow), suggesting the formation of a pseudoaneurysm; C: The signs of vertebral arterial contrast medium spillage disappeared after stent implantation.
FINAL DIAGNOSIS
She was promptly diagnosed with hemorrhagic shock due to vertebral artery pseudoaneurysms caused by a fishbone.
TREATMENT
The patient suffered from sudden cardiac arrest half an hour after admission. After successful cardiopulmonary resuscitation, a thoracotomy was performed, during which a large amount of uncoagulated blood was found in the left thorax. The pleura on the top wall of the left lung was ruptured, and pulsatile bleeding was seen from the breach. After gauze packing, digital subtraction angiography (DSA) of the carotid artery was performed and showed an overflow of contrast medium in the initial segment of the left vertebral artery (Figure 1B). A pseudoaneurysm was discovered,and two stent grafts (5 mm x 50 mm, 5 mm x 25 mm, W.L. Gore & Associates, Inc.)were implanted. After that, no contrast medium spillage was seen (Figure 1C).Thoracoscopy was performed on the next day to remove the gauze. No active bleeding was found at the rupture site of the original pleura.
The patient underwent symptomatic supportive therapies such as infusion, blood transfusion, and anti-infection in the Intensive Care Unit.
OUTCOME AND FOLLOW-UP
She maintained clear consciousness while her vital signs and hemodynamics became stable. Tracheal extubation was performed on the 6th d after admission. However, on the 9th d after admission, the patient suddenly developed hemorrhagic shock again.The enhanced chest CT revealed a new pseudoaneurysm at the beginning of the left subclavian artery (Figure 2A). An emergency thoracotomy was performed and showed active bleeding at the top of the left pleura again. Gauze was used to stop bleeding, and DSA was performed immediately. Pseudoaneurysm on the left subclavian artery (Figure 2B) was confirmed, and two stent grafts (8 mm × 25 mm, 8 mm × 50 mm, W.L. Gore& Associates, Inc.) were successfully implanted in the left subclavian artery (Figure 2C). The patient's hemoglobin did not decline further, but her condition progressively worsened into multiple organ failure. She died on the 11th d after admission.
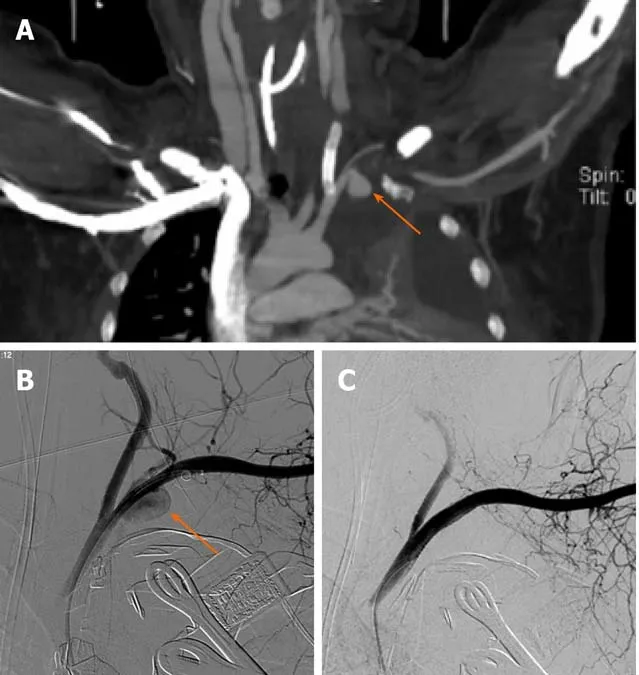
Figure 2 Coronal reconstruction of the contrast-enhanced chest CT (A) and digital subtraction angiography of the left subclavian artery and stent implantation. A: Pseudoaneurysm formation at the start of the left subclavian artery (arrow) and endovascular stent implantation in the left vertebral artery. B: Contrast medium overflow at the start of the left subclavian artery, suggesting the formation of a pseudoaneurysm (arrow); C: After the stent graft was implanted, the contrast medium spillage disappeared.
DISCUSSION
Serious complications occur in less than 5% of patients after swallowing a fishbone[2]and include esophageal perforation, mediastinal infection, neck abscess, lung injury,and vascular damage around the esophagus[3], among which vascular injury is the most dangerous. Although chest CT, endoscopy, and thoracotomy did not find a fishbone in our case, we considered that both pseudoaneurysms were caused by the fishbone piercing the artery wall according to the history and clinical manifestations of swallowing a fishbone.
There are two different types of vascular injury around the esophagus caused by a fishbone. One is the formation of a fistula between the esophagus and arteries such as the thoracic aorta, common carotid artery, subclavian artery, and lingual artery[3-6].Aortic-esophageal fistula (AEF) is relatively common and associated with a high mortality rate. Another type arises when the fishbone enters the mediastinum completely by penetrating the wall of the esophagus and then pierces the adjacent blood vessels to form a pseudoaneurysm, but no fistula is formed between the esophagus and blood vessels. Our case is an example of the second type. The patient felt discomfort after swallowing the fishbone, but the feeling was relieved by a following cough. The fishbone probably penetrated the esophagus wall into the mediastinum during the cough. No hematemesis occurred after the pseudoaneurysm formation, indicating that no fistula formed between the damaged artery and the esophagus. The blood accumulated in the mediastinum and flowed into the left thoracic cavity through the damaged parietal pleura. This situation is rarer than in the first type. A fishbone that penetrated the esophagus wall into the mediastinum can move and pierce the neck and chest blood vessels, such as the common carotid artery,subclavian artery, and zygomatic vein[7,8]. However, cases of vertebral artery injuries caused by a fishbone were quite rare[9]and the cases of vertebral artery pseudoaneurysm have never been reported before. In addition, all of the cases reported previously were single vascular injuries, and there were no reports of multiple arteries damaged in a short term, as in our case. This was the main cause of death for our patient, which makes our report unique.
Surgery and endovascular stent implantation are the main therapies for swallowed fishbones complicated with artery pseudoaneurysms around the esophagus. Surgery is the traditional and most recognized treatment, but it is traumatic and cannot control the bleeding quickly. Generally, cases of pseudoaneurysms accidentally caused by fishbones are highly precarious and complex. The patients who have been previously treated with surgery alone always died. It was not until 1980 that the first case of AEF was successfully treated[10]. Endovascular stent implantation is an emerging method. It is minimally invasive and can stop bleeding quickly, which makes up for the shortcomings of traditional surgery. Endovascular stent can not only save patients'lives in a timely manner but also allow for subsequent surgery[5]. However, this approach could not remove the fishbone and solve the problems of infection caused by the esophageal perforation. Therefore, the combined use of these two treatments can effectively improve the survival of such patients. In this case, the patient was in a stable condition after endovascular therapy for the first pseudoaneurysm. However,the second pseudoaneurysm led to another episode of severe hemorrhagic shock within a short period of time, which is why the patient died even after two successful hemostasis operations. We speculated that the occurrence of two blood vessel injuries in a short time may be related to the obvious displacement of the fishbone in the mediastinum. Therefore, it is of great significance to find and remove the fishbone as soon as possible. In addition, some scholars believe that mediastinal infection secondary to esophageal perforation may also be the cause of arterial injury[11], and anti-infection treatment is also important.
CONCLUSION
Vascular injury around the esophagus is a serious complication of swallowing fishbones and associated with a high mortality rate, especially in the case of multiple vascular injuries. The combined use of surgery and endovascular stent implantation is the best choice to treat such complications. Early removal of the fishbone can avoid multiple blood vessel injuries and can significantly improve the survival of such patients.
ACKNOWLEDGEMENTS
The authors thank Cheng-Yan Zhang of the Institute of Immunology, Zhejiang University for her help in this study.
杂志排行

World Journal of Clinical Cases的其它文章
- Effective administration of cranial drilling therapy in the treatment of fourth degree temporal, facial and upper limb burns at high altitude:A case report
- Rare imaging findings of hypersensitivity pneumonitis: A case report
- Successful management of a tooth with endodontic-periodontal lesion: A case report
- Primary chondrosarcoma of the liver: A case report
- Choriocarcinoma with lumbar muscle metastases: A case report
- Monocular posterior scleritis presenting as acute conjunctivitis: A case report