Benign symmetric lipomatosis (Madelung’s disease) with concomitant incarcerated femoral hernia: A case report
2020-04-07BoLiZhengXingRangJiaCongWengGuoZuoXiongXianPengDai
Bo Li, Zheng-Xing Rang, Jia-Cong Weng, Guo-Zuo Xiong, Xian-Peng Dai
Bo Li, Zheng-Xing Rang, Jia-Cong Weng, Guo-Zuo Xiong, Xian-Peng Dai, Department of Vascular and Hernia Surgery, The Second Affiliated Hospital of Nanhua University, Hengyang 421001,Hunan Province, China
Abstract BACKGROUND Benign symmetric lipomatosis (BSL) was first described by Brodie in 1846 and defined as Madelung’s disease by Madelung in 1888. At present, about 400 cases have been reported worldwide. Across these cases, surgical resection remains the recommended treatment. Here we report a case of neck BSL with concomitant thick fatty deposit in the inguinal region, which concealed the signs of a right incarcerated femoral hernia.CASE SUMMARY A 69-year-old male patient was admitted to our hospital with “abdominal pain,abdominal distension, nausea-vomiting and difficult defecation for half a month”.Moreover, he had a mass in the right inguinal region for more than 10 years. An egg-sized neck mass also developed 15 years ago and had developed into a full neck enlargement 1 year later. In addition, the patient had a history of heavy alcohol consumption for more than 40 years. With the aid of computerized tomography scan, the patient was diagnosed with BSL and a low intestinal mechanical obstruction caused by a right inguinal incarcerated hernia. Under general anesthesia, right inguinal incarcerated femoral hernia loosening and tension-free hernia repair was performed. However, this patient did not receive BSL resection. After a 1-year follow-up, no recurrence of the right inguinal femoral hernia was found. Moreover, no increase in fat accumulation was found in the neck or other areas.CONCLUSION Secretive intraperitoneal fat increase may be difficult to detect, but a conservative treatment strategy can be adopted as long as it does not significantly affect the quality-of-life.
Key Words: Benign symmetric lipomatosis; Madelung’s disease; Neck; Inguinal region;Inguinal incarcerated hernia; Case report
INTRODUCTION
Benign symmetric lipomatosis (BSL), also called Madelung’s disease, multiple symmetric lipomatosis or Launosi-Bensaude syndrome, manifests with abnormal fat distribution[1]. BSL was first described by Brodie in 1846 and defined by Madelung in 1888[2]. Alcohol withdrawal is the most effective prevention and treatment, although the pathogenesis of BSL is still unclear[3]. The disease is more common in middle-aged to elderly men and often develops in white people in the Mediterranean region or eastern Europe[4]. Nevertheless, the incidence rate of BSL is low, and at present about 400 cases have been reported worldwide with the number of cases reported in China being similar to that of other countries.
The diagnosis of BSL is primarily based on clinical characteristics and imaging examinations, particularly that of magnetic resonance imaging, to determine fat deposition. Surgical resection remains the recommended treatment. However, other treatment options are also available. The most frequently affected body part for BSL is the neck and can result in serious neck deformity, social anxiety and breathing difficulties. Here, we report a rare case of neck BSL (conservative strategy adopted)with a concomitant thick fatty deposit in the inguinal region (surgical treatment performed), which concealed the signs of an incarcerated femoral hernia.
CASE PRESENTATION
Chief complaints
A 69-year-old male patient was admitted to The Second Affiliated Hospital of Nanhua University with abdominal pain, abdominal distension, nausea-vomiting and difficult defecation.
History of present illness
The patient admitted to The Second Affiliated Hospital of Nanhua University presented with abdominal pain, abdominal distension, nausea-vomiting and difficult defecation for half a month.
History of past illness
The patient had a mass in the right inguinal region for more than 10 years. Moreover,an egg-sized neck mass occurred 15 years ago and gradually developed into full-neck enlargement within the following year. In addition, the patient had a history of heavy alcohol consumption for more than 40 years.
Physical examination
During the physical examination, a mild abdominal distension and right lower abdominal tenderness were found. Moreover, a mass was palpated in the right inguinal region, and obvious symmetrical fat accumulated in the neck and shoulder on both sides of the body.
Laboratory examinations
During the laboratory examination, no special laboratory signs were found.
Imaging examinations
Computerized tomography (CT) showed intestinal obstruction (Figure 1A) and a mass in the right inguinal region (Figure 1B). Moreover, there was a full-neck enlargement(which gradually developed from an egg-sized neck mass that occurred 15 years ago)(Figure 2A and 2B). The CT scan of the neck showed symmetrical fat accumulation in the neck and shoulder on both sides of the body (Figure 3A and 3B).
FINAL DIAGNOSIS
BSL with concomitant right inguinal incarcerated hernia causing low intestinal mechanical obstruction.
TREATMENT
Under general anesthesia, an emergency right inguinal incarcerated femoral hernia loosening and tension-free hernia repair was performed on the night of hospital admission. The hernia content proved to be that of the small intestine with congestion and edema, and no intestinal necrosis was observed. Medical repair patches (UHSL1 patches, Johnson & Johnson) were intraoperatively implanted with a connecting column connecting the upper and lower patches to reduce their movement. One patch was a rectangular piece of size 12 cm × 6 cm covering the posterior wall of the inguinal canal the other was a circular piece of size 10 cm × 6 cm covering the pectineus foramen. However, he did not receive surgery for BSL. As a standard of clinical practice, the patient was admitted to the intensive care unit for postoperative monitoring and care. He began anal exhaust when transferred to the general ward 1 d after surgery and defecated 2 d later. No complications, such as incision infection and liquefaction, occurred during hospitalization.
OUTCOME AND FOLLOW-UP
After a 1-year follow-up, no recurrence of the right inguinal femoral hernia (i.e.no intestinal protrusion in the right inguinal area and no obvious gas accumulation in the intestinal canal) was found on the CT scan (Figure 4A and 4B). Although the patient did not receive surgery or any other BSL treatment and was still mildly alcoholic, no increase in fat accumulation was observed in the neck or other areas during the followup period. Therefore, the secretive increase of intraperitoneal fat may be difficult to detect until the appearance of abdominal symptoms. A conservative strategy can be selectively adopted as long as the quality-of-life of the BSL patients is not affected.
DISCUSSION
BSL is mainly presented as the accumulation of a large amount of nonenveloped fatty tissue in the neck and abdomen, but most deposits are benign lesions[1]. BSL can also manifest as symmetrical fat deposition in the tongue[5], scrotum and other rare body parts[6]. Clinically, BSL is divided into three types[7]. Type I mainly develops in males where adipose tissue lesions are mainly concentrated in the neck, upper back,shoulder and upper arm,etc. Type II has no gender tendency, and the incidence rate in males and females is similar. The main lesion sites are the upper back, deltoid muscle area, upper arm, buttocks and upper thighs, and some patients have fat accumulation in the upper abdomen. Type III is a congenital accumulation of fat around the trunk.We classify the current case as Type I BSL based on the clinical manifestation of a large amount of symmetrical and painless fat tissue that accumulated in parts of the jaw,neck, occipital, shoulder, back, sternum and supraclavicular fossa. The skin color of the lesion was normal with a painless and unclear boundary, poor movement and a nodular soft mass. However, physical symptoms may occur if the trachea and local nerves are compressed by a large amount of fat accumulation.
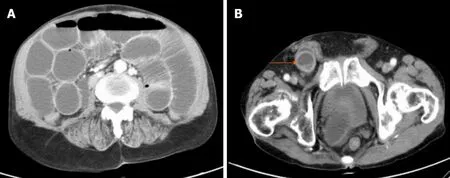
Figure 1 Computerized tomography images of the patient’s abdomen. A: Intestinal obstruction was observed; B: A mass was observed in the right inguinal region (arrow).

Figure 2 Photos of the patient showing a full-neck enlargement gradually developed from an egg-sized neck mass occurring 15 years ago. A: Posterior view; B: Side view. Arrows show the neck enlargement.
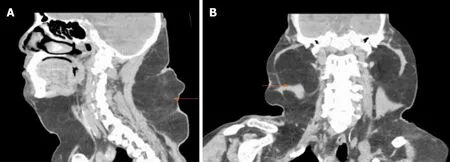
Figure 3 Computerized tomography images showing symmetrical fat accumulation in the neck and shoulder on both sides of the body. A:An image showing fat accumulation on the front and posterior sides of the patient’s neck; B: An image showing fat accumulation on the left and right sides of the patient’s neck. Arrows show fat accumulation.
In the present case, CT images indicated that the patient also had thick fat deposits in the inguinal region, and thus the signs of commitment incarcerated hernia were easily missed. Therefore, for such cases, the diagnosis should be confirmed based on the patient’s previous medical history, physical examination and CT imaging. What we want to emphasize is that the patient only received an emergency operation that“cured” his incarcerated hernia but did not receive any treatment for BSL, which seemed to remain stable without worsening signs. Therefore, a conservative strategy can be selectively recommended as long as the patient’s self-perceived quality-of-life is not seriously affected.
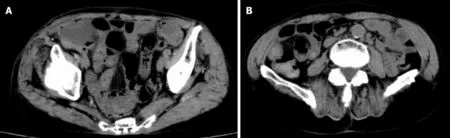
Figure 4 Computerized tomography images confirmed no recurrence of the right inguinal femoral hernia after a 1-year follow-up. A: No intestinal protrusion in the right inguinal area; B: No obvious gas accumulation in the intestinal canal.
The pathogenesis of BSL is still unclear at the present time. The disease may be caused by mitochondrial dysfunction in adipose tissue, decreased activity of cytochrome C oxidase, catecholamine-induced fat deposition or a decreased number and activity of beta adrenergic receptors[3]. Moreover, about 95% of patients with BSL have a history of heavy and long-term alcohol consumption[8]. The patient in the current case indeed had a long and continuous history of heavy alcohol drinking.Currently, there is no effective treatment for BSL, although alcohol abstinence, weight control, surgical treatment (lipotomy, liposuction) and drug therapy (fenofibrate,phosphatidyl glycerin) may be beneficial[9]. As the disease progression of BSL is slow,the early consultation rate is very low and patients often seek medical treatment due to changes in their physical appearance. In some cases, surgical procedures such as liposuction and resection[10]need to be performed in order to quickly relieve symptoms, restore appearance and/or to relieve the psychological burden.
CONCLUSION
The present case exhibits the following characteristics: (1) The patient was an elderly male and not among the femoral hernia-prone population; (2) A large amount of fat accumulation in the inguinal region led to the nonobvious signs of inguinal incarcerated femoral hernia, which had been previously missed; and (3) Fat accumulation around the surgical incision potentially increased the risk of fat liquefaction. In view of the above characteristics, we recommend that a thorough clinical history and careful physical examination be necessary for the diagnosis and surgical indication of patients who present with abdominal pain or distension, nauseavomiting and difficult defecation with obvious signs of BSL such as a neck mass or secretive symptoms such as abnormally accumulated intraperitoneal fat. Moreover,the swollen intestine trapped in the neck of the hernia sac must be intraoperatively examined for necrosis before being returned to the abdominal cavity if there is a long interval between the appearance of abdominal pain and the visit to the hospital. In addition, it is necessary for these patients to increase the frequency of dressing changes to prevent potential infection and fat liquefaction.
杂志排行
World Journal of Clinical Cases的其它文章
- Erratum: Author’s Affiliation Correction. Type II human epidermal growth factor receptor heterogeneity is a poor prognosticator for type II human epidermal growth factor receptor positive gastric cancer (World J Clin Cases 2019; Aug 6; 7 (15): 1964-1977)
- New treatment of patellar instability after total knee arthroplasty: A case report and review of literature
- Potential protection of indocyanine green on parathyroid gland function during near-infrared laparoscopic-assisted thyroidectomy:A case report and literature review
- Fanconi-Bickel syndrome in an infant with cytomegalovirus infection: A case report and review of the literature
- Incomplete Kawasaki disease complicated with acute abdomen: A case report
- Chinese patient with cerebrotendinous xanthomatosis confirmed by genetic testing: A case report and literature review